IN NEWLY PUBLISHED PAPER, SCIENTISTS AT GLOBAL LYME ALLIANCE AND BROWN UNIVERSITY USE MATHEMATICAL MODELING TO ESTIMATE THAT MORE THAN TWO MILLION PEOPLE COULD SUFFER FROM POST-TREATMENT LYME DISEASE SYNDROME NEXT YEAR
STAMFORD, CONN (April 24, 2019)—According to a new joint study conducted by scientists at Global Lyme Alliance (GLA) and Brown University, more than two million people in the United States could suffer profound disability from post-treatment Lyme disease syndrome (PTLD) by the year 2020.
The study, published today by BMC Public Health, used advanced mathematical modeling to calculate the total number of patients with PTLD, a disorder which causes 10 to 20% of Lyme disease patients to suffer from severe symptoms long after their antibiotic treatment has ended—even if their initial infection was promptly diagnosed and correctly treated. PTLD can cause a variety of symptoms including incapacitating fatigue, chronic pain and neuro-cognitive impairment. Symptoms are often so severe that normal schedules for work, school, and personal lives are derailed.
Lyme disease has reached epidemic levels in the U.S., with an estimated 427,000 people in the U.S. newly infected every year. With timely diagnosis and antibiotic treatment most patients recover. However, researchers still do not understand why so many people remain sick months and even years after initial antibiotic treatment. Public and private insurance for the most part will not cover costs for treatment, so patients must pay medical expenses out of pocket.
About the research, lead investigator Allison DeLong, M.S., a biostatistician at Brown University’s Center for Statistical Sciences and a member of GLA’s Scientific Advisory Board, said that there were two goals of the study. Her first was to develop a rigorous mathematical framework for estimating the prevalence of PTLD in the U.S. The second was to actually calculate it to provide some projections for 2020.
“To our knowledge, this is the first time such work has been done and we felt it was time to address these deficits,” she said.
To better define the true burden of PTLD, DeLong and fellow authors based their models on U.S. Lyme disease incidence since 1980, including variables such as age, gender, life expectancy, and the estimated treatment failure rate of 10 to 20%.
“Depending on the model used, we calculated that by 2020, there could be between 81,713 to 1,944,189 individuals with PTLD in the U.S.,” said study co-author Mayla Hsu, Ph.D., Director of Research and Science at GLA, the leading 501(c)(3) dedicated to conquering Lyme and other tick-borne diseases through research, education and awareness.
Dr. Hsu said the massive number of PTLD sufferers should interest health economists studying disease burden in the U.S.
“These are substantial numbers of people struggling with chronic illness and disability,” she said. “They and their families are impacted financially, because they are often unable to work or complete their educations, and are forced to bear the medical costs themselves. This study is a vital first step toward understanding the large number of people who are suffering from PTLD.”
The study’s authors were quick to note however that as more information becomes available about Lyme incidence and the growth rate of the epidemic, new data can be added, leading to ever more precise predictions.
“This framework,” added DeLong, “will be useful now and should grow in accuracy and applicability as more data about PTLD becomes available.” Added Dr. Hsu: “This is a beginning of a vital investigative process, but by no means the last word. It reinforces the overarching need to greatly expand research that will lead to optimal treatment of these patients.”
About Global Lyme Alliance Global Lyme Alliance is the leading 501(c)(3) dedicated to conquering Lyme and other tick-borne diseases through research, education and awareness. GLA has gained national prominence for funding some of the most urgent and promising research in the field, while expanding education and awareness programs for the general public and physicians. We support those around the globe needing information about tick-borne diseases.
NOTE: The term post-treatment Lyme disease syndrome (PTLDS) refers specifically to the 10-20% of patients who were diagnosed and treated at the acute stage of their Lyme infection, yet continue to remain sick and symptomatic. Using this term is not intended to exclude anyone suffering from long-term or persistent infection. In context for this research project, it’s critical to start with a well-defined group, such as PTLDS, for study validation purposes. Due to the inaccuracies in Lyme diagnostic testing, at all stages of the disease, it’s nearly impossible to determine the entire population at this point in time. We fully acknowledge that there are more Lyme sufferers outside of the “PTLDS” category, and it’s our goal to find the answers that will help all these patients. The positive outcome of this study is that we now have a starting point to share with the medical and general communities about the substantial number of people who are suffering in the U.S. as a result of Lyme disease.
_________________
**Comment**
I had to chuckle at the disclaimer at the end. I was just about ready to send them an email until I read it.
The disclaimer reveals a problem with the 10-20% defined as PTLDS. Unfortunately, the CDC has derived a 10-20% statistic based ONLY on patients who are diagnosed and treated early that go on to develop chronic/persistent symptoms. This does NOT and should NOT include those of us who took months to years to get an accurate diagnosis and treatment. According to microbiologist Holly Ahern, that group is 30-40% of patients. When you add the two groups together, that’s a whopping 60% that go on to have remaining symptoms.
This detail is important as the 10-20% doesn’t reveal the amplitude of the problem. And for those vying for research dollars, statistics matter.
If they come up with 2 million developing chronic symptoms only from the PTLDS group (10-20%), imagine the millions upon millions affected when you count ALL of those with remaining symptoms.
Please note that the folks at Global Lyme Alliance and Brown University never state that those suffering with remaining symptoms are hopeless cases that can’t be treated. The intention of the work is to reveal the magnitude of the suffering. The Newsweek article pulls that that it can’t be treated from thin air. I’ve had long-time advocates claim it’s propaganda being used to prepare us for a new Lyme vaccine.
Did you know that the LYMERIX vaccine caused 640 emergency room visits, 34 life threatening reactions, 77 hospitalizations, 198 disabilities, and 6 deaths? In a vile cesspool of conflicts of interest are university patent holders, drug companies, and the FDA itself as another patent holder. It generated 40 million dollars before it was yanked. (2008, Drymon) http://www.yourlawyer.com/topics/overview/lymerix One doctor stated that 21 patients developed severe arthritis after receiving the LYMERIX vaccine. http://www.lymediseaseassociation.org/index.php/about-lyme/controversy/vaccine/261-lymerix-meeting “Given that Dr. Marks lead the clinical trials for Lymerix’s competitor, the OspA vaccine produced and then abandoned by Aventis Pasteur, his conclusions mean a lot. “In my opinion,” he told FDA officials, “there is sufficient evidence that Lymerix is causally related to severe rheumatologic, neurologic, autoimmune, and other adverse events in some individuals. This evidence is such as to warrant a significantly heightened degree of warnings and possible limitations or removal from marketing of Lymerix.”
https://madisonarealymesupportgroup.com/2017/01/26/lyme-vaccine-to-be-tested-on-humans/ The biological mechanism hypothesis was that the outer surface protein A (OspA), which was the antigenic component of the LYMErix vaccine,induced autoimmunity in genetically susceptible individuals, including high levels of autoantibody to OspA in their synovial fluid.
