https://physiciansforinformedconsent.org/covid-19-vaccines/

Physicians for Informed Consent: CDC Data Show COVID-19 Mass Vaccination Has Had No Measurable Impact on COVID-19 Mortality in the U.S.
Newly released document highlights 20 scientific facts that challenge the assumptions underlying COVID-19 vaccine mandates.
NEWPORT BEACH, CALIF. (PRWeb) – February 22, 2022
Physicians for Informed Consent (PIC), an educational nonprofit organization focused on science and statistics, has released a new educational document entitled, “COVID-19 Vaccine Mandates: 20 Scientific Facts That Challenge the Assumptions.” The document helps readers become more familiarized with the scientific facts regarding COVID-19, its treatment options, and the COVID-19 vaccines.
Developed in a reader-friendly format, the document highlights available scientific data from the Centers for Disease Control and Prevention (CDC), U.S. Food and Drug Administration (FDA), and COVID-19 vaccine clinical trials, and it addresses the assumptions underlying COVID-19 vaccine mandates. Twenty scientific facts are provided on key public health topics, including:
- The lack of a long-term benefit of the COVID-19 vaccines on the spread of COVID-19
- The lack of a proven benefit of the COVID-19 vaccines on COVID-19 deaths
- The risks of COVID-19 vaccine injections versus the safety of SARS-CoV-2 infection in children
- Waning vaccine immunity and booster shot efficacy
- COVID-19 early-treatment and prevention options
“Vaccine mandates are unethical because they attempt to coerce people to act against their own judgment, and because they are unscientific,” said Dr. Shira Miller, founder and president of PIC. “Our focus is on delivering scientific data about infectious diseases and vaccines which are often overlooked in the mainstream. We developed this new document to help physicians, policymakers and the public better understand and communicate about the scientific facts that challenge the assumptions underlying COVID-19 vaccine mandates.”
The document reveals CDC data — from April 2020 through January 2022 — which show that mass vaccination with the COVID-19 vaccine has had no measurable impact on COVID-19 mortality in the U.S. In addition, short-term clinical trial data indicate that 1 in 6 to 1 in 9 people 12–55 years of age who receive mRNA COVID-19 vaccines suffer severe (grade 3) systemic reactions, and long-term safety studies have not been conducted. And finally, more than 53% of Americans have already had COVID-19 and may have greater protection against reinfection than vaccinated people.
To download your copy of “COVID-19 Vaccine Mandates: 20 Scientific Facts That Challenge the Assumptions,” visit physiciansforinformedconsent.org/covid-19-vaccines. Readers are encouraged to share the document with their physicians, family and community.
About Physicians for Informed Consent
Physicians for Informed Consent is a 501(c)(3) educational nonprofit organization focused on science and statistics. PIC delivers data on infectious diseases and vaccines, and unites doctors, scientists, healthcare professionals, attorneys, and families who support voluntary vaccination. In addition, the PIC Coalition for Informed Consent consists of over 300 U.S. and international organizations that represent millions of people. To learn more or to become a member, please visit physiciansforinformedconsent.org. |
|
COVID-19 Vaccine Mandates: 20 Scientific Facts That Challenge the Assumptions
