Dr. Richard Urso discusses scientifically unsupported lockdowns, which are causing excess deaths, and the seasonal nature of Covid-19. (Jan. 22, 2021)
(01:04) Covid-19 is a seasonal illness
(02:35) Experts arguing lockdowns cause deaths, suicides, mental health issues…
(03:22) Businesses shut down and newly created reliance on govt
(03:47) Vaccine passports
(04:29) Lockdown caused poverty and connection to health and illness
(04:59) Great Barrington Declaration
(05:35) Lockdowns not supported by science
(05:51) Fear and PCR tests
(06:15) Covid-19 diagnosing protocol changed to include clinical diagnosis after Biden elected president
DR. RICHARD URSO (PART 4): COVID-19 TREATMENT EXISTS & CONFLICTS OF INTEREST (9:16)
Dr. Richard Urso discusses successful treatment protocols, including hydroxychloroquine and iverectin, that have always been available and are purposely being ignored for political and financial conflicts of interest within the FDA, CDC and NIH. (Jan. 22, 2021 interview.)
Dr. Urso has successfully treated 200+ Covid-19 patients and prophylaxed 400+ people using various treatment protocols.
(00:40) Drug treatment protocols
(05:04) Treating his first Covid-19 patient
(05:55) Go to outpatient drugs
(06:28) Covid-19 prophylaxis
(06:57) Why has the FDA not approved certain drugs used in the treatment of Covid-19?
(07:38) Conflicts of interest within FDA, CDC and NIH
(08:50) Part 5 preview: Vaccines
On Monday, September 6, 2021, the Cincinnati judge, Michael A. Oster, Jr., ruled that West Chester hospital would be allowed to discontinue giving ivermectin to their patient, Jeffrey Smith, after the initial ruling compelled the hospital to give Mr. Smith the drug for 14 days.
“But for me, the most disturbing issue is that the hospital itself—after telling Julie Smith, Jeffrey’s wife, that they had tried everything to recover her husband and could do nothing more for him—refused to try ivermectin,” said Dr. Wagshul.
According to the U.S. Centers for Disease Control and Prevention, people who got the COVID shot early are now at increased risk for severe COVID disease
This may be a sign that antibody dependent enhancement (ADE) is occurring, or it may simply indicate that the protection offered is limited to a few months, at best
Recent research warns the Delta variant “is posed to acquire complete resistance to wild-type spike vaccines.” This could turn into a worst-case scenario that sets up those who have received the Pfizer shots for more severe illness when exposed to the virus
To “stay ahead of the virus,” the Biden administration is now considering recommending a booster shot five months after the initial two doses rather than waiting eight months, as previously suggested
Israeli data show Pfizer’s shot went from a 95% effectiveness at the outset to 39% by late July 2021, when the Delta strain became predominant. The U.S. Food and Drug Administration’s expectation for any vaccine is an efficacy rate of at least 50% compared to placebo
The official COVID-19 vaccine narrative changes rapidly these days. It took just one month for it to go from “if you’re vaccinated you’re not going to get COVID,”1 including the Delta variant,2 to “people who got vaccinated early are at increased risk for severe COVID disease.”3
From the get-go, I and many other medical experts have warned of the possibility of these shots causing antibody dependent enhancement (ADE), a situation in which the shot actually facilitates a cascade of disease complications rather than protects against it. As a result, you may suffer more severe illness when encountering the wild virus than had you not been “vaccinated.”
While we don’t yet have definitive proof that ADE is occurring, we are seeing suspicious signs that it might be. Data showing those who got the shot early this year are now at increased risk of severe infection could be such a sign. At bare minimum, it’s an indication that the protection you get from these shots is very temporary, lasting only a few months.
This makes sense when you consider they program your body to produce just one type of antibody against a specific spike protein. Once the spike protein, or other elements in the virus, starts to mutate, protection radically diminishes. Worse, the vaccine facilitates the actual production of the variants because it is “leaky” and provides only partial ineffective immune protection.
Natural immunity is far superior, as when you recover from the infection, your body makes antibodies against all five proteins of the virus, plus memory T cells that remain even once antibody levels diminish. This gives you far better protection that will likely be lifelong, unless you have impaired immune function.