Dr. Stricker states:
Another Lyme OspA Vaccine Whitewash The meta-analysis by Zhao and colleagues comes to the conclusion that “the OspA vaccine against Lyme disease is safe and its immunogenicity and efficacy have been verified.” The authors arrive at this sunny conclusion by excluding 99.6% of published articles that demonstrate potential problems with the OspA vaccine. Furthermore, the authors ignore peer-reviewed studies, FDA regulatory meetings and legal proceedings that point to major problems with OspA vaccine safety (1-3). This whitewash bodes ill for future Lyme vaccine candidates because it fosters disregard for vaccine safety among Lyme vaccine manufacturers and mistrust among potential Lyme vaccinees.
Source:
M.M. Drymon. Disguised as the Devil: How Lyme Disease Created Witches and Changed History. (New York: With Avenue Press, 2008).
The one thing I didn’t deal with that I will point out now is this regurgitated number in the NEJM article of 10-20% of patients moving on to chronic/persistent Lyme. The following informative article written by Lorraine Johnson points out this number to be considerably higher which corresponds to my experience as a patient advocate: https://madisonarealymesupportgroup.com/2018/07/22/lyme-costs-may-exceed-75-billion-per-year/. Excerpt below:
Besides the staggering financial cost to this 21st century plague, this paper, based on estimates of treatment failure rates associated with early and late Lyme, estimates that 35-50% of those who contract Lyme will develop persistent or chronic disease.
Let that sink in.
And in the Hopkins study found 63% developed late/chronic Lyme symptoms.
For some time I’ve been rankled by the repeated CDC statement that only 10-20% of patents go on to develop chronic symptoms. This mantra in turn is then repeated by everyone else.
While still an estimate, I’d say 35 to over 60% is a tad higher than 10-20%, wouldn’t you? It also better reflects the patient group I deal with on a daily basis. I can tell you this – it’s a far greater number than imagined and is only going to worsen.
Carl Tuttle
Hudson, NH
JUL 26, 2018 — Please see the letter below addressed to Anthony S. Fauci, M.D., Director, National Institute of Allergy and Infectious Diseases (NIAID).
It would appear that the racketeering scheme to downplay the severity of Lyme disease is rampant throughout all government health agencies.
Letter to Anthony S. Fauci, M.D:
———- Original Message ———-
From: Carl Tuttle
To: Anthony.Fauci@nih.hhs.gov
Cc: catharine.paules@nih.hhs.gov, hilary.marston@nih.hhs.gov, Marshall.Bloom@nih.hhs.gov, comments@nejm.org, ddutko@hanszenlaporte.com, chris.smith@mail.house.gov, collin.peterson@mail.house.gov, jdrazen@nejm.org, info@massmed.org, president@massmed.org, mmsvp@massmed.org
Date: July 26, 2018 at 9:16 AM
Subject: Tickborne Diseases — Confronting a Growing Threat
Tickborne Diseases — Confronting a Growing Threat
Catharine I. Paules, M.D., Hilary D. Marston, M.D., M.P.H., Marshall E. Bloom, M.D., and Anthony S. Fauci, M.D. This article was published on July 25, 2018, at NEJM.org. https://www.nejm.org/doi/full/10.1056/NEJMp1807870
Excerpt:
“Although most cases are successfully treated with antibiotics, 10 to 20% of patients report lingering symptoms after receiving appropriate therapy.”
July 26, 2018
Office of the Director,
National Institute of Allergy and Infectious Diseases (NIAID),
National Institutes of Health,
Bethesda, MD 20892
Attn: Anthony S. Fauci, M.D., Director
Dear Dr. Fauci,
There has been a thirty year fixation on the acute stage of Lyme disease (with bulls-eye rash) after early treatment however patients with a prolonged exposure to the pathogen before diagnosis and initial treatment are almost always incapacitated.
You know that untreated strep throat progresses to rheumatic fever causing irreversible heart damage. What happens to the Lyme patient who went months, years or decades before diagnosis? Dr. Neil Spector required a heart transplant after his Lyme went undiagnosed for four years while his laboratory tests (serology) were repeatedly negative. [1]
Singer/songwriter Kris Kristofferson was being treated for Alzheimer’s disease when discovering he had undiagnosed Lyme disease. [2]
Autopsy results identify the destructive nature of Borrelia as evident in Vicky Logan’s liver (nutmeg liver), kidneys, heart, lungs and brain. The patient died after the insurer refused additional IV antibiotic therapy. [3]
There is a growing patient population of this class of disabled patient who has been ignored for nearly four decades. Lyme disease is a life-altering/life-threatening infection misclassified as a low-risk and non-urgent health issue through an elaborate racketeering scheme as outlined in the SHRADER & ASSOCIATES, LLP racketeering lawsuit. [4] The U.S. Centers for Disease Control has aligned themselves with the seven defendants/academics named in this RICO lawsuit.
From your article:
“Nonserologic platform technologies may also improve diagnostic capabilities, particularly in identifying emerging pathogens. Two previously unknown tickborne RNA viruses, Heartland virus and Bourbon virus, were discovered by researchers using next-generation sequencing to help link organisms with sets of unexplained clinical symptoms.”
When Sanger sequencing identified a case of chronic Lyme disease, the CDC stopped all communication with the Director of Milford Molecular Diagnostics. [5], [6]
The recently published Middelveen paper reported persistent infection as the majority of patients were culture positive for infection even after multiple years on antibiotics so there was no relief from current antimicrobials. Some patients had taken as many as eleven different types of antibiotics. [7]
_______________________
Dr. Fauci; your “Perspective” published in the New England Journal of Medicine does not mention anything I have presented here so it would appear that you are caught up in this racketeering scheme to suppress the severity of a disease that is destroying lives, ending careers, causing death and disability while leaving victims in financial ruin. There are no Public Service Announcements informing the public that you could become horribly disabled or die from Lyme disease.
It is time to move Lyme disease to HIGHEST ALERT and remove the CDC’s stronghold over the progress to find a curative approach for the late stage Lyme epidemic. [8]
Acknowledgment and response to this letter is requested.
Respectfully submitted,
Carl Tuttle
Lyme Endemic Hudson, NH
Cc: Attorney Daniel Dutko of Hanszen Laporte
U. S. Representatives Chris Smith and Colin Peterson
The conclusion is that the number of people with chronic Lyme disease likely ranges between 1 and 3 million and the annual cost—for chronic Lyme disease alone—may top $75 billion a year.
The cost is based on a study by Dr. Xinzhi Zhang, an epidemiologist who works for the Centers for Diseases Control. (Not to be confused with Dr. Ying Zhang at Johns Hopkins.)[1]
The number of people estimated to have chronic Lyme disease is based on studies of treatment failure rates for both early and late Lyme disease. Treatment failure rates range from 35% to 50%.[2-6]
Studies that show lower treatment failure rates are based on ideal diagnosis with prompt antibiotic treatment of 20 days or more, and they gauge treatment success by “objective” criteria—like resolution of a rash caused by Lyme disease.