Fact 1: “all transmissions between patients and staff occurred between masked and vaccinated individuals, as experienced in an outbreak from Finland.” The authors state that the study “challenges the assumption that high universal vaccination rates will lead to herd immunity and prevent COVID-19 outbreaks.”1
Fact 2: CDC study found that 74% of cases were fully vaccinated.2
Fact 3: Harvard study found “no significant signaling of COVID-19 cases decreasing with higher percentages of population fully vaccinated.”3
Fact 4: There is no evidence from clinical trials that any of the vaccines prevent death because they did not have enough statistical power to measure the vaccine’s ability to prevent deaths.4-6 The FDA states, “A larger number of individuals at high risk of COVID-19 and higher attack rates would be needed to confirm efficacy of the vaccine against mortality.”4-6
Fact 5: CDC study observed that 100% of severe, critical, and fatal cases of COVID-19 occurred in vaccinated individuals.1
Fact 6: CDC data show mass vaccination with the COVID-19 vaccine has had no measurable impact on COVID-19 mortality in the U.S.7
Fact 7: In the Pfizer clinical trial, there were zero cases of severe COVID-19 in children who did notreceive the vaccine. 8,9 In contrast, for children 5 years or older, the Pfizer COVID-19 vaccine clinical trial found that the vaccine causes severe (grade 3) systemic reactions that include fever greater than 102.1° F; vomiting that requires IV hydration; diarrhea of six or more loose stools in 24 hours; and severe fatigue, severe headache, severe muscle pain, or severe joint pain that prevents daily activity.9-12
Fact 8: In the clinical trial, a range of 1 in 59 to 1 in 143 vaccinated children 5 to 11 years of age suffered severe systemic reactions within seven days of the second dose. There were 3 to 8 cases of severe systemic reactions observed in the vaccinated group for every 10 cases of non-severe COVID-19 in the unvaccinated group.9
Fact 9: In the clinical trial, 1 in 9 vaccinated adolescents 12 to 15 years of age suffered severe systemic reactions within seven days of receiving the second dose. There were 7 times more severe systemic reactions observed in the vaccinated group than non-severe COVID-19 cases in the unvaccinated group.10-12
Fact 10: The clinical trial also found that 1 in about 1,100 vaccinated children 12 to 15 years of age had a grade 4 systemic reaction (fever greater than 104° F) after the first dose that required an ER visit and withdrawal from the study.10,13
Fact 11: The Pfizer clinical trial did not have enough statistical power to show the vaccine is safe in children under 18 years of age, as the study did not include enough subjects to establish safety (i.e., the clinical trial only included about 2,600 vaccinated children aged 5 to 15).9,14 In comparison, it is known that COVID-19 fatalities are rare in children. As of Nov. 3, 2021, the chance of a child 17 years or younger contracting SARS-CoV-2 and dying from COVID-19 was 1 in 126,000 or 0.0008%.15
Fact 12: Because all subjects in clinical trials were observed for only two to six months, the long- term safety of COVID-19 vaccines for any age group is not known. Per the FDA, there are currently insufficient data to make conclusions about the safety of Pfizer, Moderna and Johnson & Johnson vaccines in subpopulations such as pregnant and lactating individuals, and immunocompromised individuals.4,8,16 Per Pfizer, the vaccine “has not been evaluated for the potential to cause carcinogenicity, genotoxicity, or impairment of male fertility.”17
