By Rob Verkerk PhD
Founder, executive and scientific director, ANH-Intl
Advisory Board member, Yes to Life, UK integrative cancer charity
Professor emeritus Michel Goldman MD PhD is one of Europe’s leading doctors and immunologists. He’s the founder and the President of the I³h Institute and Professor of Immunology and Pharmacotherapy at the Université Libre de Bruxelles (ULB). He’s spent a lifetime developing new drugs and has been a long-running champion of vaccines, most recently mRNA vaccines used to combat covid-19 (C19).
When he wrote a piece for Science Business in February 2021 pushing for more C19 vaccines in Europe, he wouldn’t have known his own life might be compromised by the very products he was so passionately advocating.
Five months after receiving his second of two doses of the Pfizer C19 mRNA ‘genetic vaccine’, Prof Goldman felt unwell with flu-like symptoms and swollen lymph nodes. His brother, Serge Goldman, head of the nuclear medicine department at ULB, ran a CT scan of him. That led to the diagnosis of a specific type of lymphoma, AngioImmunoblastic T cell Lymphoma (AITL).
Dr Goldman knew his immune system was going to take a hammering from chemotherapy, so he decided to get his third, ‘booster,’ jab, in the hope it might give him some protection against C19 disease should he contract the virus while undergoing treatment. But another scan just 8 days later showed the cancer had gone into overdrive – appearing like fireworks throughout much of his body on the PET/CT scan (Figure 1, right side image).
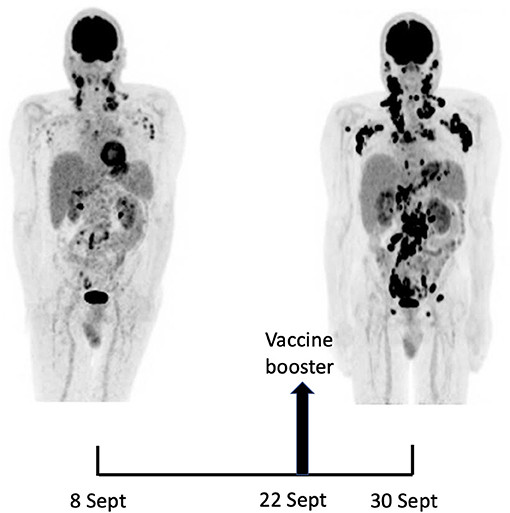
Figure 1. CT scans showing dramatic increase in nodal and gastro-intestinal lesions 8 days following Pfizer mRNA ‘booster’, compared with baseline 22 days earlier (5 months after first two Pfizer mRNA injections). Source: Goldman et al. Frontiers Med (2021).
Going public, said Goldman, seemed like the right thing to do. To this end, the two brothers, along with other colleagues, published a detailed report of Dr Goldman’s case in Frontiers Medicine, the journal for which Michel Goldman is field chief editor. The before and after booster PET/CT scans, shown above, were presented in the paper along with blood work that, among other things, showed a staggering 5.3-fold increase in a key marker for cancer in the lymph nodes, the total lesion glycolysis (TLG) index. Let’s remind ourselves that the TLG index tests were just 22 days apart, and the huge elevation was probably triggered by the booster received just 8 days previously.
The Atlantic and The Epoch Times were the main media portals to report on the case (here and here, respectively). By contrast, the mainstream media have been mute, despite the likelihood that one of their own had been taken down by their revered technology.
In their Frontiers Medicine case report, the authors state, “Within a few days following the vaccine booster, the patient reported noticeable swelling of right cervical lymph nodes“, which promoted the second, especially disturbing PET/CT scan. The authors argue the incredibly rapid progression of the cancer was likely to have been induced by the mRNA vaccines, notably the booster, through its effects on a specific mutation (RHOA G17V) in T follicular helper (TFH) cells. Considering the over 100 different forms of cancer that have been described, Goldman’s cancer, AITL, is already rare and not all patients with this cancer carry this mutation (around 75% in one study were found to be carriers). Perhaps an excuse for the medical mainstream medical community to stay largely mute?
But Goldman’s case report is one of a growing number.