Real-world data from Israel confirms this, showing those who have received the COVID jab are 6.72 times more likely to get infected than people with natural immunity.4,5,6
CDC Admits ‘Vaccine’ Immunity Doesn’t Last
In an August 20, 2021, report, BPR noted:7
“’The data we will publish today and next week demonstrate the vaccine effectiveness against SARS COVID 2 infection is waning,’ the CDC director [Rochelle Walensky] began … She cited reports of international colleagues, including Israel ‘suggest increased risk of severe disease amongst those vaccinated early.’
Fear not, the same people who tried to sell Americans immunity through a jab and promised to hand back the freedoms they impeded on have a plan, and they’re not leaving much room for personal choice.
‘In the context of these concerns, we are planning for Americans to receive booster shots starting next month to maximize vaccine induced protection. Our plan is to protect the American people and to stay ahead of this virus,’ Walensky shared …
The CDC director appears to all but admit that the vaccine’s efficacy rate has a strict time limit, and its protections are limited in the ever-changing environment.
‘Given this body of evidence, we are concerned that the current strong protection against severe infection, hospitalization and death could decrease in the months ahead. Especially among those who are higher risk or those who were vaccinated earlier during the phases of our vaccination roll out,’ Walensky explained …
Starting September 20, Americans who completed their two doses of the Pfizer or Moderna vaccine at least eight months ago will be eligible for a booster shot. The goalposts back to a ‘normal’ society continue to be moved further and further. When will Americans, especially those who complied with initial vaccinations, have had enough?”
Data Reveal Rapidly Waning Immunity From Shots
Indeed, Israeli data show Pfizer’s shot went from a 95% effectiveness at the outset, to 64% in early July 2021 and 39% by late July, when the Delta strain became predominant.8,9 Meanwhile, the U.S. Food and Drug Administration’s expectation for any vaccine is an efficacy rate of at least 50%.
Pfizer’s own trial data even showed rapidly waning effectiveness as early as March 13, 2021. BMJ associate editor Peter Doshi discussed this in an August 23, 2021, blog.10
By the fifth month into the trial, efficacy had dropped from 96% to 84%, and this drop could not be due to the emergence of the Delta variant since 77% of trial participants were in the U.S., where the Delta variant didn’t emerge until months later. This suggests the COVID shot has a very temporary effectiveness regardless of new variants.
What’s more, while Israeli authorities claim the Pfizer shot is still effective at preventing hospitalization and death, many who are double-jabbed do end up in the hospital, and we’re already seeing a shift in hospitalization rates from the unvaccinated to those who have gotten one or two injections. For example, by mid-August, 59% of serious COVID cases were among Israelis who had received two COVID injections.11
Vaxxed Over Age 50 at Increased Risk for Serious Infection
Data from the U.K. show a similar trend among those over the age of 50. In this age group, partially and fully “vaccinated” people account for 68% of hospitalizations and 70% of COVID deaths.12
80% of COVID Hospitalizations in Massachusetts Were Vaxxed
Data13 from the U.S. Centers for Disease Control and Prevention also raise questions about the usefulness of the COVID shots. Between July 6 and July 25, 2021, 469 COVID cases were identified in a Barnstable County, Massachusetts, outbreak.
Of those who tested positive, 74% had received two COVID injections and were considered “fully vaccinated.” Even despite using different diagnostic standards for non-jabbed and jabbed individuals, a whopping 80% of COVID-related hospitalizations were also in this group.14,15
The CDC also confirmed that fully vaccinated individuals who contract the infection have as high a viral load in their nasal passages as unvaccinated individuals who get infected, proving there’s no difference between the two, in terms of being a transmission risk.16
If vaccination status has no bearing on the potential risk you pose to others, why do we need vaccine passports? According to Harvard epidemiologist Martin Kulldorff, this evidence demolishes the case for passports.17 They clearly cannot ensure safety, as evidenced by outbreaks where the vaccination rate was 100%. Examples include outbreaks onboard a Carnival cruise liner18 and the HMS Queen Elizabeth, a British Navy flagship.19
Study Predicts Pfizer Shot Will Enhance Delta Infectivity
A study20 posted August 23, 2021, on the preprint server bioRxiv now warns the Delta variant “is posed to acquire complete resistance to wild-type spike vaccines.” This could essentially turn into a worst-case scenario that sets up those who have received the Pfizer shots for more severe illness when exposed to the virus. As explained by the authors:21
“Although Pfizer-BioNTech BNT162b2-immune sera neutralized the Delta variant, when four common mutations were introduced into the receptor binding domain (RBD) of the Delta variant (Delta 4+), some BNT162b2-immune sera lost neutralizing activity and enhanced the infectivity.