Fact 13: Safety surveillance reports have identified serious risks of myocarditis and pericarditis in subjects under age 40, within seven days of vaccination. In boys aged 16 or 17, the FDA has reported an excess risk of myocarditis or pericarditis of 1 in 5,000 after the second dose of the Pfizer COVID-19 vaccine.18 And in boys aged 12 to 17, also after a second dose of the Pfizer COVID-19 vaccine, a Hong Kong study found an excess risk of myocarditis or pericarditis of 1 in 2,700.19
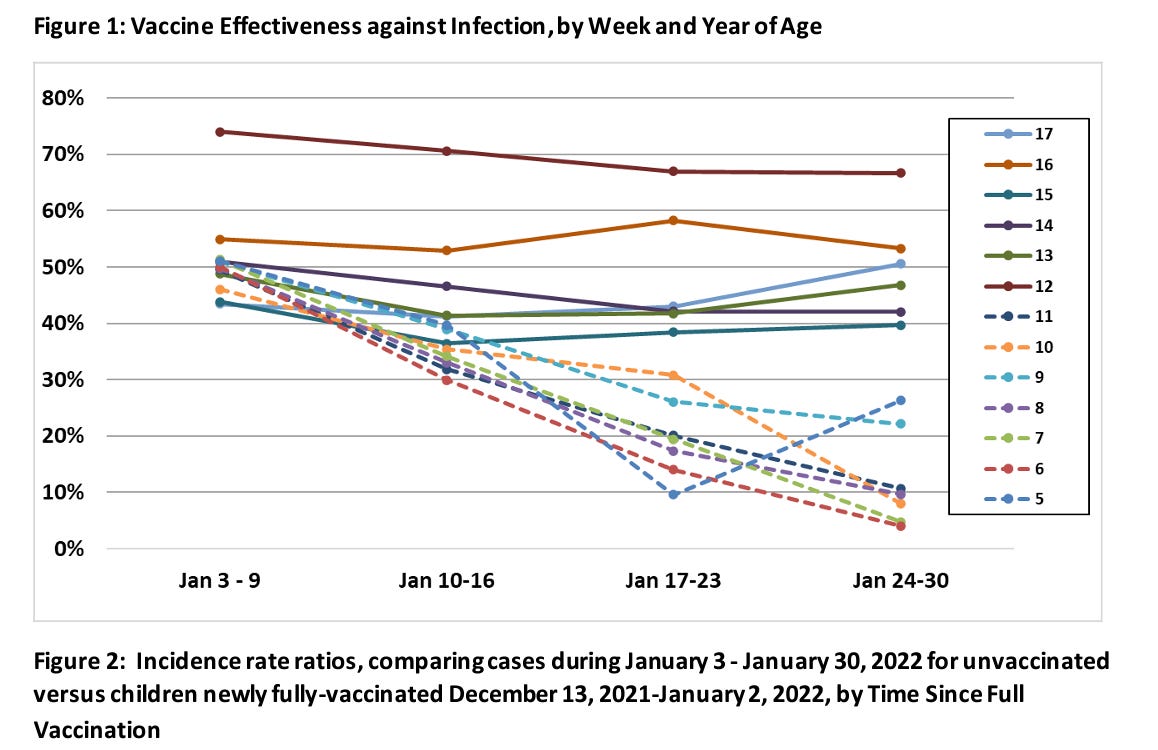
Fact 14: The clinical trials detected that vaccine immunity wanes significantly over a short period of time. For example, the Pfizer vaccine efficacy decreased by 8% to 18% within only six months, and the J&J vaccine efficacy decreased by 25% to 29% within only six months.20,21 Additionally, the efficacy measured in the clinical trials was against the original Wuhan strain, not the new variants.
Fact 15: In clinical trials, a third dose of Pfizer or Moderna vaccine or a second dose of Johnson & Johnson vaccine has not been evaluated for efficacy against disease, but rather antibody counts were observed in a small number of vaccinated subjects for only one month.18,21,22
Fact 16: Treatments for COVID-19 have improved significantly since the pandemic began in early 2020, resulting in improved survival rates in hospitalized cases.23,24 Indeed, for people not living in a nursing home, the overall survival rate of COVID-19 is 99.8% in the U.S., and 99.999% for children specifically.25,26
Fact 17: Hundreds of studies have observed the effectiveness of various treatments, the most studied being ivermectin, vitamin D, hydroxychloroquine (HCQ), and monoclonal antibodies.27-30 These treatments may also be beneficial for prophylaxis (i.e., pre-exposure or post-exposure prevention of symptomatic COVID-19 infections).31-35
Fact 18: There is evidence that previous SARS-CoV-2 infection is more effective at preventing SARS- CoV-2 infection than COVID-19 vaccines. The J& Jvaccine clinical trial included over 2,000 subjects who had contracted SARS-CoV-2 before the study. The trial, which tested unvaccinated and vaccinated people uniformly, recorded the incidence of COVID-19 in that unvaccinated group at least 28 days after the vaccination of the other subjects in the study. The COVID-19 incidence of the unvaccinated group with prior SARS-CoV-2 infection was 0.1% (2/2,021), whereas the COVID-19 incidence of vaccinated subjects was 0.59% (113/19,306). These data suggest that there are 6 times more cases of COVID-19 in vaccinated subjects than in unvaccinated subjects previously infected with SARS-CoV-2.36
Fact 19: Data from the Johnson & Johnson clinical trial also indicate that an unvaccinated person previously infected with SARS-CoV-2 has a 99.9% chance of being protected from a repeat infection. Of note, as of July 1, 2021, there have been 177.4 million SARS-CoV-2 infections in the U.S., which is 53.8% of the U.S. population.26,36
Fact 20: Infection and transmission of SARS-CoV-2 occur at high rates in fully vaccinated populations, and a significant proportion of severe, critical and fatal COVID-19 cases occur in fully vaccinated individuals. CDC data show mass vaccination with the COVID-19 vaccine has had no measurable impact on COVID-19 mortality in the U.S. In addition, short-term clinical trial data indicate that 1 in 6 to 1 in 9 people 12–55 years of age who receive mRNA COVID-19 vaccines suffer severe (grade 3) systemic reactions, and long-term safety studies have not been conducted.13,37 Thus, the scientific data demonstrate that vaccine mandates have not been proven to create a safer environment.
Source