Lymphoma risk is something that should be near the centre of the pharmacovigilance radar of health authorities. That’s because it’s known that the C19 jabs often causes swelling of lymph nodes (lymphadenopathy) (as in Goldman’s case, and here and here, sometimes so much so that when it occurs in a woman’s breasts it can look like breast cancer). But as Dr Goldman knows too well, there can be a very fine line between an agent that causes swollen lymph nodes and one that triggers or promotes cancer in a person’s lymph – i.e. lymphoma.
Flares of skin diseases (that may increase cancer risk) such as bullous pemphigoid received some publicity especially via new media and channels like our own during the early days of WHO declaring monkeypox as a pandemic. While bullous pemphigoid has been associated with C19 vaccination, it is an autoimmune condition, not specifically a cancer.
But a dysfunctional immune system can contribute to cancer.
Is there any evidence of a direct link between C19 genetic vaccines and skin cancer?
Six cases of recurrence of cutaneous lymphoma following C19 vaccination (also Pfizer) were described in JAMA Dermatology by a group from the Feinberg School of Medicine in Chicago, the recurrences sometimes occurring many years after remission. Two cases were reported in the Journal of the European Academy of Dermatology and Venereology and proceeded the viral vector jab by AstraZeneca. A report by Aaron Mangold and colleagues from the Mayo Clinic in Phoenix, Arizona, reported on a case of a recurrence of cutaneous lymphoma after C19 vaccination (Pfizer). But rather than suggesting caution for those with a history of it, patients are actively encouraged to take the C19 vaccines and boosters given their immune compromised state. If they are anything like Michel Goldman, they will get no benefit from the jabs, but they will expose themselves to a potential risk.
These cases published in peer reviewed journals are simply a few examples and of course represent a tiny number of cases in relation to the vast numbers of people who’ve been exposed to the injections. But how many don’t make it into these scientific publications? A reasonable assumption would be that it is the vast majority, given the travesty that has assaulted scientific free speech since the pandemic was declared in March 2020.
The scientific method, before it was derailed by a corrupt pharmaceutical industry, has long valued the importance of observation. The Big Bang theory of an expanding universe, for example, only developed serious legs after red-shifts of galaxies and stars were observed through the Hubble telescope.
Beyond peer review journals
So what of the cases being reported on the internet and social media? Should we dismiss these as medical misinformation like the social media owners themselves who probably cull most reports, but can’t stop some slipping through the net? Especially when they come off accounts with large followings, such as those of celebrities?
Hollywood stars – and fitness coaches – don’t get much more famous than Jane Fonda. After successfully battling breast and skin cancers, the actress was recently diagnosed with non-Hodgkins lymphoma. She had been covid vaccinated. Just a coincidence?
What about cervical cancer campaigner, Vicky Phelan, as an example? As a member of a ‘vulnerable group’, The Irish Times reported on her relief after she received her first jab. Then, tragically, The Daily Mail informed us she was dead. Another coincidence?
Australian boxer, Billy Dib, had been diagnosed with stomach cancer. Then came another diagnosis: aggressive non-Hodgkins lymphoma. He too had dutifully received his shots. Another anecdote, only a coincidence – surely?
If you want more anecdotes from non-celebrities, go trawl C19 vaccine injury groups on uncensored social medial channels like Telegram. The following are just some examples we picked up on Covid BC (Vax Reactions). While these heart-breaking cases should trigger concerned scientists and health authorities into deeper investigations, they are instead just ignored as worthless anecdotes by those who choose to continue not to stray into territory that might now befit the newly created version of ‘medical misinformation’. You wonder why the families of lost loved ones get so upset, only to be further ostracised and written-off as rabid ‘anti-vaxxers’. Don’t tell me we live in a world that values human dignity.

Screengrabs taken recently from the Telegram group, Covid BC (Vax Reactions) with over 25,000 members.
Is it all just coincidence?
As with any emerging phenomenon, we currently have way more questions than answers. Do cases that might be rare in relation to a specific type of cancer amount to a significant number when they’re all consolidated?