In contrast, patients measure treatment success by whether they are restored to health—and that is the measure that we used.
Let me first give you the big picture, then I’ll drill down into the details.
The annual cost of a disease depends on how many people have it and how much it costs to treat it per year. Sounds easy enough, but there are no official counts on the number of people with late/chronic Lyme disease.
The number of people with late or chronic Lyme disease depends on how many people contract Lyme disease annually and how many of those get well or die. The CDC estimates that 300,000 cases of Lyme disease occur each year and we will work with that.[7]
(Bear in mind, though, that a recent Wall Street Journal article suggests that these numbers undercount cases in “low-incidence” states by as much as 50 times. [8])
If 300,000 people contract Lyme disease each year, how many remain ill and for how long? That depends in part on whether they are diagnosed and treated early or late.
A study by Hirsch out of Johns Hopkins suggests that as many at 40% of Lyme patients are not diagnosed early. An earlier study by Aucott found that even with early diagnosis and treatment, roughly 35% developed new-onset fatigue, 20% widespread pain, and 45% neurocognitive difficulties at six months after treatment.[6]
Of course, treatment failure rates are higher for those diagnosed late and for those with the persistent form of the disease. Treatment failure estimates in those with late/chronic Lyme disease range from 34-53% using broad demographic data with follow-up periods extending out to 4.5 years.[2, 3, 5, 9]
These estimates of treatment failure rates associated with early and late Lyme disease suggest that the prevalence range of persistent or chronic Lyme disease is between 35-50% of those who contract Lyme disease.
Once a patient has chronic Lyme disease, the question becomes “how long does it last?” The majority of patients in our published survey of over 3,000 reported that they had been ill for 10 or more years.[10] We did not ask how much longer than 10 years and so many may have been sick 15, 20 years, or more. Some might remain ill for the rest of their lives.
The last piece of information you need to determine the annual cost of chronic Lyme disease is a good estimate of the cost of the illness. For this, we turned to the CDC and an analysis conducted by Dr. Xinzhi Zhang.
His CDC study in 2002 estimated the total cost of Lyme disease at $203 million, based on the estimate of Lyme cases at that time–approximately 24,000 surveillance cases a year.
However, in 2013, the CDC dramatically increased the number of cases of estimated Lyme disease cases per year to over 300,000. That drove the annual cost of Lyme disease to exceed $3.1 billion. (See: Annual Lyme costs now top $3.1 billion–It’s time to wake up!) https://www.lymedisease.org/lymepolicywonk-annual-lyme-costs-now-top-3-1-billion-its-time-to-wake-up-2/ The increased cost reflected the CDC’s revision of case numbers from 30,000 to 300,000 and adjustments for inflation.
As it should, the CDC study estimate reflects the full societal cost of Lyme disease. This includes direct medical costs, indirect medical costs (additional medication costs), non-medical costs (e.g. travel), and loss of productivity from patients who take time from work due to illness.
The CDC study also considered both early and late/chronic Lyme disease. The direct medical costs were obtained from insurance billing information. The remaining costs were determined through patient surveys.
One of the things they found was that loss of work productivity and non-medical costs were a huge amount (over 85%) of the cost of late Lyme disease. That’s because this disease really takes a toll on patients. Many patients are unable to work entirely and others have to cut back their work hours or change the nature of their work because of the disease.[10]
Compared to the loss of work productivity in patients with chronic Lyme disease, the cost of treatment is chump change!
As I noted, the costs in the CDC study were adjusted to reflect inflation and the CDC’s revised 300,000 case estimate. But remember, the CDC study also used medical claims data for the direct medical costs. These are outdated.
Fortunately, a recent study out of Johns Hopkins by Adrion and Aucott reviewed an enormous insurance claims data base (47 million patients) and found that Lyme disease is associated with $2,968 higher total health care costs and 87% more outpatient visits over a 12 month period. [11]
Many of these early Lyme patients (63%) developed symptoms commonly associated with late/chronic Lyme disease, such as debilitating fatigue, memory loss, pain, musculoskeletal symptoms, or peripheral neuropathy.
These patients incurred $3,798 total direct medical costs associated with Lyme disease and had 66% more healthcare visits, and 89% more emergency room visits over a 12-month period.
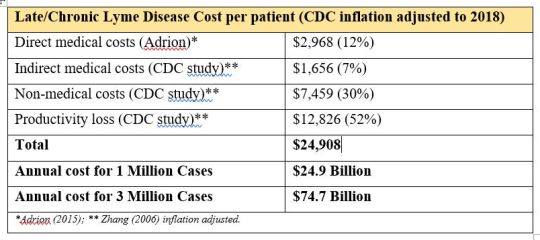
When we combine Adrion’s direct medical costs for early Lyme disease with the CDC’s inflation-adjusted indirect medical costs, non-medical costs and loss of work productivity for late/chronic Lyme disease, the total annual cost per person is about $25,000 ($24,909). See the table below.
At 1 million cases of chronic Lyme disease, the annual cost is roughly $25 billion and at 3 million cases of chronic Lyme disease, the annual cost is about $75 billion.
The same analysis can be done for early Lyme disease. Adrion’s study reported that the direct medical costs per year could be as high as $1.3 billion, using a CDC estimate of 440,000 cases per year. (CDC estimates range from 240,000 cases a year to 440,000 cases a year.)[11]
By combining these direct medical costs with the CDC’s other illness-related costs (adjusted for inflation), the total for early Lyme disease is roughly $1.11 billion based on 300,000 cases per year.
The annual cost of Lyme disease is becoming clearer, as our understanding of the number of cases and associated costs for early Lyme disease and late Lyme disease improves.
Today, the combined cost of early and late/chronic Lyme disease is between $26.1 billion and $76.6 billion dollars a year. The cost of late/chronic Lyme disease is the major component of these costs. The costs will continue to grow exponentially because they are driven by the following factors:
Too many patients are not diagnosed and treated early, when treatments are more effective;
Treatment failure rates for early Lyme disease are too high; and
Treatment failure rates for late Lyme disease are too high.
Until we address these issues in earnest, patients will continue to suffer unnecessarily and the societal costs of Lyme disease will continue to soar.
Lorraine Johnson, JD, MBA, is the Chief Executive Officer of LymeDisease.org. You can contact her at lbjohnson@lymedisease.org. On Twitter, follow her @lymepolicywonk. If you have not signed up for our patient-centered big data project, MyLymeData, please register now.
References
Zhang, X., et al., Economic impact of Lyme disease. Emerg Infect Dis, 2006. 12(4): p. 653-60.
