Get Sicker: Anatomy Of A Failed Policy
https://trialsitenews.com/get-sicker-anatomy-of-a-failed-policy/
Get Sicker: Anatomy Of A Failed Policy

By Mary Beth Pfeiffer
Twenty-seven-year-old Ankit Dubey was sick and terrified. He could hear sirens blaring across Lucknow, his home in northern India. He had been warned away from hospitals. People in his middle-class neighborhood were dying.
This second COVID wave was nothing like the first in 2020. This was Armageddon, “a horror movie,” he said, that lasted through April and May of 2021. He had thought lockdowns had spared India the chaos he had seen on TV from New York and Rome. He was wrong. “We went through hell,” he said.
Dubey told me his story because he wants the West to understand, to know. He, his parents, 56 and 65, and brother, 30, all four sick, were spared death, thankfully, but also painful and prolonged illness. How? They got treated early with a combination of safe generic drugs: azithromycin, doxycycline, and another he had never heard of: ivermectin. Other Indians tell similar stories.
India has been cast as a COVID failure with a struggling health-care system and spotty access to vaccines. But despite those two realities, India quelled a vicious Delta wave by making a key choice. Most of its states, led by 240-million population Uttar Pradesh where Dubey lives, opted to treat COVID early. The United States, Canada, the United Kingdom and most of Europe have not. They can learn from Ankit Dubey’s story. (See link for article)
_________________
**Comment**
“Get Sicker” is exactly the MO of our corrupt public health ‘authorities’ regarding Lyme/MSIDS as well.
You may recognize the author of the article. She’s a Lyme/MSIDS sufferer as well and has written about the plight of Lyme patients. Unfortunately, she has bought the lie and written a book that ‘climate change’ is what is driving tick and disease proliferation. I have it on good authority from an expert, independent tick researcher, also a patient, that this is just not the case. Similarly to what we are going through now with COVID, our government is well versed in utilizing ‘slight of hand’ tactics, quite similar to magicians, to get us concentrating and looking in one area while they perform their tricks in another area. They are firmly behind both the COVID debacle and the Lyme/MSIDS debacle – causing both, with severe conflicts of interest and owning patents on nearly every aspect of both diseases.
Summary of article:
- Patients in the U.S. are offered nothing to treat COVID early and despite its failure, are only offered ventilators when cases become severe.
- Some of these patients worsen needing hospital care due to a cytokine storm.
- U.S. patients have had hospital staff whisper that ivermectin works, but that “their hands are tied.” A nurse stated, “When we used to prescribe it, everybody was walking out alive.”
- When a terminal COVID patient asked for ivermectin his doctor stated, “You might as well drink bleach.” Another practitioner called it “witchcraft.”
- The two U.S. patients needing hospital care in the article had ivermectin smuggled in to the hospital and miraculously, after a hard fight, got the hospitals to give it to them.
- The change was ‘180 degrees,’ and they both lived to tell the tale.
- We are being told there is no early treatment. THIS IS A LIE.
- People have died needlessly and government is complicit.
Important quote:
“It embarrasses me for what we have done in the U.S. in terms of this management,” Dr. Mobeen Syed, a medical educator with 395,000 YouTube subscribers, told me when we spoke of ivermectin for this article. “It embarrasses me that even though we have drug that is safer than Tylenol, we have made people resort to taking horse paste or animal products. We have done this to Americans.”
- A data analyst researching pandemic trends makes a dire prediction: as the weather cools and people move indoors – the highly vaccinated states in the north are going to face a COVID catastrophe. He states only early treatment can stop it.
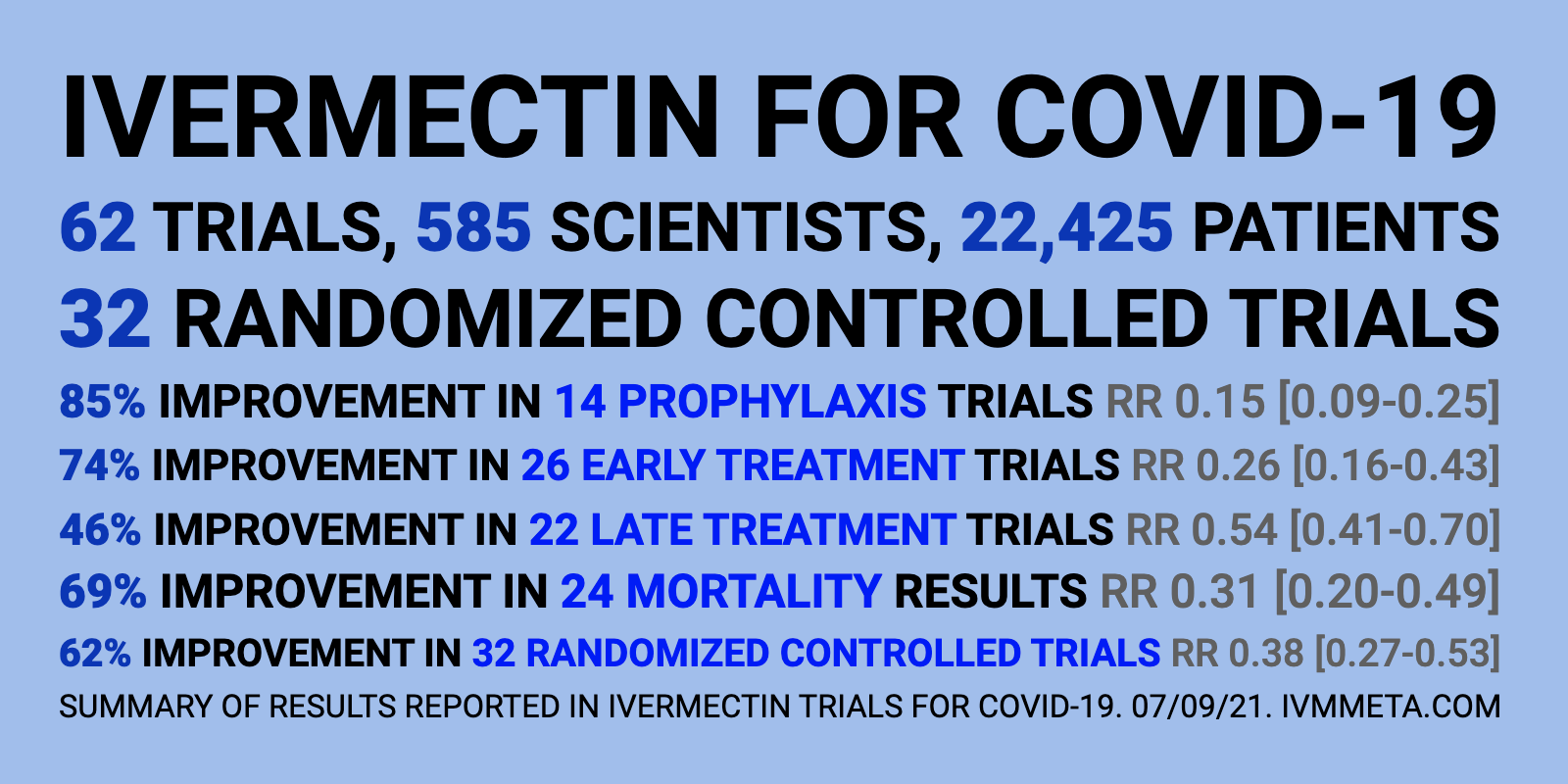
- This same analyst has documented ivermectin’s impact globally and found ivermectin has reduced hospitalizations dramatically.
- In the U.S.; however, there is willful ignorance and demonization of ivermectin and early treatment, but speedy acceptance of ineffective and toxic drugs like remdesivir, and the belief that ‘vaccines’ are the only way out.
- Emergency Use Authorization (EUA) for a fast-tracked, experimental mRNA ‘vaccine’ only works if, “there are no adequate, approved, and available alternatives.”
- The media is enabling censorship and fostering COVID fiction that treating COVID is a “right-wing” construct. They also dismiss ‘vaccine’ side effects and continue to call them ‘rare.’
- Countries are caving to the U.S.-hatched COVID fiction.
- Doctors’ licenses are being threatened, and reputations imperiled over using early treatments like ivermectin.
- There were more than 500 deaths in the first year of remdesivir usage.
- There have been 20 deaths in 19 years of ivermectin usage.
- The FDA, spurred by “multiple” reports of ivermectin ‘poisoning,’ lied when it put out a post on it causing “serious harm, seizures, coma, and even death”. When the author inquired on how many is “multiple,” she was told FOUR. Yet, the FDA had no trouble approving remdesivir which has caused far more deaths.
- CDC also bad-mouthed ivermectin and pushed the “calls to the poison control center” narrative. The problem is they give no data to support this claim.
- In India, ivermectin is a house-hold name and easily available for about $2 at the nearest drug store. People there no longer fear COVID. They simply treat it.
The article discusses India’s successful usage of ivermectin for COVID. I’m also happy to report that there is an Awaken India Movement which shares resources and brings people together who desire freedom of choice and basic human rights. The group demands no lockdowns, no mandatory masks, no mandatory social distancing, no mandatory testing, no mandatory vaccines, no GMO foods, no 5G, no tech censorship, no new normal, and no great reset.
This movement undoubtedly stems from the history of Bill Gate’s usage of India as his laboratory for his vaccine ventures in victimizing poor children, which was documented by filmmaker Mikki Willis in his 2020 documentary, Plandemic. You can watch the section on Bill Gates with English subtitles here, and with Hindi subtitles here.
Independent journalist Ben Swann also interviewed Mr. Willis to discuss the section of his documentary on India, and how much of what evil Bill Gates did in India regarding vaccine trials has been scrubbed from the Internet.