We should also be asking ourselves which of the following three scenarios we should be investigating:
- Cases of cancer initiation that appear to have arisen in previously entirely healthy people,
- Recurrence of cancer in those who appeared cancer free and had been given the ‘all clear’, or,
- Cases of cancer promotion where it appears that the vaccines may have promoted existing cancers, making them progress unusually rapidly or aggressively?
Or a combination of two or more of these?
Regrettably, we don’t have clear answers to any of these questions. But there are suggestions in the evidence available so far that the latter two scenarios might be particularly problematic in some people: namely the triggering of relapses and the aggressive promotion of existing cancers.
What’s becoming untenable scientifically is the position that there is no relationship whatsoever between this new class of genetic vaccines and cancer. The zeal by which health authorities and the medico-industrial complex are clinging to this rapidly eroding position should be a matter of concern to all of us. An unbiased scientific position should by now have centred on initiating a thorough, long-term investigation into this inevitably complex issue, clouded by a series of concurrent factors, not least of which are the backlogs in cancer patients being seen by health systems caused by lockdowns, social distancing and others measures taken by governments.
The fact that the genie is out of the bottle and it is now widely accepted that Big Pharma is intrinsically corrupt and, perversely, has become the face of socially acceptable organised crime, should be enough to wake most people out of their ‘trust the authorities’ slumber. Especially in the knowledge that mRNA technology is considered one of the most promising platforms for Big Pharma that has struggled to recover its pipelines in the wake of the blockbuster drug patent cliff that was hit good and proper around a decade ago.
Sadly, too many are still taking Big Pharma organised crime bosses for their word, perhaps concerned that if they spoke out they might be marginalised as conspiracy theorists. Put yourself in Big Pharma’s shoes and think how desperately inconvenient it would be for an unequivocal cancer-related signal to reveal itself and be publicly acknowledged. Imagine how much stock the genetic vaccine makers are likely putting behind the idea that any genuine signal for cancer initiation or promotion could be conveniently hidden under the smokescreen of cancer backlogs.
Why medics underreport cancer cases
Since the mainstream view incorrectly perceives C19 genetic vaccines as safe (and effective), mainstream oncologists who are encountering cancer cases do not typically relate cases that present to them as being linked to C19 vaccines. That’s one of the added complications of cancer – there’s always going to be significant delay involved. It’s also why, by contrast, anaphylactic or allergic reactions are normally readily admitted by vaccine makers and health authorities because they’re so obviously and temporally linked to the injections (i.e. the time delay between administration and signal is very short so making it much harder to dispel causation).
While myocarditis and pericarditis have now been added to the official list of possible side effects for Pfizer’s Comirnaty mRNA vaccine as shown on the patient information leaflets in both the USA and UK, their frequency isn’t specified, being labelled as “Not known”. Could this be interpreted as meaning, “We don’t want to tell you“?
On these patient information leaflets, the word ‘cancer’ doesn’t appear anywhere. In the minds of most practicing doctors, this translates to “there is no relationship between cancer and C19 vaccines”. Based on current data, this is an erroneous assumption, but we still need more clarity over what the strength of the relationship is and how many people and what kinds of people might be most at risk.
Many practicing medics who don’t have the time or inclination to trawl the literature and preprint servers have a false sense of confidence over the quality and completeness of the evidence base that underpins C19 genetic vaccines. They might forget that when mRNA and viral vector shots were launched in late 2020, the emerging evidence of thromboembolic (clotting), myocarditis or pericarditis risk were denied – until the data showing otherwise became indisputable.
Another major problem we have with the perception among physicians, as officially appointed gatekeepers of the public’s health, is that any apparent increases in prevalence a doctor or oncologist might encounter is likely to be put down to backlogs, which might come as no surprise given the delays in normal screening or cancer care. That’s a fair assessment, given medics have been playing ‘catch up’ given visits to doctors, hospitals and screening clinics were significantly reduced during the lockdowns of 2020 and 2021.
Most doctors also don’t have the time, sometimes also not the inclination, to review the emerging literature, some of which is beginning to suggest a possible relationship between C19 injections and increased cancer incidence. Few, as well, recognise just how hard it is to get papers published in major journals that are hellbent on supporting the narrative as they are so dependent, directly and indirectly, on research funds from pharma. It’s easier to continue to pedal the view, and in so doing not upset the apple cart, that C19 genetic vaccines are safe (see our feature last month, ‘The narrative around the safety of covid shots is cracking’).