Treib, J., et al., Clinical and serologic follow-up in patients with neuroborreliosis. Neurology, 1998. 51(5): p. 1489-91.
Shadick, N.A., et al., Musculoskeletal and neurologic outcomes in patients with previously treated Lyme disease. Ann Intern Med, 1999. 131(12): p. 919-26.
Shadick, N.A., et al. The long-term clinical outcomes of Lyme disease. A population-based retrospective cohort study. Ann Intern Med, 1994. 121, 560-7.
Asch, E.S., et al., Lyme disease: an infectious and postinfectious syndrome. J Rheumatol, 1994. 21(3): p. 454-61.
Aucott, J.N., et al., Post-treatment Lyme disease syndrome symptomatology and the impact on life functioning: is there something here? Qual Life Res, 2013. 22(1): p. 75-84.
McGinty, J., Lyme Disease: An Even Bigger Threat Than You Think A look at why cases of the tick-borne illness are undercounted, in Wall Street Journal. June 22, 2018.
Shadick, N.A., et al., The long-term clinical outcomes of Lyme disease. A population-based retrospective cohort study. Ann Intern Med, 1994. 121(8): p. 560-7.
Johnson, L., et al. Severity of chronic Lyme disease compared to other chronic conditions: a quality of life survey. PeerJ, 2014. 2, e322 DOI: 10.7717/peerj.322.
Adrion, E.R., et al., Health care costs, utilization and patterns of care following Lyme disease. PLoS ONE, 2015. 10(2): p. e0116767.
________________
**Comment**
Besides the staggering financial cost to this 21st century plague, this paper, based on estimates of treatment failure rates associated with early and late Lyme, estimates that 35-50% of those who contract Lyme will develop persistent or chronic disease.
Let that sink in.
And in the Hopkins study found 63% developed late/chronic Lyme symptoms.
For some time I’ve been rankled by the repeated CDC statement that only 10-20% of patents go on to develop chronic symptoms. This mantra in turn is then repeated by everyone else.
While still an estimate, I’d say 35 to over 60% is a tad higher than 10-20%, wouldn’t you? It also better reflects the patient group I deal with on a daily basis. I can tell you this – it’s a far greater number than imagined and is only going to worsen.
Time for every number on the CDC website to be adjusted.
BROOKLINE, Vt. – Pat Horrigan, 56, of Brookline, Vt., says he’s too sick to work. The federal government thinks he’s not sick enough to receive disability benefits.
“You don’t want to end up like me,” warned Horrigan.
In 2014, he started feeling ill.
“I was burning up. I had a real bad flu, or at least that’s what I was feeling like,” he said. “Couldn’t get my temperature down, throwing up, couldn’t hardly walk, couldn’t hardly do anything. I was just immobile on the couch.”
It wasn’t normal behavior for a Navy veteran with a lengthy resume of active jobs: from fire chief, to soccer coach to electrician.
“I’m a 110% everything I do, 10-12 hour days,” he said.
Despite never having the typical “bulls eye” rash associated with a tick-borne disease, Horrigan was tested for and diagnosed with lyme disease. He thinks he might have been bit while working on a farm baling hay.
In the four years since, he’s endured a legal battle to get what his doctors and counselors tell him he deserves.
“She said ‘let’s get you started getting disability.’ and I’m like ‘really? I didn’t know I even qualified.’ ‘Are you kidding me? Yea, you qualify and you’re a vet. Let’s see what we can do,” he remembers of a conversation early in his journey.
For the past several years, he has fought to get federal disability benefits.
He and his lawyer have continually been denied, appeal after appeal.
“John said ‘most of my clients are lucky to have one letter for a doctor. You’ve got four or five. This is like a slam dunk. You’ve got everything you need,’” he said of his lawyer’s view.
His latest motion has been pending in U.S. District Court in Vermont since September.
In the meantime, Horrigan’s been out of work and without an income. His wife went back to work as a nurse.
They moved into a corner of their daughter’s house in Brookline, Vt.
He thinks federal judges see the word “lyme” and immediately reject his claims.
“You’re sick. People stub their toes and they get disability. Something’s gotta change. They got to realize lyme is serious if you’ve got it as bad as we have it,” he said.
“To date, there’s just no evidence to suggest people have an ongoing infection like that,” said Bradley Tompkins, infectious disease epidemiologist at the Vermont Department of Health.
He, along with much of the medical community and the Centers for Disease Control and Prevention, says “chronic lyme disease” does not exist, or at least, is up for debate.
Most people diagnosed with lyme disease see their symptoms disappearance after treatment.
There is a recognized, yet rare (10-20% of patients), syndrome called Post Treatment Lyme Disease Syndrome that causes sustained symptoms for months, or up to a few years.
“It could be some sort of autoimmune response to the initial infection,” explained Tompkins. “There’s again, no evidence that there’s live bacteria that’s causing an illness and causing an infection. But there could be debris left over from the bacteria that is triggering your immune system to cause joint pain and joint swelling. So that’s what a lot of researchers are looking into now.”
“The CDC-infectious disease board have real conflicts when it comes to their potential findings on lyme disease,” said Lt. Gov. Dave Zuckerman (P/D – Vt.).
For Lt. Gov. Zuckerman, it’s personal. His wife, Rachel Nevitt, was diagnosed with lyme disease at least 6 years ago.
“She’s still only about half the person she was when I married her,” he said. “It is mentally debilitating. It is physically debilitating. It really changes your ability to function in society.”
He says it’s frustrating to hear health officials deny something he can see with his own eyes.
“Highly respected institutions, research institutions, Johns Hopkins, Stanford and others, have researchers that are really looking into this epidemic and finding that some of the research done and some of the findings done from the 90s and early 2000s is really outdated,” he said. “They’re finding a lot more instances where the lyme bacteria can survive with many of the antibacterial treatments and have ways to survive it and persist.”
Zuckerman says the onus is on the federal government to help people like his wife and Horrigan.
He adds that he pitched an idea to Governor Phil Scott (R – Vt.) last summer.
“Why don’t we work with private donors to endow a research chair at UVM Medical Center. Put UVM Medical Center in there with Johns Hopkins and Stanford, in the lyme research world, really put a bullseye for lack of a better term, on Vermont and say ‘we have a cutting edge, academic medical institution here looking at what the real issues are’ because it’s widespread in Vermont, throughout New England and the northeast,” he said.
But Pat Horrigan doesn’t have time for research. He wants change now.
“I’m blazing a trail for folks behind me because in a way I think that I am. It’s crazy. We’re sick. We need help,” he said.
This comes as lyme disease is on the rise in the region.
According to Tompkins, the Department of Health is still working through its data from 2017.
He says his department did more investigations last year than ever before, so he wouldn’t be surprised if the results show 2017 had the highest number of lyme disease cases, or close to the highest number, ever.
