PIC Updates ‘Aluminum – Vaccine Risk Statement’ to Include Association Between Aluminum & Asthma
PIC Updates Its ‘Aluminum – Vaccine Risk Statement’: Document Includes Data on Association Between Aluminum in Vaccines and Childhood Asthma
 Physicians for Informed Consent (PIC) Updates Its ‘Aluminum – Vaccine Risk Statement’: Document Includes Data on Association Between Aluminum in Vaccines and Childhood Asthma
Physicians for Informed Consent (PIC) Updates Its ‘Aluminum – Vaccine Risk Statement’: Document Includes Data on Association Between Aluminum in Vaccines and Childhood Asthma
According to PIC, adverse effects of aluminum may not be restricted to neurological conditions*
NEWPORT BEACH, Calif., December 29, 2022 (Newswire.com) – Physicians for Informed Consent (PIC) has released an update to its Aluminum – Vaccine Risk Statement (VRS) titled “Aluminum in Vaccines: What Parents Need to Know.” The concise, two-page educational document — which serves to answer important questions about the risks of aluminum-containing vaccines — now includes important data about a study’s link between aluminum in vaccines and asthma. Asthma is a disease that affects the lungs. It causes repeated episodes of wheezing, breathlessness, chest tightness, and nighttime or early morning coughing.
Developed from data compiled by the Centers for Disease Control and Prevention (CDC), U.S. Food and Drug Administration (FDA), and the Agency for Toxic Substances and Disease Registry (ATSDR), the PIC document provides reader-friendly Q&As on topics such as:
- Why is aluminum in vaccines?
- Which vaccines contain aluminum?
- How much aluminum is in vaccines?
- Is exposure to aluminum from vaccines safe?
The document explains that both the FDA and ATSDR have raised concerns about the negative effects of aluminum exposure in humans. Scientific studies have shown that small amounts of aluminum can interfere with cellular and metabolic processes in the nervous system. Some of the most damaging effects of aluminum range from motor skill impairment to encephalopathy (altered mental state, personality changes, difficulty thinking, loss of memory, seizures, coma, and more).
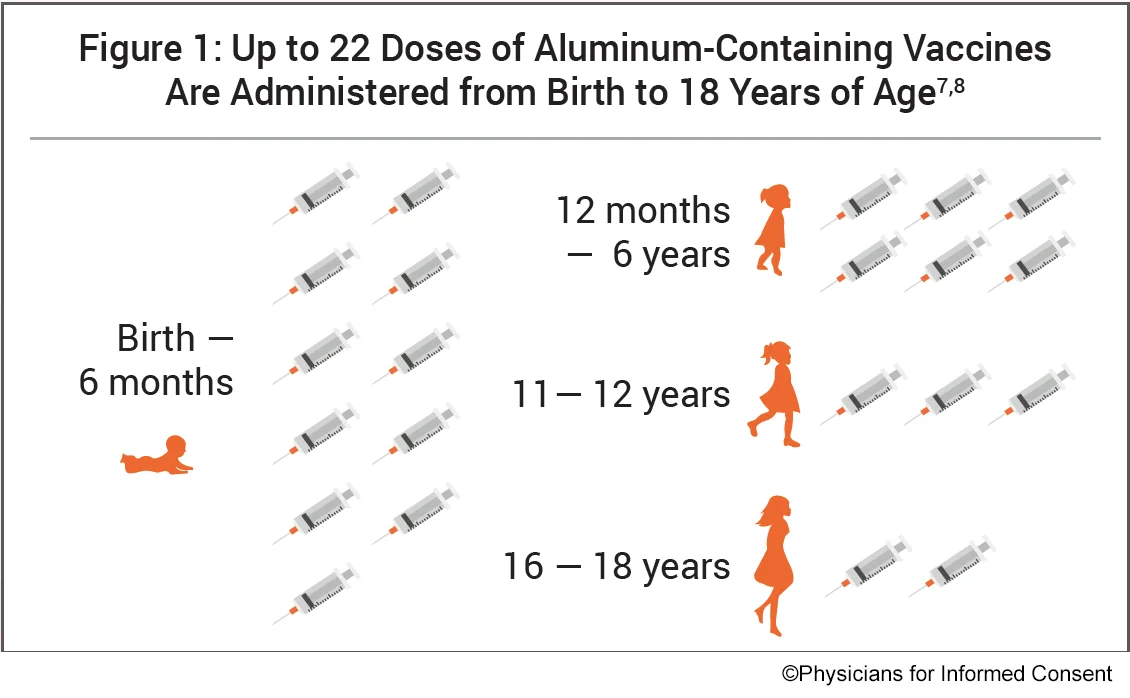
Studies have also shown that adverse effects of aluminum may not be restricted to neurological conditions.* A study referenced in the PIC document and published in Academic Pediatrics found that asthma occurred in 1 in 183 vaccinated children for every 1 mg (1,000 mcg) increase in aluminum exposure. In the United States, up to 22 doses of aluminum-containing vaccines are administered to children, with 11 doses administered from birth to 6 months of age.
“Overexposure to aluminum may lead to significant harm,” said Dr. Shira Miller, founder and president of Physicians for Informed Consent. “In California, where PIC is headquartered, since Senate Bill 277 (SB 277) was enacted in 2015, numerous doses of aluminum-containing vaccines are mandated for public and private K-12 school attendance — with no exceptions for religious or personal belief exemptions. PIC asserts that vaccine mandates are unscientific and unethical and a threat to public health. SB 277, and any other law that coerces vaccination, needs to be repealed.”
To read or download the educational document “Aluminum in Vaccines: What Parents Need to Know,” please visit physiciansforinformedconsent.org/aluminum.
* In 2008, the Agency for Toxic Substances and Disease Registry (ATSDR), a division of HHS, used studies of the neurotoxic effects of aluminum to determine that no more than 1 milligram (mg) (1,000 micrograms [mcg]) of aluminum per kilogram (kg) of body weight should be taken orally per day to avoid aluminum’s negative effects.
Physicians for Informed Consent is a 501(c)(3) nonprofit educational organization focused on science and statistics. PIC delivers data on infectious diseases and vaccines, and unites doctors, scientists, healthcare professionals, attorneys, and families who support voluntary vaccination. In addition, the PIC Coalition for Informed Consent consists of over 300 U.S. and international organizations. Click here to make a donation.
Press Contact:
info@picphysicians.org
925-642-6651
CLICK HERE to view on Newswire.
CLICK HERE to share on Twitter.
CLICK HERE to share on Facebook.
CLICK HERE to share on Instagram.
CLICK HERE to share on LinkedIn.
- https://madisonarealymesupportgroup.com/2018/08/21/aluminum-in-the-brain-in-multiple-sclerosis-regulatory-and-funding-agencies-silent-complicit/
- https://madisonarealymesupportgroup.com/2018/06/01/immunoexcitotoxicity-as-the-central-mechanism-of-etiopathology-treatment-of-autism-spectrum-disorders-a-possible-role-of-fluoride-aluminum/
- https://madisonarealymesupportgroup.com/2017/09/19/autism-aluminum-adjuvant-link-corroborated/
- https://madisonarealymesupportgroup.com/2019/09/14/autoimmune-psychosis-fingerprints-of-aluminum-induced-autoimmunity/
- https://madisonarealymesupportgroup.com/2017/09/21/aluminum-flawed-assumptions-fueling-autoimmune-disease-and-lyme/
- https://madisonarealymesupportgroup.com/2019/12/24/acute-exposure-chronic-retention-of-aluminum-in-3-vaccines-schedules-effects-of-genetic-environmental-variation/