Given that cancer is now so common, with every other person being expected to get it at some time in their life and more than one in every four people dying from it, knowing whether an agent that has been given to around 90% of the adult population is, or isn’t, driving cancer is of extreme importance.
How can we better understand what’s going on?
To help unpack the complexities we face around C19 injections and cancer, a number of different factors or possibilities need to be teased apart, as follows:
- All of the available miscellaneous reports, like that of Michel Goldman, need to be collated in one central database to help better understand both how common (or uncommon) the various supposedly rare cases of cancer initiation or progression following the different types of C19 genetic vaccination might be. From there, any patterns that help identify potential susceptibility need to be elucidated so that exposure to these ‘susceptible’ individuals can be eliminated
- We need to be able to distinguish between any cancer promotion that occurs following exposure to SARS-CoV-2, versus the vaccine, this task being made all the tougher given that the spike protein, albeit in different forms, is common to both the circulating virus and the antigen produced by the body in response to genetic instructions provided by the ‘vaccine’
- All available data need to then be put into an epidemiological framework so that the possibility of coincidence – or otherwise – can be ruled out. It’s worth remembering cancer is so common that cases will always be diagnosed in a short window post vaccination. Looking at the prevalence and type of cancer in a given population, and the nature and rapidity of its progression in relation to the pre-covid era, will provide important insights
- We also need to have a clear understanding of how many of the cancer cases we’re now seeing are caused by the delays in screening and treatment that resulted from covid-19, associated lockdowns and social isolation, and,
- Finally, we need to explore the possibility that there might be a meaningful, deeply disturbing, signal that might show that C19 vaccines are driving cancer in significant numbers of people, while understanding better the genetic and environmental backgrounds of these individuals in the event that there is such a relationship.
Sadly, this work, that requires considerable resources (especially access to data and funding) has yet to be undertaken in any kind of meaningful or comprehensive way by the scientific and medical mainstream. Those of us who are C19 vaccine skeptics are left to tentatively sound the alarm, as we did for autoimmune risks, other ‘vaccine risks (here and here), transparency – and all the other areas for which cover-ups were the default mainstream position.
The curved ball of causation
It’s increasingly being realised that disease causation (aetiology), in the case of most diseases, especially the ones that create the biggest burdens on society like cancer, is a thoroughly complex process, rather than a simple, linear one. In other words, and by way of example, the causes of cancer can’t be tracked solely to say 3, 5 or even 10 distinct causes, be they smoking, alcohol consumption, obesity, lack of physical activity, chemicals in the environment, too much or too little sunshine, infections, poor diets or specific genetic backgrounds.
While these factors may increase or decrease risk, the interplay of these factors on every individual’s unique book of genes that have in turn been modified by their environment and behaviour (epigenetics), not only during their lives to-date, but also through the epigenetically-modified genomes they have inherited from their parents, contribute to a very complex and variable picture of aetiology.
This partially explains why monotherapies don’t work very well in so many cases. In the case of cancer, poisoning cancer cells with chemicals (chemotherapy) or radiation (radiotherapy), or cutting tumours out of the body (surgery), don’t address the underlying, root causes of the imbalances that contributed to the disease. Yet these modalities still remain the primary treatments for cancer today, with the global oncology drugs market being valued at US$135 billion in 2020, and set to double by 2030. The global radiology market, by comparison, was around one-twentieth of the size, being valued in 2020 at a little under US$7 billion.
So, recognising that cancer initiation or mediation is a complex multi-factorial and often delayed process means that trying to pin blame (causation) on a single agent is incredibly difficult, or even impossible. That’s one of the reasons why, despite billions having been spent on research over many decades, we have only a small list of 122 recognised human carcinogens, as collated by the International Agency on Research on Cancer (IARC). Putting naturally-occurring substances and compounds to one side given these have always been part of our background exposure during the course of our species’ evolution, there are a staggering 350,000 industrial chemicals that are globally approved for production and use. Over a third of these cannot be explicitly identified in order to protect intellectual property or because their composition is too complex to be understood. So much for transparency and putting the protection of the interests of industry ahead of the public or environment.
