Excess Deaths in UK Higher Now Than During COVID ‘Pandemic’ & Unvaxxed Have Lower Mortality Rate Than Vaxxed
**UPDATE**
Please watch this brief 3 minute video on Denmark’s alarming excess mortality for every age cohort, and the fact they have stopped the COVID shots for those under age 50. The U.S. is experiencing the same thing. Why are they not stopping these clot shots here?
http:// Approx. 8 Min
Excess Deaths Higher Now Than During COVID ‘Pandemic’
GBNews
Nov. 9, 2022
Jamie Jenkins former leader of Health Numbers at the Office For National Statistics in the UK. goes through the alarming excess deaths being seen which the mainstream media simply ignores.
________________
Striking Correlation Between Autumn Vaccine Boosters and Excess Deaths in England as Total Non-Covid Excess Tops 23,000
Why is The UK Suffering an Unaddressed 9/11-Like Excess Death Rate Every Two Weeks?
The numbers of deaths of various types, never attributed to the vaccine, or even to post-infection problems, tells us that something is horrifically wrong.
About 1/2 of the deaths are attributed to “COVID-19”, but given policy flaws and false positives, and reports of re-coding deaths, we can expect that the true attributable fraction is far less.
In mid-September, 2022, the non-COVID-19 attributed excess was called “puzzling” by The Guardian; mass causality disasters caused by vaccination are not “puzzling” when we know the mechanisms of harm caused by the adenovirus vaccines, and the mRNA vaccines themselves. Plus, we know about Pathogenic Priming. Further, how many of the COVID-19 deaths are due to ADE is not estimated.
We now have two years’ worth of data from in the post-vaccine era (PVE, data are from Statistica). The data hint at a seasonality pattern in excess deaths opposite to that of the typical winter respiratory disease deaths, which would imply a lag, but it’s too soon to tell.
Excerpts:
The report goes on to educate us that COVID-19 ranks 12th in the cause of death, with the #1 cause of death being Alzheimer’s (attributable of course to aluminum exposure).
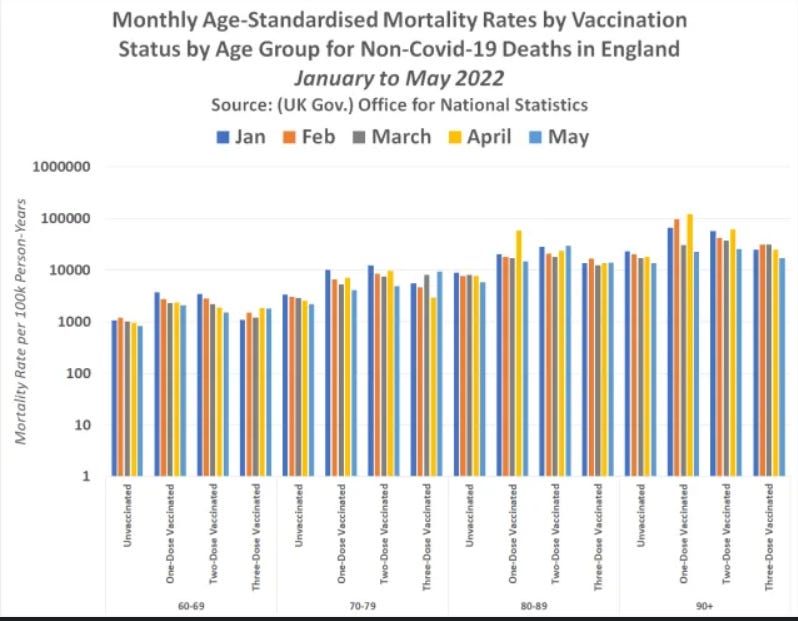
Here are some older ONS data (to May, 2022) showing the unvaccinated have the lowest per capita mortality rate in the UK compared to the other variously-vaccinated:
Regarding Pathogenic Priming and ADE a new study confirms that reinfection with COVD increases risks of death, hospitalization, and sequelae in multiple organ systems.
COVID jabs cause pathogenic priming through ADE but mainstream medicine and media will never discuss this. We also know the chosen treatment of Paxlovid causes COVID rebound – or reinfection, and is extremely dangerous. This is similar to the fact that COVID and the shots – due to blood clotting, as well as masks cause hypoxia (low oxygen). COVID spreads through floors and walls, yet people are still masking up with oxygen depriving, bacteria laden masks which obviously don’t stop a virus or reduce transmission. This will also never be revealed by mainstream medicine or media.
Government publishes horrific figures on COVID Vaccine Deaths: 1 in every 310 people died within 1.5 months of receiving the COVID Vaccine Booster
Excerpts:
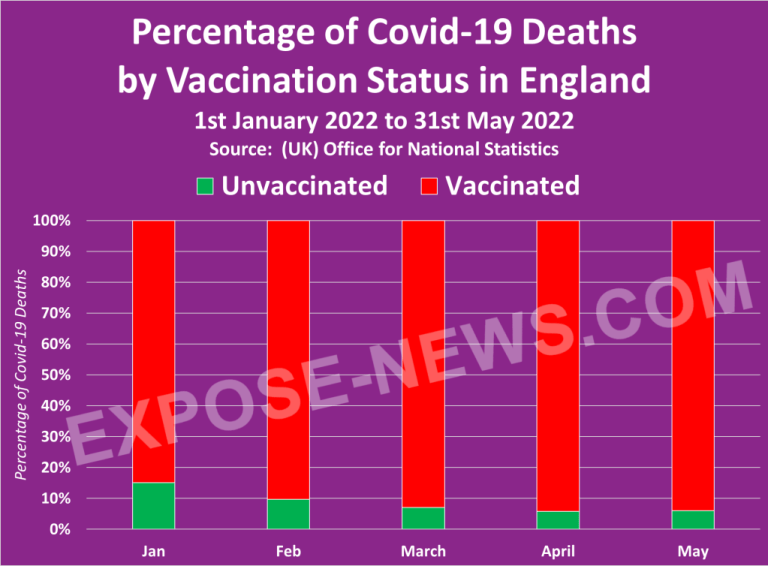
The dataset does not reveal how these figures compare to the unvaccinated, but another dataset published by the ONS on July 6th 2022, does.
The dataset, which can be downloaded here and accessed on the ONS website here, shows that between 1st January 2022 and 31st May 2022, the vaccinated population accounted for 9 in every 10 Covid-19 deaths, and 91% of those deaths were among the triple/quadruple vaccinated.
Sudden Canadian Doctor Deaths now at 90
Ninety Canadian doctors have died suddenly or unexpectedly since the rollout out of the dangerous and ineffective Covid-19 mRNA “vaccines,” according to the research of Dr. William Makis, MD, without ANY investigation by the Canadian Medical Association (CMA). The agency has ignored two letters of concern with research findings from Dr. William Makis and has turned around and stated that this doctor’s research is dangerous “disinformation.”
Medical associations are completely controlled by unelected officials in bed with Big Pharma who are using censorship and persecution tactics against any doctors who dissent. They also teach doctors to deceive patients. These organizations need to be disbanded and rendered defunct.
_________________
http:// Approx. 2 Min
Nov. 10, 2022
GBN News: Mark Dolan Tonight
Remember Those Who wanted To Punish the Unvaxxed & Called Them ‘Racist’
“They’ve got blood on their hands. Never forgive. Never forget. And Never Again.” ~ Mark Dolan
For more:
- https://madisonarealymesupportgroup.com/2022/11/02/huge-excess-deaths-why-is-no-one-investigating-this-data-show-moderna-doubles-chance-of-infant-death-compared-to-pfizer/
- https://madisonarealymesupportgroup.com/2022/08/09/cdc-caught-lying-yet-again-about-association-between-heart-inflammation-mrna-shots-professor-shows-a-relationship-between-excess-deaths-shots/
- https://madisonarealymesupportgroup.com/2021/09/17/new-physician-alliance-hospitals-killing-people-doctors-hamstrung-by-regulators-leading-to-hundreds-of-thousands-of-excess-unnecessary-deaths/
- https://madisonarealymesupportgroup.com/2022/06/01/vaers-hijacked-open-letter-from-nzdsos-need-to-investigate-deaths-following-vaccination/
- https://madisonarealymesupportgroup.com/2020/12/21/warning-3150-injuries-in-1st-week-of-covid-vaccines-among-american-healthcare-workers-pregnant-women-included/ Latest VAERS data and mounting list of adverse reactions & deaths