________________
**Comment**
And so it goes, round and round. Can’t get disability for Lyme because they say there’s no proof of infection.
https://madisonarealymesupportgroup.com/2017/12/02/scottish-doctor-gives-insight-on-lyme-msids/“If you look at major medical microbiology and infectious disease textbooks, they state that after 4 weeks you can’t find the Lyme bacteria anymore. Therefore Lyme is then categorised as ‘post infectious’. But I get back to the point I’ve made before: if you can’t culture it, you cannot know anything about its viability. You do not have a organism specific test (culture or PCR), that guides your ‘test of cure’. How do you say that a bacteria is killed, when you couldn’t grow and measure it in the first place?” “One of the rules of infectious diseases medicine is that once you stop treatment and the patient stays better, they are cured. When they get worse, the infection has returned and they have relapse of infection and need repeat treatment.My ID colleagues live by that rule with most other infections, but not with Lyme.”
LYME DISEASE, TRANSPLACENTAL TRANSMISSION AND FETAL DAMAGE
The two sides of the coin in pregnancy and LYME DISEASE
Hello friends of the network DERMAGIC EXPRESS, I bring you today another topic for what I call the “SAGA” on LYME DISEASE, in this case the controversial issue of TRANSPLACENTAL TRANSMISSION AND FETAL DAMAGE AND DEATH in pregnant women and infected with the feared BORRELIA BURGDORFERI.
I have found numerous references; most claim that BORRELIA in pregnant women with LYME DISEASE traverses the placenta and reaches the fetus and can cause multi organic damage, including the death of the same, intrauterine or a few hours or days after birth. Other authors say that this is false.
The CDC (Center of Control of Infectious Diseases) affirms that if the pregnant woman with LYME does her treatment, the child will be born healthy and recommends the use of the antibiotic AMOXICILLIN, because DOXYCYCLINE can cause damage to the developing fetus. The question here is what would happen if the BORRELIA species is resistant to AMOXICILLIN? Or the antibiotic to which BORRELIA is sensitive cannot be indicated because it would harm the fetus?
BORRELIA BURGDORFERI was discovered in 1982 by the aforementioned Willy Burgdorfer, the causal agent of the ERYTHEMA MIGRANS or LYME DISEASE, and only 1 year later the first study in 1983 described that it is suspected that this ESPIROCHETE can cross the placenta and infect the fetus, study published by Shirts SR, Brown MS, and Bobitt JR. under the name of “Listeriosis and borreliosis as causes of antepartum fever”. (8)
Later in the year 1985 Schlesinger PA, Duray PH, Burke BA, Steere AC, Stillman MT published a paper called “Maternal-fetal transmission of the spirochete of Lyme disease, Borrelia burgdorferi” where they report a case of a woman who developed LYME DISEASE and did not receive treatment with antibiotics. The child was born at 35 weeks of pregnancy and died of congenital heart disease the first week of life. The autopsy revealed the LYME ESPIROCHETE in the SPLEEN, KIDNEYS AND BONE MARROW. (2)
Later, the same WILLY BURGDORFER the discoverer and “father” of the ESPIROCHETE BORRELIA, who along with Dr. Alan Mc Donald and Jorge Benach PhD, published in the year 1987 (31 years ago) a work they called “stillbirth following maternal LYME DISEASE.” and I quote from the conclusions of these scientists: (24.)
“… Two cases of transplacental transmission of the BORRELIA BURGDORFERI were found associated with fetal death and congenital malformations, different anomalies were detected in each case …”
“… We recommend that pathologists study the tissues of stillborn fetuses in search of BORRELIA BURGDORFERI especially those with cardiac anomalies, and clinical doctors investigate the exposure during the first trimester of pregnancy to BORRELIA BURGDORFERI and in these cases determine if cardiac organogenesis is complete by the end of the first trimester of pregnancy”
“… We believe that there is enough evidence to alert women living in endemic areas of LYME DISEASE and doctors to recognize the early signs and symptoms of the disease and to start treatment with PENICILLIN at the same dose of SYPHILIS as used in pregnant women in the first trimester, regardless of the results of the laboratory tests … “
Another study that is worth noting is the one made by the MEDLINE database updated for the year of July 2012, the last revision of November 2012 of 88 journal articles from the PUBMED database, which I summarize as follows:
Maternal-Fetal Transmission of Lyme Disease
RESULTS:
1.) Mothers with active Lyme Disease,Treated: 14.6% of the pregnancies with sequelae,
2.) Untreated: 66.7% of the pregnancies with sequelae,
3.) Unknown as to treatment: 30.3% with sequelae.
4.) Specific adverse outcomes included: cardiac 22.7%, neurologic 15.2%, orthopedic 12.1%, ophthalmic 4.5%, genitourinary 10.6%, miscellaneous anomalies 12.1%, 2nd trimester demise 12.1%. Highest rate of adverse outcome (72.7%) in women with infection acquired prior to or during first trimester.)
Now I will put a summary of the most frequent clinical manifestations described in the studies of children born to mothers with LYME disease, LYME positive
COMMON SIGNS AND SYMPTOMS IN LYME POSITIVE CHILDREN:
=====================================================
1.) LOW GRADE FEVER: 59% -60%
2.) FATIGUE AND LACK OF RESISTANCE: 72%
3.) NOCTURNAL SWEATING: 23%
4.) PALE, DARK CIRCLE UNDER THE EYES: 42%
5.) ABDOMINAL PAIN: 20-29%
6.) DIARRHEA OR CONSTIPATION: 32%
7.) NAUSEA: 23%
8.) CARDIAC ANOMALIES: 23%: PALPITATIONS, (PVC) HERAT MURMUR, MITRAL VALVLE PROLAPSE
9.) ORTHOPEDIC DISORDERS: SENSITIVITY (55%), PAIN (69%) SPASMS AND GENERALIZED MUSCLE PAIN (69%), RIGIDITY AND / OR DELAY OF MOVEMENTS (23%).
10.) RESPIRATORY INFECTIONS OF THE SUPERIOR TRACT AND OTITIS: 40%
11.) ARTHRITIC DISORDERS AND PAINFUL JOINTS: 6% -50-%
12.) NEUROLOGICAL DISORDERS:
A- HEADACHES: 50%
B-) IRRITABILITY: 54%.
C-) BAD MEMORY: 39%
13.) DELAY IN DEVELOPMENT: 18%
14.) SEIZURE DISORDERS: 11%
15.) VERTIGO: 30%
16.) TIC DISORDERS: 14%
17.) INVOLUNTARY ATETOID MOVEMENTS: 9%.
18.) LEARNING DISORDERS AND HUMOR CHANGES: 80%
A-) COGNITIVE SPEAKING: 27%
B-) SPEACH DELAY: 21%
C-) READING-WRITING PROBLEMS: 19%
D.) PROBLEMS OF VOCAL ARTICULATION: 17%.
E-) PROBLEMS OF AUDITIVES / VISUAL PROCESSING: 13%
F-) WORD SELECTION PROBLEMS: 12%
G-) DYSLEXIA: 8%
19.) SUICIDAL THOUGHTS: 7%
20.) ANXIETY: 21%
21.) ANGER OR RAGE: 23%
22.) AGGRESSION OR VIOLENCE: 13%
23.) IRRITABILITY: 54% -80%
24.) EMOTIONAL DISORDERS: 13%
25.) DEPRESSION: 13%
26.) HYPERACTIVITY: 36%
27.) PHOTOPHOBIA: 40-43%
28.) GASTROESOPHAGEAL REFLUX WITH VOMIT AND COUGH: 40%
29.) SECONDARY ERUPTIONS: 23%
30.) OTHER ERUPTIONS: 45%
31.) CAVERNOUS HAEMANGIOMA: 30%
32.) OULAR PROBLEMS: POSTERIOR CATARACTS, MYOPIA, STIGMATISM, CONJUNCTIVE ERYTHEMA (LYME EYES), OPTICAL NERVE ATROPHY AND / OR UVEITIS: 30%
44.) FATIGUE AND LACK OF RESISTANCE: 72%
45.) SENSITIVITY OF SKIN AND NOISE (HYPERACUITY): 36-40%
46.) AUTISM.
There are numerous studies showing a clear EVIDENCE that the BORRELIA BURGDORGFERI in pregnant women is able to cross the placenta and infect the fetus. I could get tired here of giving you the description of each of them. But I will give you ALL the BIBLIOGRAPHIC REFERENCES that I found from the year 1983 until the year 2017, first the ones I found and then a chronology of ALL of them.
I close this issue which is HIGHLY DISCUSSED TODAY, with a post by Angélica Johansson, a great fighter against THIS PLAGUE that I found in my LINKEDIN network about the future of the planet and the LYME DISEASE … I quote:
“…”1 million people are predicted to get infected with Lyme disease in the USA in 2018. Given the same incidence rate of Lyme disease in Europe as in the USA, then 2.4 million people will get infected with Lyme disease in Europe in 2018. In the USA by 2050, 55.7 million people (12% of the population) will have been infected with Lyme disease. In Europe by 2050, 134.9 million people (17% of the population) will have been infected with Lyme disease. Most of these infections will, unfortunately, become chronic.
The estimated treatment cost for acute and chronic Lyme disease for 2018 for the USA is somewhere between 4.8 billion USD and 9.6 billion USD and for Europe somewhere between 10.1 billion EUR and 20.1 billion EUR. If governments do not finance IV treatment with antibiotics for chronic Lyme disease, then the estimated government cost for chronic Lyme disease for 2018 for the USA is 10.1 billion USD and in Europe 20.1 billion EUR.
If governments in the USA and Europe want to minimize future costs and maximize future revenues, then they should pay for IV antibiotic treatment up to a year even if the estimated cure rate is as low as 25%. The cost for governments of having chronic Lyme patients sick in perpetuity is very large….”
But what you see every day is a fight between IDSA and ILADS, CDC and others on the subject of whether it is a simple tick bite and you take an antibiotic and you cure or that it is a disease of difficult diagnosis and high cost of treatment. Between believers and non-believers to summarize. The truth is that it is spreading all over the world in leaps and bounds.
And if you have doubts that this ESPIROCHETE may or may not harm the fetus of pregnant women, cause birth defects, and many other consequences including, stillborn babies, read this “MOUNTAIN” of references that I leave here.
Approx. 25 Min.
Sue Faber, RN and Co-Founder of LymeHope speaks to pregnancy and Gestational Lyme at the LymeHope Education Event, Oakville, Ontario on November 3, 2017.
Dr. Elena Frid, a board-certified NYC neurologist and specialist in Lyme disease & other vector-borne diseases, discusses congenital Lyme disease.
**Comment** In reference to Dr. Frid’s comment that congenital Lyme is rare, I would disagree. We have not been keeping track of numbers and there are probably way more than is being acknowledged.
CONCLUSION: BORRELIA BURGDORFERI, not only transmitted by the tick bite, is TRANSMITTED by sexual contact, fluids and can also colonize the fetus of pregnant women if there is no effective treatment able to eradicate it during the same. And it is not exclusive to the Northern Hemisphere. The BORRELIA is also in the Southern Hemisphere.
2.) Maternal-fetal transmission of the Lyme disease spirochete, Borrelia burgdorferi. Ann Intern Med. 1985 Jul;103(1):67-8. [PUBMED]. Schlesinger PA, Duray PH, Burke BA, Steere AC, Stillman MT.
3.) Borrelia burgdorferi in a newborn despite oral penicillin for Lyme borreliosis during pregnancy. Pediatr Infect Dis J. 1988 Apr;7(4):286-9. [PUBMED]. Weber K1, Bratzke HJ, Neubert U, Wilske B, Duray PH.
4.) Neonatal skin lesions due to a spirochetal infection: a case of congenital Lyme borreliosis? Int J Dermatol. 1997 Sep;36(9):677-80. [PUBMED]. Trevisan G1, Stinco G, Cinco M.
5.) Confirmation of Borrelia burgdorferi spirochetes by polymerase chain reaction in placentas of women with reactive serology for Lyme antibodies. Gynecol Obstet Invest. 1996;41(4):240-3. [PUBMED]. Figueroa R1, Bracero LA, Aguero-Rosenfeld M, Beneck D, Coleman J, Schwartz I.
6.) Detection of Borrelia burgdorferi DNA in urine of patients with ocular Lyme borreliosis.
Pleyer U1, Priem S, Bergmann L, Burmester G, Hartmann C, Krause A. Br J Ophthalmol. 2001 May;85(5):552-5. [PUBMED]
7.) Culture and identification of Borrelia spirochetes in human vaginal and seminal secretions [version 1; referees: 1 not approved]. Marianne J. Middelveen1, Jennie Burke2, Eva Sapi3, Cheryl Bandoski3, Katherine R. Filush3, Yean Wang2, Agustin Franco2, Arun Timmaraju3, Hilary A. Schlinger1, Peter J. Mayne1, Raphael B. Stricker1
Source: https://f1000research.com/articles/3-309/v1 F1000 RESEARCH
8.) Listeriosis and borreliosis as causes of antepartum fever. Obstet Gynecol. 1983 Aug;62(2):256-61. [PUBMED]. Shirts SR, Brown MS, Bobitt JR.
9.) Maternal-fetal transmission of the Lyme disease spirochete, Borrelia burgdorferi.
Schlesinger PA, Duray PH, Burke BA, Steere AC, Stillman MT.
10.) Gestational Lyme borreliosis. Implications for the fetus. Rheum Dis Clin North Am 1989 Nov 15:657-77. MacDonald AB. Source: . Rheum Dis Clin North Am 1989 Nov 15:657-77
12) Lyme Borrelia positive serology associated with spontaneous abortion in an endemic Italian area.) Acta Eur Fertil. 1988 Sep-Oct;19(5):279-81. [PUBMED]. Carlomagno G1, Luksa V, Candussi G, Rizzi GM, Trevisan G.
13.) Infection with Borrelia: Implications for Pregnancy. James M O’Brien 1. and 2 Odessa P Hamidi. Division of Maternal Fetal Medicine, Pennsylvania College of Medicine, USA. Department of Obstetrics and Gynecology, Pennsylvania College of Medicine, USA.
SOURCE: http://www.smgebooks.com/lyme-disease/chapters/LD-17-05.pdf
14.) MEDLINE results for: borrelia pregnancy AND human. 88 journal articles in the PubMed
database BDH, July 2012, Latest Revision Novemb
er 2012, http://www.Huismans.de.vu
15.) Infants born to mothers with antibodies against Borrelia burgdorferi at delivery. Eur J Pediatr. 1989 Feb;148(5):426-7. [PUBMED]. Nadal D1, Hunziker UA, Bucher HU, Hitzig WH, Duc G.
17.) Congenital relapsing fever (Borrelia hermsii).Blood, 15 November 2000, Vol. 96, No. 10, pp. 3333-3333William A. Dittman. Sr, Sacred Heart Medical Center, Spokane, WA.
20.) Borreliosis during pregnancy: a risk for the unborn child?. Vector Borne Zoonotic Dis. 2011 Jul;11(7):891-8. doi: 10.1089/vbz.2010.0102. Epub 2010 Oct 6. [PUBMED]. Mylonas I1.
21.) Intrauterine transmission of Borrelia burgdorferi in dogs. Am J Vet Res. 1993 Jun;54(6):882-90. [PUBMED]. Gustafson JM1, Burgess EC, Wachal MD, Steinberg H.
22.) Fetal outcome in murine Lyme disease. Infect Immun. 1995 Jan;63(1):66-72. [PUBMED] Silver RM1, Yang L, Daynes RA, Branch DW, Salafia CM, Weis JJ.
27.) Teratogenic effects of the bacteria Borrelia sp. on the fetuses of pregnant women with Lyme disease. Sliwa, Leopold. Nowa Medycyna 04/2011. (Translation of above article)
28.) Lyme disease in pregnancy: case report and review of the literature. Obstet Gynecol Surv. 2007 Jan;62(1):41-50. [PUBMED] Walsh CA1, Mayer EW, Baxi LV.
29.) Borreliosis During Pregnancy: A Risk for the Unborn Child? VECTOR-BORNE AND ZOONOTIC DISEASES. Volume 11, Number 7, 2011. Mary Ann Liebert, Inc..DOI: 10.1089/vbz.2010.0102. Ioannis Mylonas. Source full text: http://boreliozaonline.pl/publikacje/Borelioza-w-ciazy.pdf BIBLIOGRAPHICAL REFERENCES BY CHRONOLOGY
source:
Lyme Disease and Pregnancy, Maternal Fetal Transmission of Lyme Disease:
1983 Shirts SR, Brown MS, Bobitt Jr. Listeriosis and borreliosis as causes of antepartum fever. Obstet Gynecol 1983;62:256.
1985 Schlesinger PA, Duray PH, Burke BA, Steere AC, Stillman MT. Maternal fetal transmission of the Lyme disease spirochete, Borrelia burgdorferi. (1985) Ann Intern Med, 103, 67-8.
1985 MMWR. Update: Lyme Disease and Cases Occurring during Pregnancy—United States. Vol. 34, No. 25 (June 28, 1985), pp. 376- 378, 383-384
1986 MacDonald A. Human fetal borreliosis, toxemia of pregnancy, and fetal death. Zentralbl Bakteriol Mikrobiol Hyg A. 1986 Dec;263(1-2):189-200.
1986 Burgdorfer, W., The Enlarging Spectrum of Tick Borne Spirochetoses; R.R. Parker Memorial address. Reviews of Infectious Diseases, vol.8, no.6 (Nov-Dec 1986), pp.932940
1986 Markowitz LE, Steere AC, Benach JL, et al. Lyme disease during pregnancy. JAMA.(1986); 255(24), 3394-6.
1987 MacDonald AB, Benach JL, Burgdorfer W. Stillbirth following maternal Lyme disease. N Y State J Med. 1987 Nov;87(11):615-6.
1988 Weber K; Bratzke HJ, Neubert U, Wilske B, Duray PH. (1988) Borrelia burgdorferi in a newborn despite oral penicillin for Lyme borreliosis during pregnancy. Pediatr Infect Dis J, 7:286-9.
1988 Carlomagno G, Luksa V, Candussi G, et al. (1988) Lyme Borrelia positive serology associated with spontaneous abortion in an endemic Italian area. Acta Eur Fertil 19(5), 279-81.
1988 Medici F, Benach J, Williams C. Lyme Disease during Pregnancy A Cord Blood Serosurvey. Annals New York Academy of Sciences. Volume 539, Lyme Disease and Related Disorders Pages 504–506.
1988 Health and Welfare Canada. Canada Diseases Weekly Report, June 4, 1988. Lyme disease in Canada.
1988 Lyme disease in Canada. Epidemiologic Report. CMAJ Vol. 139, Aug 1, 1988
1989 MacDonald A. Gestational Lyme borreliosis. Implications for the fetus. Rheum Dis Clin North Am. 1989 Nov;15(4):657-77.
1989 Halperin JJ., Dattwyler R., et al. A Perspective on the treatment of Lyme Borreliosis. Reviews of infectious diseases. Vol. 11 Supp 6. Sept/Oct 1989. S1518-1525
1989 Nadal D, Hunziker UA, Bucher HU, et al. (1989) Infants born to mothers with antibodies against Borrelia burgdorferi at delivery. Eur J Pediatr 148(5), 426-7.
1989 Steere et al. Lyme Seropositivity and pregnancy outcome in the absence of symptoms of Lyme disease. Scientific Abstracts June 12-17, 1989. 53 Annual Meeting of American College of Rheumatology.
1991 Lakos A. Lyme Borreliosis in Hungary in the years 1984 through 1989. Parasit hung., 24;5-51, 1991
1992 ACOG Committee Opinion. Lyme disease during pregnancy. Int J Gynecol Obstet 1992, 39; 59-60.
1992. Bracero LA, Wormser GP, Leikin E. Tejani N. Prevalence of seropositivity to the Lyme disease spirochetes during pregnancy in an epidemic area: A preliminary report. J Matern Fetal Investig. 1992(2): 265-268
1993 Hercogova J, Tomankova M, Frosslova D, Janovska D. Early-stage lyme borreliosis during pregnancy: treatment in 15 women with erythema migrans. Ceska Gynekol 58(5):229-232.