This kind of complexity provides the ‘perfect storm’ in which to conceal or deny a cancer promotion effect for many months or even years. Until such time as the evidence becomes so overwhelmingly obvious it can no longer be concealed from public view.
Let’s look at the bigger picture
So how do we get under the bonnet of this sticky issue for which we’ve been hearing evidence that’s dismissed as anecdote for close on a year, and for which there is an increasing trickle of published case reports and social media anecdotes?
The starting point is to look at population-wide patterns in cancer related prevalence and mortality and try to account for the proportion that might be related to backlogs. Until very recently, in late 2022, national cancer data for 2021 (the year C19 vaccine roll-out started in earnest) were not generally released into the public domain, no doubt staff shortages linked to the pandemic being the official explanation.
But we’re at last able to get some access to national data. Having seen that official data can be subject to manipulation seemingly in order to conceal disturbing trends, we shouldn’t necessarily treat these data as ‘gospel’. Among the most important work showing up how data can be deliberately or unwittingly fudged, is the extensive work of Prof Norman Fenton’s group at Queen Mary University of London who showed how UK Office for National Statistics (ONS) data, that was widely viewed as among the most reliable, had been manipulated. In this case, the data made the injections look much better than they were. If these are the only population data we have, we have no option but to take them at face value.
The UK National Health Service (NHS) Systemic Anti-Cancer Therapy COVID-19 Dashboard offers an overview of the number of people who have been receiving cancer treatments in the NHS since the covid-19 pandemic was announced. Delays in receiving data from NHS Trusts was, perhaps surprisingly, not as delayed in 2021 as it has been in 2022, which raises some interesting questions in itself.
There was a predictable and marked reduction in treatments between March and June 2020 during the first wave of covid-19 (Fig. 1) that caused many hospitals to dramatically change and dial back their normal operation.
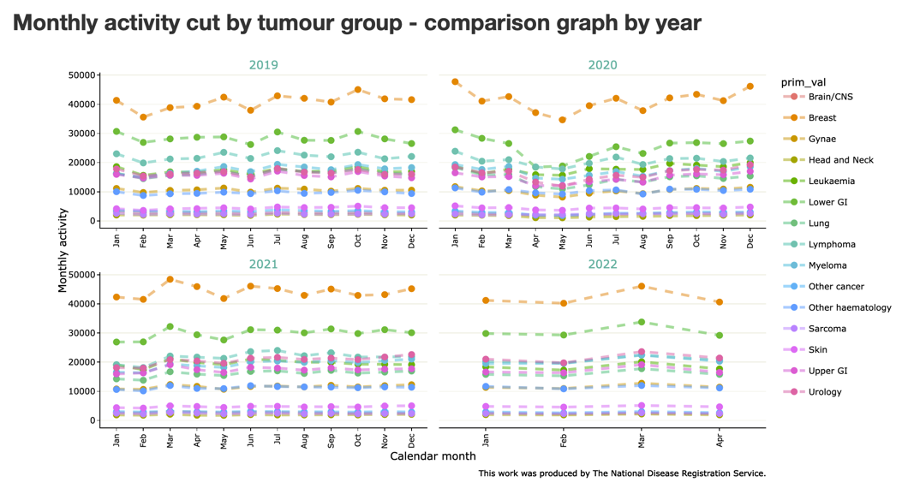
Figure 1. UK National Health Service (NHS) Systemic Anti-Cancer Therapy COVID-19 Dashboard summaries. Note drop in cancer treatments between March-June 2020 linked to the first pandemic wave.
Following this, there is an uptick in treatments over many types of cancer, that can best be seen by clicking through successive months in the drop-down menus of the comparison tables (2019 vs 2020, 2021 vs. 2019/2020, 2022 vs. 2020/2021) of the ‘Monthly Activity + sub-population breakdown’ tab.