Unique mutations in the Delta NTD were involved in the enhanced infectivity by the BNT162b2-immune sera. Sera of mice immunized by Delta spike, but not wild-type spike, consistently neutralized the Delta 4+ variant without enhancing infectivity.
Given the fact that a Delta variant with three similar RBD mutations has already emerged according to the GISAID database, it is necessary to develop vaccines that protect against such complete breakthrough variants.”
Proactive Use of COVID Shots Drive Dangerous Mutations
It’s now clear that early warnings against mass vaccination during an active outbreak are being realized. It’s not the unvaccinated that are driving mutations; it’s the vaccinated, as the injections simply do not prevent infection.
The end result, if we keep going, will be a treadmill of continuous injections to keep up with the merry-go-round of waning effectiveness in general combined with the emergence of vaccine-resistant variants. As reported by Live Science:22
“Vaccine-resistant coronavirus mutants are more likely to emerge when a large fraction of the population is vaccinated and viral transmission is high … In other words, a situation that looks a lot like the current one in the U.S.
The mathematical model,23 published July 30 in the journal Scientific Reports, simulates how the rate of vaccination and rate of viral transmission in a given population influence which SARS-CoV-2 variants come to dominate the viral landscape …
If viral transmission is low, any vaccine-resistant mutants that do emerge get fewer chances to spread, and thus, they’re more likely to die out, said senior author Fyodor Kondrashov, who runs an evolutionary genomics lab at the Institute of Science and Technology Austria.”
These findings come as no surprise to those familiar with previous research showing the same exact thing. As explained in “Vaccines Are Pushing Pathogens to Evolve,” published in Quanta Magazine,24
“Just as antibiotics breed resistance in bacteria, vaccines can incite changes that enable diseases to escape their control.”
The article details the history of the anti-Marek’s disease vaccine for chickens, first introduced in 1970. Today, we’re on the third version of this vaccine, as within a decade, it stops working. The reason? The virus has mutated to evade the vaccine. As a result of these leaky vaccines, the virus is becoming increasingly deadly and more difficult to treat.
A 2015 paper25 in PLOS Biology tested the theory that vaccines are driving the mutation of the herpesvirus causing Marek’s disease in chickens. To do that, they vaccinated 100 chickens and kept 100 unvaccinated. All of the birds were then infected with varying strains of the virus. Some strains were more virulent and dangerous than others.
Over the course of the birds’ lives, the unvaccinated ones shed more of the least virulent strains into the environment, while the vaccinated ones shed more of the most virulent strains. As noted in the Quanta Magazine article:26
“The findings suggest that the Marek’s vaccine encourages more dangerous viruses to proliferate. This increased virulence might then give the viruses the means to overcome birds’ vaccine-primed immune responses and sicken vaccinated flocks.”
Vaccinated People Can Serve as Breeding Ground for Mutations
Before 2021, it was quite clear that vaccines push viruses to mutate into more dangerous strains. The only question was, to what extent? Now all of a sudden, we’re to believe conventional science has been wrong all along. Here’s another example: NPR as recently as February 9, 2021, reported that “vaccines can contribute to virus mutations.” NPR science correspondent Richard Harris noted:27
“You may have heard that bacteria can develop resistance to antibiotics and, in a worst-case scenario, render the drugs useless. Something similar can also happen with vaccines, though, with less serious consequences.
This worry has arisen mostly in the debate over whether to delay a second vaccine shot so more people can get the first shot quickly. Paul Bieniasz, a Howard Hughes investigator at the Rockefeller University, says that gap would leave people with only partial immunity for longer than necessary.”
According to Bieniasz, partially vaccinated individuals “might serve as sort of a breeding ground for the virus to acquire new mutations.” This is the exact claim now being attributed to unvaccinated people by those who don’t understand natural selection.
It’s important to realize that viruses mutate continuously and if you don’t have a sterilizing vaccine that blocks infection completely, then the virus mutates to evade the immune response within that person. That is one of the distinct features of the COVID shots — they’re not designed to block infection. They allow infection to occur and at best lessen the symptoms of that infection. As noted by Harris:28
“This evolutionary pressure is present for any vaccine that doesn’t completely block infection … Many vaccines, apparently, including the COVID vaccines, do not completely prevent a virus from multiplying inside someone even though these vaccines do prevent serious illness.”
In short, like bacteria mutate and get stronger to survive the assault of antibacterial agents, viruses can mutate in vaccinated individuals who contract the virus, and in those, it will mutate to evade the immune system.
In an unvaccinated person, on the other hand, the virus does not encounter the same evolutionary pressure to mutate into something stronger. So, if SARS-CoV-2 does end up mutating into more lethal strains, then mass vaccination is the most likely driver.
What NFL Outbreak Can Tell Us
As reported August 27, 2021, by MSN,29 as players were encouraged to get the COVID shot for everyone’s safety, separate testing rules were put into place. Players who have gotten the jab only need to test every two weeks, while unvaccinated players undergo daily testing.
The relaxed testing requirement for double-jabbed players was used as incentive to go ahead and get the shot. As reported by MSN, “Conversely, the continued daily testing would become part of a punitive system that would make life so annoying for the unvaccinated that they would eventually get on board.”30
Well, this didn’t work out as planned. Nine Titans players and head coach Mike Vrabel have now tested positive, showing it really doesn’t matter if you’re double-jabbed or not. The infection spreads among the vaxxed just the same. As noted by MSN:31
“The pandemic is in a phase where the unvaccinated are facing the vengeance of a more aggressive strain of COVID-19. It’s also an era when the vaccinated are grappling with the reality that their shots are mitigating their symptoms and medical complications, but not completely preventing them from becoming infected or transmitting COVID to others.”
To remedy the matter, the NFL Players Association, the union representing players of the National Football League, is now calling for a return to daily testing of all players, regardless of COVID jab status. Time and again, we find that incentives fall far short of their initial promise. This has been the case for masks as well.
First, we were told that if we got the COVID shot, we didn’t need to wear masks anymore. Of course, universal mask recommendations returned full force when it became apparent that breakthrough infections were still occurring at a surprising rate.
Now, routine testing with a test known to produce false positives at a rate of about 97%32 is promoted again, regardless of injection status, and there’s no reason to assume the same won’t happen with vaccine passports. We’re promised freedom if we give up medical autonomy, but freedom will never actually be granted. They’ll just continue to move the goal post.
It is highly likely, in fact even predictable, that despite its dramatic ineffectiveness, the requirement for one or two COVID jabs will soon be turned into three, and vaccine passport holders who don’t want to get that third shot will be back at Square 1. They’ll be just as undesirable as those who got no shots.
Considering the speed at which SARS-CoV-2 is mutating, you can be assured there will be a fourth shot,and a fifth and, well, you get the idea. Vaccine passports and COVID jab requirements will simply lead to a situation where you have to keep getting additional shots or lose all your privileges.
Of course, every single injection comes with health risks, and the risk for an adverse event will probably get bigger and bigger with each additional shot, and you don’t need to be a modern-day Nostradamus to see where this will lead us.
Five-Month Booster Shot Now Under Consideration
Unfortunately, rather than accepting reality — which is that SARS-CoV-2 is here to stay, just like any number of other common cold and influenza viruses — and stopping the merry-go-round of injections that only make matters worse, President Biden said he’d spoken with Dr. Anthony Fauci about giving booster shots at the five-month mark after the initial round of injections rather than waiting eight months, as previously suggested.33
While Fauci quickly responded34 that eight months was still the goal, he also said that “we are open to data as they come in” if the Food and Drug Administration and the Advisory Committee on Immunization Practices determine a sooner timeline is necessary.
Israel began administering a third booster shot to people over the age of 60 July 30, 2021. August 19, eligibility for a booster was expanded to include people over the age of 40, as well as pregnant women, teachers and health care workers, even if they’re younger than 40. Initial reports suggest the third dose has improved protection in the over-60 group, compared to those who only got two doses of Pfizer.35 According to Reuters:36
“Breaking down statistics from Israel’s Gertner Institute and KI Institute, ministry officials said that among people aged 60 and over, the protection against infection provided from 10 days after a third dose was four times higher than after two doses. A third jab for over 60-year-olds offered five to six times greater protection after 10 days with regard to serious illness and hospitalization.”
Anyone who thinks one or more booster shots are the answer to SARS-CoV-2 is likely fooling themselves though. I look forward with trepidation to data on hospitalization and death rates, not to mention side effect rates, in the months to come.
Knowing what we already know about the risks of these shots and their tendency to encourage mutations, it seems reasonable to suspect that all we’re doing is digging ourselves an ever-deeper, ever-wider hole that’s going to be increasingly difficult to get out of.
Teaching physical therapists when and how to suspect Lyme disease
By Jennifer Shea, PT, ATC-R
I practiced physical therapy for many years prior to becoming ill with Lyme disease and babesiosis. My education included a course in clinical pathology and a unit on infectious disease.
Less than one page in my medical textbooks was devoted to Lyme disease. The text described an acute flu-like illness experienced by individuals following a tick bite.
Key diagnostic features included a bull’s eye rash, facial nerve palsy and a swollen knee. Treatment consisted of a short course of doxycycline. It all seemed pretty straight forward. It wasn’t until I contracted the disease myself that I began to understand its elusive nature.
Unrecognized Lyme disease?
Reflecting back on my career, I recall several patients whom I treated that likely had Lyme disease and/or co-infections. I failed to recognize it at the time.
One patient had been diagnosed with fibromyalgia. As I examined her, she couldn’t tolerate even the lightest touch due to skin sensitivity. She reported profound weakness, fatigue, muscle twitching, and wandering joint pain.
In an effort to improve her strength and endurance, I developed a treatment plan involving gentle aquatic exercise. The water would provide resistance she could tolerate, and the buoyancy could be used to our advantage. She appeared to do well at our first session but chose not to return. She explained that despite the gentleness of the intervention, she experienced overwhelming fatigue and malaise after any type of exercise.
Another patient came to the clinic with a diagnosis of neck pain. Patients can often associate the onset of symptoms with a precipitating event, but this patient’s pain came on gradually and without apparent cause. X-ray and MRI results were normal except for mild age-related changes. The location of her pain shifted randomly, moving from the upper to the lower neck region appearing on the right one day and the left another.
Typically, patients experience symptoms that improve or worsen in a predictable pattern associated with posture, repeated movements, or activities, but this patient’s symptoms fit no such pattern. She experienced numbness and tingling that migrated. During several treatment sessions, she complained of intense headaches and felt generally unwell due to a virus she recently caught that she “just couldn’t shake.” Whenever she appeared to improve in response to treatment, she would regress for reasons unknown.
Horowitz symptom questionnaire
I’ll never know if those patients had Lyme disease. At the time, I didn’t know enough about the disease to consider it as a possible underlying cause for their symptoms.
Today I am alert to its varied manifestations and have the benefit of using a tool called the Horowitz Multiple Systemic Infectious Diseases Syndrome Questionnaire to help sort things out.
The Horotwitz questionnaire has been shown to be a valid, efficient, and low-cost screening tool to assist practitioners in deciding if additional testing is needed to distinguish between Lyme disease and other illnesses. The results of a 2017 study showed that this questionnaire accurately differentiated those with Lyme disease from healthy individuals. It can be used by medical practitioners or laypersons.
According to the CDC, some 476,000 individuals in the United States are diagnosed and treated for Lyme disease annually. According to MyLymeData, most patients see more than four physicians prior to being diagnosed, and 36% do not receive a diagnosis before at least six years of illness.
It’s reasonable to assume that many individuals with Lyme disease who have not yet been diagnosed seek physical therapy services to address the manifestations of the infection. Given that early treatment is associated with better outcomes, raising awareness among health care professionals is imperative.
It’s also important to make people aware of the limitations of diagnostic testing and that they have a choice when seeking treatment. They can choose to be treated under the guidelines set forth by the Infectious Diseases Society of America or those established by the International Lyme and Associated Diseases Society.
Early diagnosis is critical
To that end, I wrote an article that was recently published in Physical Therapy Journal to guide physical therapists in the recognition and referral of individuals with suspected Lyme disease. I hope that by educating physical therapists about the disease, many individuals will be diagnosed sooner than they might be otherwise.
Citera M, Freeman PR, Horowitz RI. Empirical validation of the Horowitz multiple systemic infectious disease syndrome questionnaire for suspected Lyme disease. Int J Gen Med. 2017;10:249-273. doi: 10.2147/IJGM.S140224
_________________
**Comment**
While treatment wasn’t the focus of this article, please understand it would be very unwise to “choose” IDSA Lyme treatment, as you will be given an insufficient course of doxycycline. This abysmal, monotherapy has shown to fail in nearly every antibiotic study ever done for the simple reasons that Lyme is a persistent,stealthy pathogen, and it rarely comes alone.
Far wiser, is to locate a Lyme literate doctor specifically trained in tick-borne illness who appreciates and understands the complexities of treating this monster. These doctors diagnose and treat clinically based upon symptoms, not an antiquated, faulty test that misses anywhere from 50-90% of cases.
If you are new to this game, please read the sordid back-story and why there is polarization within the medical community on nearly every aspect of the illness.
WARNING: Regarding tick-borne illness, all you will get from mainstream medicine is heartache, abuse, and poverty.
Unholy Interlocking of Government, Corporate, and Medical Dogma Sacrifices Lives – The Semmelweis Saga Resurrected
Robert Jay Rowen, MD1*
1Private Medical Practice, 2200 County Center Dr. Ste C, Santa Rosa, California, 95403, USA
Some two centuries ago, Ignaz Semmelweis observed that hand washing with a chlorinated lime solution (an oxidizing agent) would curb infection mortality related to the maternity ward. He was scorned and castigated by his peers for daring to suggest hand washing between dissecting cadavers and delivering babies. Medicine should have learned from this debacle. Has it?
Today we face unprecedented crises in infectious diseases. Pharmaceutical antibiotic drugs that ushered in the medical era are being neutralized by innovative pathogens acquiring resistance or collectively organizing in impossible to treat biofilms. According to the CDC, “more than 2.8 million antibiotic-resistant (“superbug”) infections occur in the U.S. each year, and more than 35,000 people die as a result. In addition, 223,900 cases of Clostridioides difficile occurred in 2017 and at least 12,800 people died” [1].
Despite witnessing the growth of resistance to antibiotics (which are patented for profit), there has been no interest in promoting the defensive innate processes in the human body, which creates innate oxidizing germicides (H2O2, singlet oxygen, ozone, hypochlorite, etc.) to hurl at invaders. In fact, just the opposite occurs, in large part due to the reflex rejection of highly efficacious therapies [2]. Hence, few in the medical field are aware of any alternative to chemical medicine, and fewer will consider “unapproved” therapy, even to save lives [3].
I provide the following first-hand knowledge and will elaborate.
1. In 2018, this practitioner was begged to come and minister ozone therapy to a man (husband, father and airline pilot) dying of a superbug infection in a Texas hospital. Despite the promise of a liability waiver, the hospital denied me access stating: “Policy”. The helpless man died in front of his grieving family. Several years before, a hospitalized beloved Northern California integrative physician died of lethal infection after the institution denied the requests of family and physician friends to administer high dose intravenous ascorbate.
2. One erudite layman, who is a prominent trustee of a major mid-west teaching hospital, asked the infectious disease chairman (ID) if he would permit the use of ultraviolet blood irradiation (UBI) in the hospital to save an otherwise unsalvageable patient. ID responded, “Is it FDA approved?”
