The first 10 minutes is a powerful video about an actual patient who was granted the right to try ivermectin, which ended up saving his life.I’ve posted this before, but it’s worth repeating. The remaining time is a compelling webinar to end 2022 with Betsy Ashton, Dr. Pierre Kory, and special guests filmmaker Connor Callanan, that documented his dad’s hospital treatment and attorney Ralph Lorigo.
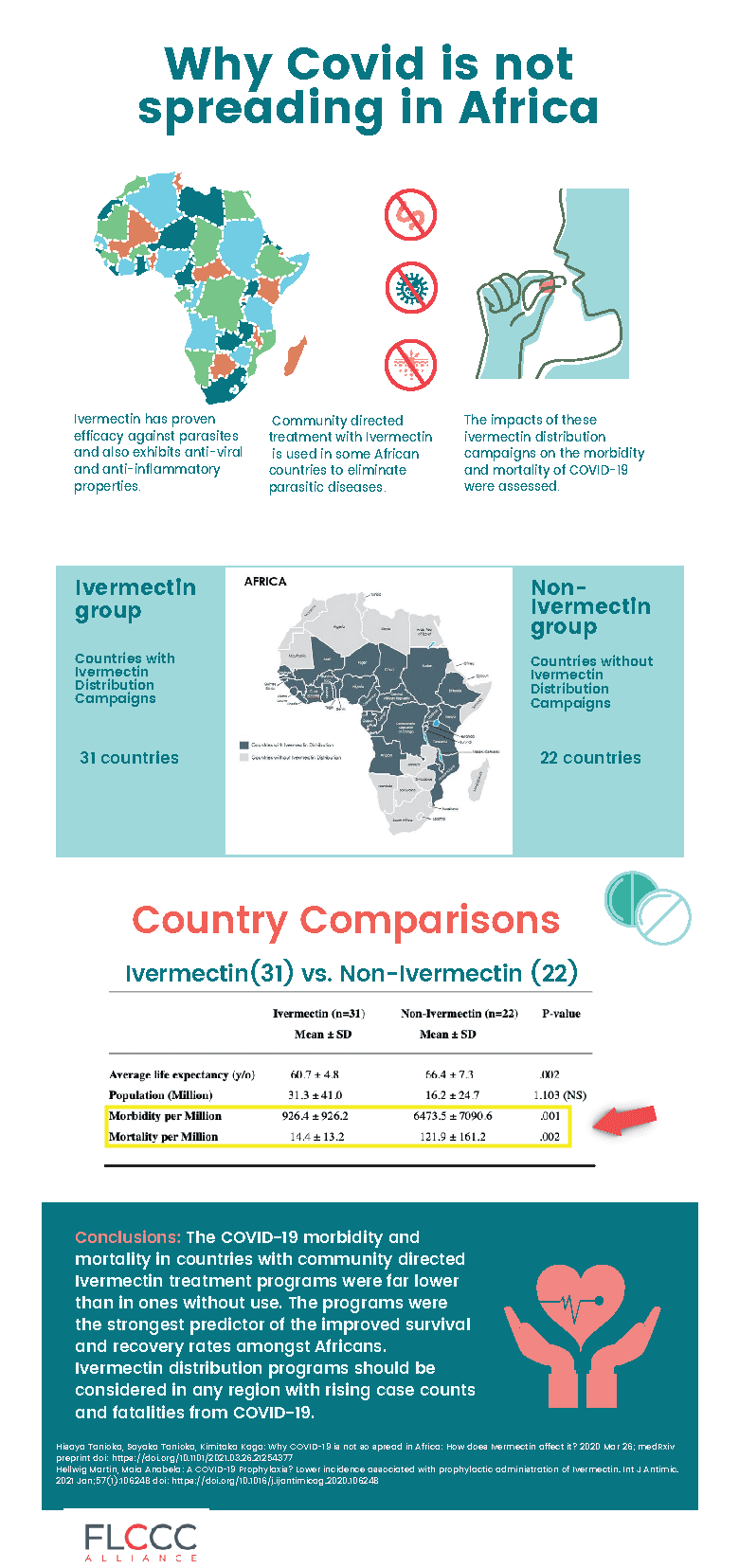
Meanwhile, in the real world, there is no apparent COVID in Africa which just happens to have a community directed ivermectin treatment program which is the strongest predictor of improved survival and recovery rates of COVID. Yet, China, with it’s three year lockdown and tyrannical ZERO COVID policy which is an utter flop, is experiencing a COVID resurgence with even CCP leaders becoming ill and dying.
The CARES Act provides incentives for hospitals to use treatments dictated solely by the federal government under the auspices of the NIH.These “bounties” must paid back if not “earned” by making the COVID-19 diagnosis and following the COVID-19 protocol.
The hospital payments include:
A “free” required PCR test in the Emergency Room or upon admission for every patient, with government-paid fee to hospital.
Added bonus payment for each positive COVID-19 diagnosis.
Another bonus for a COVID-19 admission to the hospital.
A 20 percent “boost” bonus payment from Medicare on the entire hospital bill for use of remdesivirinstead of medicines such as Ivermectin.
Another and larger bonus payment to the hospital if a COVID-19 patient is mechanically ventilated.
More money to the hospital if cause of death is listed as COVID-19, even if patient did not die directly of COVID-19.
A COVID-19 diagnosis also provides extra payments to coroners.
CMS implemented “value-based” payment programs that track data such as how many workers at a healthcare facility receive a COVID-19 vaccine.Now we see why many hospitals implemented COVID-19 vaccine mandates. They are paid more.
Outside hospitals, physician MIPS quality metrics link doctors’ income to performance-based pay for treating patients with COVID-19 EUA drugs.Failure to report information to CMS can cost the physician 4% of reimbursement.
Dr. Campbell states he is getting reports that there is virtually ZERO COVID in Uganda. Surveys were given to community health partners including doctors, nurses, and medical officers around the country. He states:
“No one is getting ‘vaccinated.’ They don’t see any COVID. They’re not getting tested. Clinically they are not seeing it in the hospitals. They are not seeing people come in with respiratory distress and other complications of COVID. The government aren’t even publishing guidelines anymore.”
Last year I posted how mainstream media simply can’t fathom why Africa remains relatively unscathed from COVID despite the fact they have community directed ivermectin treatment programs to fight river blindness. Ivermectin, of course, has been discredited and banned by corrupt public health ‘authorities’ despite mounting evidence they simply ignore. In fact, ivermectin programs were the strongest predictor of improved survival and recovery rates of COVID in Africa, but nobody in power cares.
Meanwhile, China’s 3 year lockdown, mandated masking, and ZERO COVID policy is a complete and utter flop with CCP leaders now sick and dying from COVID. Their answer? Allowing the public to purchase the Pfizer COVID drug Paxlovid which is:
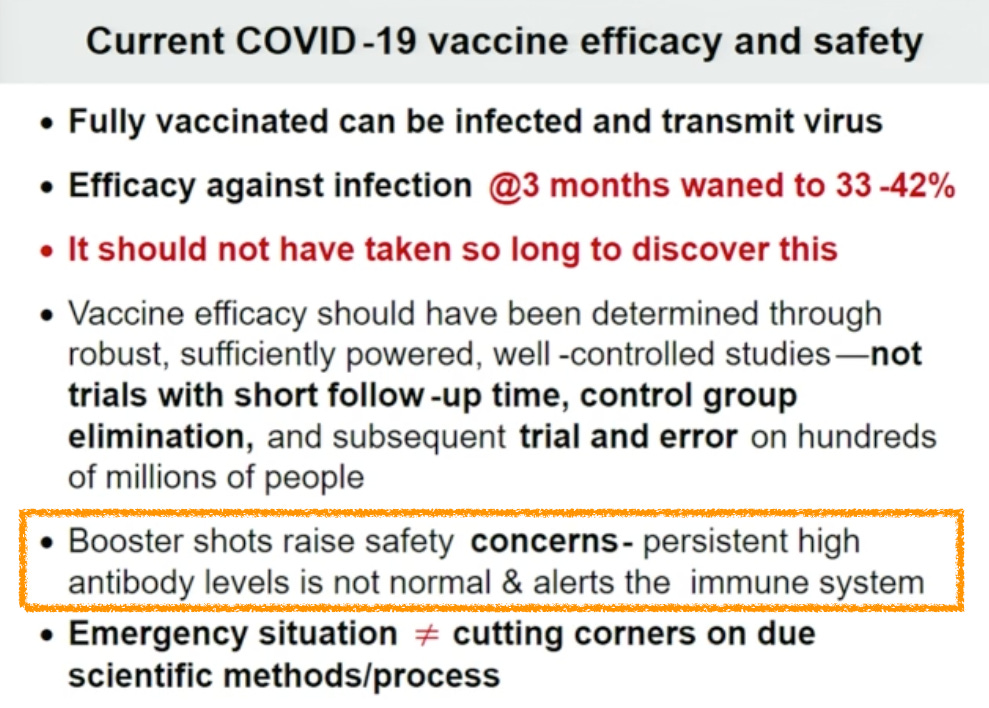
IgG4 surges, and lab-apparent T Cell targeting of infected cells declines following a 3rd Dose of the Pfizer/BioNTech Covid vaccine, in a new study from Bavaria.
Spike-overload finally seems to be showing a concrete effect in the repeat-injected: B Cells in two separate cohorts were found to be self-switching to IgG4 class antibodies, associated with tolerance and anti-inflammatory response, after the 3rd dose.
Commenter Jim H did me the splendid favor of directing my attention to a new pre-print about IgG4. It’s a game-changer.1
So, let’s review this incredible and totally unforeseeable2 discovery. (See link for article)
The Entire Warning Re: Pathogenic Priming Has Been Missed By Allopathic Medicine and by Many Who Discuss the Perils of COVID-19 “Vaccines”
The lesson from pathogenic priming is simple: more exposures means more immune disasters. In thrombocytopenia and other forms of immunopenia, for example, the scientific literature cites the IPAK April 2020 finding that 1/3 of the proteins to which SARS-CoV-2 shows risk of autoimmunity via pathogenic priming involve the immune system.
My predictions from April 2020 have sadly been born out by the scientific literature.
In 2020 alone, 14 studies cite the original Pathogenic Priming results, I’m sad to say, with evidence of myriad autoreactogenicity (see them here).
Far from beating my chest, I am deeply saddened that the way to avoid pathogenic priming induced morbidity and mortality is avoid repeated exposures to SARS-CoV-2 proteins. Obviously, with eternal boosters, the cycle of
vaccine → infect → vaccinate → infect —>…
will be eternal for those stuck in that loop, with I would expect 4-6 infections per year for some – their immune systems being confused, Th2-skewed, class-shifted, ground to dust. Source
Weiler is offering a course called “Exploring Mechanisms of Vaccine Injury/Potential Recovery Protocols – Iatrogenic Illness in Partnership with VITA” that is now being considered for CMEs for physicians. He asks all of us to send this information to medical practitioners as there’s no time to sound more warning bells. He states:
Other than this, all I can do at this point is share my remorse and sadness that more people were not warned in time.
Background/Aim: Chlamydia pneumoniae (C. pneumoniae) is implicated in the pathogenesis of Alzheimer’s disease (AD). Chlamydial elementary and reticulate bodies have been identified in tissues from afflicted AD brain regions by electron and immunoelectron microscopy, whereas similar tests of non-AD brains were negative for the bacterium. Studies in mice have shown that C. pneumoniae can rapidly penetrate the central nervous system by entering glia and causing beta amyloid deposition via the nerves between the nasal cavity and the brain, which serve as invasion pathways.
Materials and Methods: We used data from the UK Biobank (UKBB) to assess the relationship of chlamydia and AD. Circulating C. pneumoniae antigen measurements were not available, but UKBB data field 23037 held measurements of PorB antigen for Chlamydia trachomatis (C. trachomatis). We used C. trachomatis as a surrogate for C. pneumoniae since serum cross-reactivity to C. trachomatis and C. pneumoniae antigens occurs in patients with documented infection and in healthy children as revealed by microimmunofluorescence and immunoblotting techniques. Single nucleotide polymorphism (SNP) data for rs429358 and rs7412 were used to impute ApoE genotypes.
Results:PorB antigen levels for C. trachomatis were significantly higher in subjects with AD (p=0.007). PorB antigen levels were not related to ApoE genotype (e3e3, e3e4, e4e4) p=0.783. To control for the effects of age, sex, educational level, and apoE genotype, logistic regression analysis was performed. AD was the dependent variable. Independent variables were sqrt PorB antigen for C. trachomatis, age, sex, educational level, apoE genotype. AD odds ratio (OR) increased 1.156 for each unit increase of sqrt PorB antigen for C. trachomatis and the effect was significant (p=0.004).
Conclusion: PorB antigens for C. trachomatis being significantly higher in subjects with AD, corroborates previous studies demonstrating that C. pneumoniae inflammation appears to play a role in AD development. AD may result from the reactivation of embryologic processes and pathways silenced at birth. A trigger for the reactivation may be bacterial or viral infections. Further studies are warranted.
Chlamydia pneumoniae is a respiratory tract pathogen but can also infect the central nervous system (CNS). Recently, the link between C. pneumoniae CNS infection and late-onset dementia has become increasingly evident. In mice, CNS infection has been shown to occur weeks to months after intranasal inoculation. By isolating live C. pneumoniae from tissues and using immunohistochemistry, we show that C. pneumoniae can infect the olfactory and trigeminal nerves, olfactory bulb and brain within 72 h in mice. C. pneumoniae infection also resulted in dysregulation of key pathways involved in Alzheimer’s disease pathogenesis at 7 and 28 days after inoculation. Interestingly, amyloid beta accumulations were also detected adjacent to the C. pneumoniae inclusions in the olfactory system. Furthermore, injury to the nasal epithelium resulted in increased peripheral nerve and olfactory bulb infection, but did not alter general CNS infection. In vitro, C. pneumoniae was able to infect peripheral nerve and CNS glia.
In summary, the nerves extending between the nasal cavity and the brain constitute invasion paths by which C. pneumoniae can rapidly invade the CNS likely by surviving in glia and leading to Aβ deposition.
Co-infecting agents can be transmitted together with Borrelia burgdorferi by tick bite resulting in multiple infections but a fraction of co-infections occur independently of tick bite. Clinically relevant co-infections are caused by Bartonella species, Yersinia enterocolitica, Chlamydophila pneumoniae, Chlamydia trachomatis, and Mycoplasma pneumoniae…..Chlamydia trachomatis primarily causes polyarthritis. Chlamydophila pneumoniae not only causes arthritis but also affects the nervous system and the heart, which renders the differential diagnosis difficult.
Ever wonder why masks were mandated? In this clip, retired pharma R&D Exec Sasha Latpova explains that masking induces acidosis within 30 minutes because you are re-inhaling your own CO2. This acidosis triggers positives for PCR as well as illness.
A study published in 4/24 shows that while face masks can filter larger particles and fibers under specific indications, they also carry risks. A review of 24 studies showed:
(63%) had high micro- and nanoplastics (MPs and NPs) release
Go here for a review of every possible study, expert opinion and commentary on masks ever done since the 1920 Kellogg Mask Study which will never be on any of the government or health agency websites.
A brief summary on what they found:
not one study has a control group of healthy people for comparison (this shenanigan is done with ‘vaccine’ studies as well)
there are no peer reviewed studies for healthy people wearing masks
terms like “statistically significant” or “clinically relevant” are no where to be found in any of their literature. “May” or “could” are not good enough
they cite 0 studies which have masks as the only form of source control(usually mixed with hand washing, sanitizer or distancing)
many of the references have no relevance to the actual study
a majority of the above studies are based on anecdotal observations
any study done during the summer as proof is ridiculous as upper respiratory viruses don’t like temps over 80°F
models or mannequins DO NOT provide a adequate substitute for humans
A meta-analysis on 78 studies by Cochrane determined masks probably make little to no difference in the outcome of influenza-like illnesses like COVID. The analysis also reported: “Harms were rarely measured and poorly reported.”
White House Covid Advisor, Dr. Jha, finally admits on a recent zoom call that there’s:
“No study in the world that shows that masks work that well.”
Yet, despite a meta analysis and the admission by the White House COVID adviser, the CDC is the ONLY national or international public health agency that recommends masking two year old children.Listen to CDC Director Rochelle Walensky ramble on and on with pure & utter nonsense. In this important video, Dr. Prasad reads a statement from CDC director Rochelle Walensky and then states the following:
“She’s just making things up. She’s good at making things up. She made up the fact that there’s credible data that we should mask kids between 2 and 5 even though UNICEF and the WHO said not to do that. She made that up. She makes up lots of things, because she doesn’t actually use science to guide decision making, she just likes to make things up.” ~ Dr. Vinay Prasad
Masks Again?! Here’s What Current Science Says About Mask Efficacy.
Dr. Champion PhD discusses the recent push to reinstitute mask mandates and shares with you the current state of science on the effectiveness, or lack thereof, concerning masks. Be prepared with the facts! Dave also shares how sharing the science behind the question of mask efficacy was a significant element leading to YouTube shutting down his channel.
Read this hilarious account of how alpacas did their own searching and cataloging of all the mask studies.
Highlights:
the alpacas looked for randomized controlled trials – you know, the way we normally evaluate medical interventions
the alpacas found 18 (RCTs) on masks between 2008 and 2019, which is 18 more than Todd the CDC Intern managed to find when he compiled the CDC web page about masks
the article provides a quick summary of each one – with references and links at the end
Conclusion: Since the CDC clearly can’t read, the alpacas ask if someone could please transmit this information verbally to them. For the 18 studies, we have:
9 with no statistically significant benefit of masks
4 with no unmasked control
0 with a positive result vs. unmasked control
2 with a negative result vs. unmasked control
3 with “may help” vs. unmasked control (but not a statistically significant result)
Of the 14 studies with a “no mask” control, 9 showed no benefit, 3 showed weak evidence of benefit, and 2 showed strong evidence of harm.
The evidence that masks can be harmful is at least as strong as the evidence they may help.
None of this justifies forcing anyone to do anything.
Article excerpts:
And now the dirty little secret no one talks about
A lot of studies look for lab confirmed influenza because it’s a common virus and people get infected with it every flu season. Some of the studies also use one or more clinical definitions of influenza, meaning they have doctors diagnose people for illness (defined as fever plus symptoms).
Here is the point of this whole post
In several studies, the rate of diagnosed illness is higher in the mask group even though the lab confirmed influenza isn’t. These people aren’t faking it – they really have fevers and sore throats, it’s just not from influenza virus. And it’s often a statistically significant result.
But these studies are testing for lab confirmed influenza virus, so they don’t test for other things. The masks made these people sick but we don’t know why. Was it from other viruses? Bacteria? Fungi? Was it from breathing the chemicals in the masks? We don’t know, but we should be concerned.
Based on these studies, we have good reason to think that wearing masks all day will make more people sick.
And that’s the dirty little mask secret no one talks about.
________________
Please also see this short video put out by America’s Frontline Doctors (AFLD) on the ineffectiveness of masks.
Similarly to the useless (negative efficacy) and dangerous COVID gene therapy shot, which don’t stop transmission, infection, severe illness, or even death, zealots simply don’t care.
The CDC refuses to fix it’s horriblyflawed mask study which is being still being used to set public health policy, and the CDC and the FDA are completely guilty of mis or disinformation, yet are still coming after others who disagree with their fraudulent narrative.
The current administration has been found guilty of colluding with social media companies to suppress freedom of speech under the guise of ‘misinformation,’ and nearly got away with a DHS ‘ministry of truth’ type disinformation board run by ‘Scary Poppins’ until the public gave fierce backlash. And now the UN is declaring war on “conspiracy theories” and launches a #thinkbeforesharing campaign. UNESCO has teamed up with Twitter, the European Commission and the World Jewish Congress to launch the campaign.