1993 Strobino BA, Williams CL, Abid S, et al. (1993) Lyme disease and pregnancy outcome: a prospective study of two thousand prenatal patients. Am J Obstet Gynecol 169(2 Pt 1), 367-74.
1994 Gasser R. et al. A Most Unusual case of a whole family suffering from late Lyme Borreliosis for Over 20 years. Angiology Vol. 45, No. 1: 85-86.
1994 Trevisan G. Lyme Borreliosis; A general survey. Acta dermatovenerologica A.P.S. Vol 3, 94, No. 1/2 4-12
1994 Elsukova LV, Korenberg EI, Kozin GA., [Pathology of pregnancy and the fetus in Lyme disease] [Article in Russian]. Med Parazitol (Mosk). 1994 Oct-Dec;(4):59-62
1995 Gardner T. Infectious Diseases of the Fetus and Newborn, 4th edition, New York, NY. W.B. Saunders Company (1995) Chapter 11, Lyme Disease. page 447 – 528.
1995 Williams CL, Strobino B, Weinstein A, et al. (1995) Maternal Lyme disease and congenital malformations: a cord blood serosurvey in endemic and control areas. Paediatr Perinat Epidemiol 9(3), 320-30.
1995 Schmidt, B. et al. Detection of Borrelia burgdorferi DNA by Polymerase Chain Reaction in the Urine and Breast Milk of Patients with Lyme Borreliosis. DIAGN MICROBIOL INFECT DIS 1995;21:121-128.
1995 Alexander, J. Cox, S. Lyme disease and Pregnancy. Infectious diseases in Obstetrics and Gynecology 3?256-261 (1995)
1996. Figueroa R. et al. Confirmation of Borrelia burgdorferi Spirochetes by Polymerase Chain Reaction in Placentas of Women with Reactive Serology for Lyme Antibodies. Gynecol Obstet Invest 1996; 41?240-243
1996. Maraspin V, Cimperman J. Treatment of Erythema Migrans during Pregnancy. Clinical Infectious Diseases 1996; 22?788-93
1997 Silver H. (1997) Lyme Disease During Pregnancy. Inf Dis Clinics of N. Amer. Vol 11, No 1.
1997 Trevisan G, Stinco G, Cinco M. Neonatal skin lesions due to a spirochetal infection; a case of congenital lyme borreliosis? International Journal of Dermatology 36; 677-99
1999 Norris C., Gardner T. Aseptic Meningitis in the Newborn and Young Infant. Am Fam Physician 1999 May 15;59(10):2761-2770
2001 Elliot D, Eppes S., Klein J. Terratogen Update; Lyme disease. TERATOLOGY 64?276 – 281 (2001)
2001 Gardner T. Chapter 11, Lyme Disease. Remington and Klein: Infectious diseases of the Fetus and Newborn, Fifth edition. New York, NY. W.B. Saunders Company 2001 pgs. 519-641
2001 Gardner T. Lyme disease in pregnancy. Program and abstracts of the 14th International Scientific Conference on Lyme Disease and Other Tick-Borne Disorders; April 21-23, 2001; Hartford, Connecticut.
2003 Goldenberg, R. L and C. Thompson (2003). “The infectious origins of stillbirth.” Am J Obstet Gynecol 189(3): 861-73.
2003 Salvato, WT, Salvato P. Lyme disease: ancient engine of an unrecognized borreliosis pandemic? Medical Hypotheses 60(5): 742-759.
2005 Onk G, Acun C, Kalayci M, Cagavi F, et al. (2005) Gestational Lyme disease as a rare cause of congenital hydrocephalus. J Turkish German Gynecology Association Artemis, 6(2), 156-157.
2005 Jones CR, Smith H, Gibb E, Johnson L (2005) Gestational Lyme Disease: Case Studies of 102 Live Births. Lyme Times. Gestational Lyme Studies 34-36
2005 Goldenberg et al. Maternal Infection and Adverse Fetal and Neonatal Outcomes. Clin Perinatol 32 (2005) 523–559.
2006 Walsh et al. Lyme disease in pregnancy. Obstetrical and Gynecological Survey. CME Review Volume 62, Number 1.
2007 Bransfield, Robert C. et al. The association between tick borne infection, lyme borreliosis and autism spectrum disorder. Medical hypotheses (2007)
2008 Hercogova J, Vanousova D. Syphilis and borreliosis during pregnancy. Dermatol Ther 21(3), 205-9.
2008 Theiler RN, Rasmussen, S. et al. Emerging and Zoonotic infections in women. Infect Dis Clin North Am 2008 December ; 22(4): 755–viii
2009 Lakos et al. Maternal Lyme borreliosis and pregnancy outcome. International Journal of Infectious Diseases 14 (2010) e494–e498
2009. Hulinska D, Votypka J, Vanousova D, Hercogova J, Hulinsky V, Drevova H, Kurzova K, Uherkova L. Identification of Anaplasma phagocytophilum and Borrelia Burgdorferi sensu lato in Patients with Erythema Migrans. Folia Microbiol. 54(3), 246-256 (2009)
2011 Mylonas I. Borreliosis During Pregnancy: A Risk for the Unborn Child? Vector Borne Zoonotic Dis. 11?891-8.
2011 Sliwa, Leopold. Teratogenny wplyw bakterii Borelli sp. Na ploy matek chorujacych na borelioze z Lyme. Zaklad Biologi Rozwoju Czlowieka. Instytus Pielegniarstwa.
2011 Sliwa, Leopold. Teratogenic effects of the bacteria Borrelia sp. on the fetuses of pregnant women with Lyme disease. Nowa Medycyna 04/2011. (Translation of above article)
2014 Onyett, H . Lyme disease in Canada: Focus on Children. Paediatr Child Health 2014;19(7):379-83
2014 OʼBrien, JM. Martens MG. Lyme disease in pregnancy; a New Jersey medical advisory. MD advisory, Winter 2014, pgs 24-27
2015 Krysztof PJ et al. Congenital tick borne Diseases: Is this an alternative route of transmission of tick borne pathogens in Mammals? Vector-Borne and Zoonotic Diseases Vol 15, Number 11, 2015.
2015 Hu LT, Tsibris AM, Branda JA. Case Records of the Massachusetts General Hospital: Case 24-2015; A 28 year-old pregnant woman with fever, chills, headache and fatigue. N Engl J Med. 2015 Jul 30;373(5):468-75.
2016 Maldonato, Y, Nizet, V, Klein, J, Remington, J, Wilson, C. Current concepts of Infections of the Fetus and Newborn Infant. Chapter 1. page 6. Infectious Diseases of the Fetus and Newborn Infant. 8th Edition. 2016
2017 OʼBrien, JM. Baum JD. Case Report. The Journal of Family Practice. August 2017; 66(8) pg E9-10 Updated and printed by JC on November 2, 2017