Answer, “No”.
ID response, “Then I would not permit it”.
Trustee’s reply, “Then you would let the patient die rather than even tell the patient’s family about UBI?”
ID answer: “Yes”.
The trustee was aghast. “That death could be me!”
3. This practitioner took an associate to, and, led a group in Sierra Leone to use ozone therapy to rapidly cure 100% of 5 cases of the most lethal virus the world has ever known – Ebola (mortality rate – 60%). The report was submitted to major journals which summarily rejected the novel report, one stating: “we don’t think this will be of interest to our general practicing readers.” While ignoring a major potential breakthrough in acute actual viral disease management, the journal was concurrently publishing articles on vaccines for Ebola. A vaccine was of more interest to its European readers than a possible penny costing cure? The ozone breakthrough was later published in the African Journal of Infectious Diseases [4].
4. A south Florida hospital applied for an IND for ozone use in COVID. (2020) The FDA demanded expensive animal studies, despite thousands of publications on ozone and a virtually 100% safety record over many decades. Even “compassionate use” was not considered.
5. Two reporters, one for a small-time news outlet, and the other, a famous reporter for a huge NYC daily, attempted to publish articles on ozone therapy early in the COVID-19 outbreak.Their higher-ups canned publication. Both were shocked.
The world is in deadly “Catch-22” considering non-patentable therapies which might save lives. Therapies that have been studied and reported successful with complete safety for scores of years are called “anecdotal” by the FDA because clinical trials that incur huge unrecoverable costs have not been done. Millions of successful treatments are “anecdotal”. What utter nonsense. These therapies are shunned, even to the tune of watching a patient die.
Condemned to Die with No Right to Try
This seemingly corrupt paradigm has been coined: “Condemned to Die with No Right to Try” [5]. Promising but not “approved” therapies are dead on arrival. Currently, institutional (and individual) “policy” (not law) prevents hospitals (and most conventional physicians) from any consideration of non-FDA approved therapies.
The government/industrial complex has been inserted between the doctor and his patient’s needs/welfare.
This begs the question of the morality of a system that proactively denies a dying patient a chance. What has medicine (and society) become if we chose or permit sacrifice of lives for profit, policy, personal, and corporate interests?
Closer to the practicing physicians lie the state medical boards. Many have attacked doctors’ therapies not “approved” by the FDA. This also leads to death. Medical errors, most often using FDA approved treatments, are the third leading cause of American deaths [6]. FDA approved drugs are the fourth leading cause of American deaths [7]. Approved antibiotics, particularly the newer ones, even when properly administered, can lead to very severe injury.
This journal published the first article on the use of ozone therapy for coronavirus [8]. Since then, several articles have emerged echoing the wisdom of using ozone therapy [9,10], and articles have been published on its success [11–13]. Yet there has been no move by authorities to investigate this reportedly virtually 100% safe treatment, whilst governments expend trillions on novel vaccine research, development and distribution.
CDC reports half a million COVID deaths in the USA alone. Many doctors, including me, reached out to officials with ozone information, only to be shunned. Other oxidation therapies (intravenous hydrogen peroxide [14], ultraviolet blood irradiation (UBI) [15–17], intravenous ascorbate [18]) were reported in the last century to cure or mitigate untreatable serious viral (pneumonia, polio) and bacterial infections, with 100% safety and high efficacy, yet few if any infectious disease experts are so aware. Of course, none of these are patentable for profit (Figure 1).
Figure 1: Knott Hemo-irradiator, circa 1958, original American UBI device, FDA “grandfathered”. View Figure 1
Oxidation therapies harness and augment the body’s own innate pro-oxidant (germicidal) primal defenses against invaders. Ozone is actually produced in the body, and hydrogen peroxide is one of its mediators of action. High dose ascorbate is a pro-drug for hydrogen peroxide. UBI is another oxidant. These therapies have several commonalities. They have been reported: 1) Absolutely safe when properly administered, 2) Highly effective, and, 3) Because they are a “natural cure” in the public domain for many decades, they cannot be patented for profit, remaining unstudied to the degree needed for regulatory agency “approval”. Consequently, they suffer instant rejection. The medical annihilation style of Ignaz Semmelweis remains, morphing from proscribing promising sanitation to proscribing and condemning promising therapies by medical practitioners.
Solutions to the Dilemma
There are solutions to the dilemma. Current hospital practices are based on policy and not law. Change must begin at the lowest level rather than expect an agency (FDA), highly influenced by a revolving door of Pharma interests within the agency, to begin change. Leaving the FDA board should immediately disqualify one from Pharma employment for five years. Having any financial interest in Big Pharma should disqualify one from FDA employment or office.
After all, despite thousands of international articles on ozone therapy, the official stance of the FDA remains:
“Ozone is a toxic gas with no known useful medical application in specific, adjunctive, or preventive therapy. In order for ozone to be effective as a germicide, it must be present in a concentration far greater than that which can be safely tolerated by man and animals” [19].
This statement, while actually a regulation, is blatantly false. Its continuing presence has certainly condemned patients to death. Physicians and hospitals will not look past it. Water is also toxic, as is ozone, if inhaled. It also ignores the myriad of positive published papers and clinical trials readily available for half a century on PubMed.gov, our National Library of medicine, and other databases.
Change can and must begin with physicians caring more about the welfare of their patients than the prevailing dogma/paradigm and interests of the medical and pharmaceutical industry. Hospitals, like government, must recognize the human “unalienable” Right to Life, Liberty and Pursuit of Happiness, which includes health, wellness and recovery, unhindered by “policy”. Clinical success will bring these therapies into the accepted mainstream, regardless of lack of multibillion-dollar studies effectively bypassing regulatory agency obstruction. Considering the crisis we face, mainstream journals should welcome reports on solutions for these times. But to date, prestigious infectious disease journals have failed to publish manuscripts on these therapies.
Courts must also be made to take cognizance of these fundamental human rights. The New Jersey Supreme Court has recently recognized that the informed consent by patients requires doctors to include disclosure of management that the doctor might not even believe in, and let the patient make his/her own choice [20].
If the profession fails to do this on its own (after obtaining an institutional waiver of liability for offering/providing “unapproved” therapy), sooner or later a savvy attorney may bring down the doctor or institution that fails to place the needs of the patient before “policy”. The institutionalized practice of “condemning to die with no right to try” will then come to a “violent” end. Can medicine rise to avoid this? Can medicine (and science) ever put an end to Semmelweis like sagas?


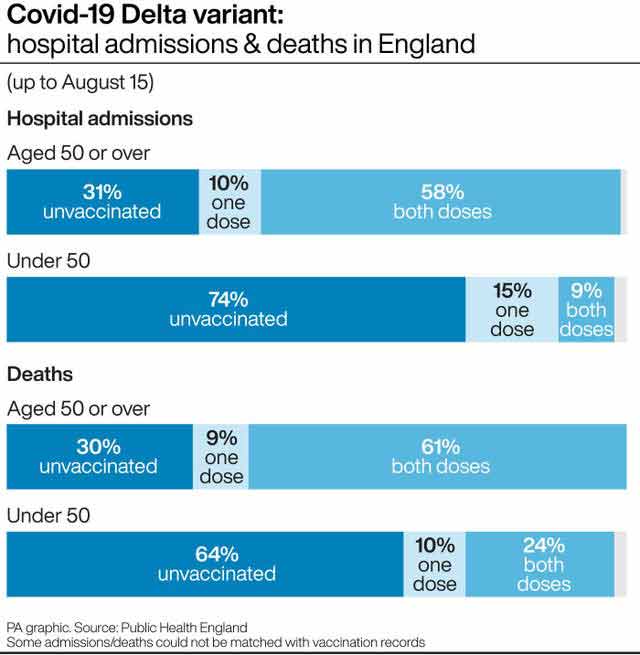

 Figure 1: Knott Hemo-irradiator, circa 1958, original American UBI device, FDA “grandfathered”.
Figure 1: Knott Hemo-irradiator, circa 1958, original American UBI device, FDA “grandfathered”. 