Some cancers and months really stand out, such as those affecting the urological system (~140% uptick in prevalence), but there is no easy way of clearly separating out backlog ‘catch-up’ effects from a potential additional signal from the C19 vaccines. As cancer specialist Prof Karol Sikora says in his UnHerd’s Post from last Monday, “the lockdown cancer wave has only just begun”. News is out suggesting Europe will be facing a “cancer epidemic” because 1 million cases were missed owing to reduced access to healthcare during the pandemic. Is this another cloud that will be used to disguise any potential contribution by C19 vaccines?
Given we can’t access any crystalline data on the subject, what clues in the data might we be looking for if such a C19 vaccine/cancer signal was present? One expectation might be that the numbers that were elevated from backlogs should start to orientate back towards normality (pre-pandemic levels, as per 2019). For many types of cancer they don’t do this – but you can’t see this from any of the summary tables for the first 4 available months of 2022 as NHS Digital has seen fit to not provide summary tables that let you compare 2022 with 2019.
Turning to the Scottish data – there are some interesting insights. Is, for example, the consistently raised prevalence of prostate cancer (Fig. 2) only down to backlogs, given there is no apparent trend towards 2019, pre-pandemic levels?
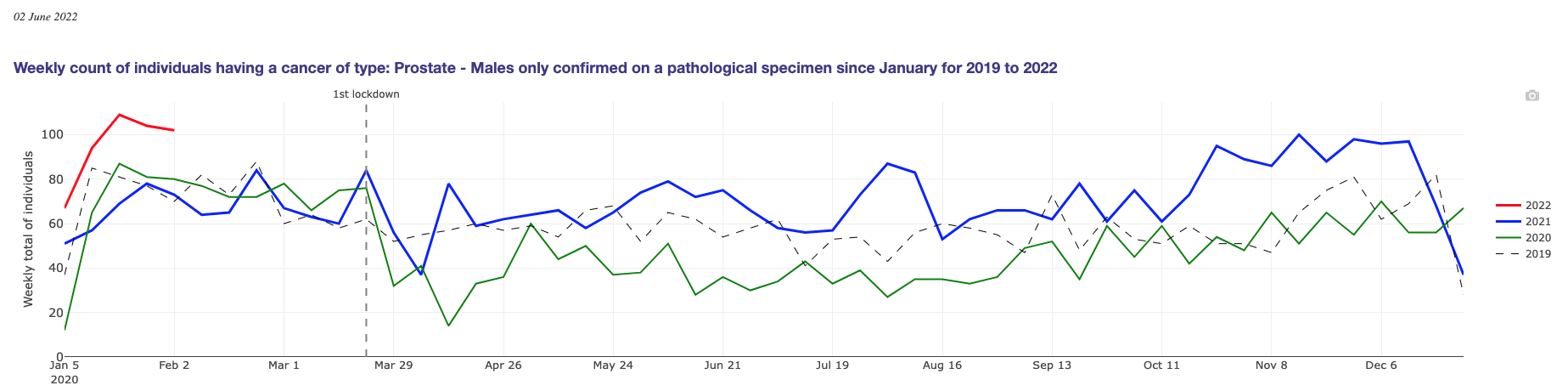
Figure 2. Official data from Public Health Scotland COVID-19 wider impacts on the health care system dashboard
The jury is out
Yes, although the jury may be out in terms of being able to point to unequivocal data showing a relationship, the facts suggest not commissioning an independent jury to investigate this complex and confounded issue would be socially irresponsible (what’s new?). We could sit back and trust the authorities and even the mainstream journals that have published papers saying ‘no need to worry about the jabs and cancer’ (such as here and here).
But these have been wrong on many prior occasions. For an ever growing number of us, any trust of the establishment in such matters, unfortunately, dissipated long ago.
There are more than adequate data to suggest both a motive (profit) and a potential mechanism (widespread evidence of immune system dysregulation).
We would be doing our fellow humans a disservie if we ignored the possibility of a smoking gun. This task being made all the harder given the cloud created by ‘pandemic backlogs’ that you should expect to hear a lot about. It wouldn’t be the first corporate cover-up, but it may be the biggest.
We will continue to track the data and share more as it becomes available.
© [2022] Alliance for Natural Health International. This work is reproduced and distributed with the permission of The Alliance for Natural Health International.
________________
For more: