Episode 355: Tick Report – an interview with Professor Stephen Rich
May, 2023
In this episode of the Tick Boot Camp Podcast, we welcome Professor Stephen Rich, a well-respected scientist in the chronic Lyme disease community from the University of Massachusetts Amherst. Join us as Professor Rich shares insights into his research on tick-borne diseases and practical applications, focusing on Lyme disease transmission, deer’s role in the spread of Lyme, and various preventive measures.
Professor Rich’s background and the Laboratory of Medical Zoology at UMass Amherst
Practical applications of Lyme research and training other scientists
Understanding the tick feeding process and Lyme disease transmission
The debate on Lyme disease transmission through other vectors (mosquitoes, bed bugs)
Spatial protection tools for preventing tick bites
Attachment times for Lyme and other tick-borne illnesses
The mystery behind the Lone Star tick-borne illness Alpga-Gal Syndrome (AGS)
The role of mice in Lyme disease transmission
Strains of Borrelia burgdorferi and their impact on humans
CDC’s stance on tick testing and available testing options through Tick Report
The importance of tick checks and using multiple senses
In this informative episode, Professor Stephen Rich offers valuable knowledge about the transmission and prevention of Lyme disease and other tick-borne illnesses. By understanding these complex processes, we can develop better preventive measures and treatment strategies. Stay tuned for future episodes featuring more insights from experts in the field.
CASE REPORT: LYME DISEASE CAUSES INFLAMMATION OF THE SPINAL CORD
There have only been 8 documented pediatric cases of Lyme disease causing transverse myelitis. In this report, the authors describe the ninth case involving a 10-year-old boy.
Transverse myelitis (TM) is an inflammation of both sides of one section of the spinal cord. Diagnosis requires clinical symptoms and evidence of inflammation within the spinal cord via cerebrospinal fluid analysis and/or magnetic resonance imaging.
Treatment of transverse myelitis typically includes oral steroids, intravenous immunoglobulins, plasma exchange, and immunomodulatory therapies.
“Clinical features consist of sensory disturbances in most patients, followed by weakness and sphincter dysfunction. Children suffer from more severe clinical impairment than adults,” the authors wrote.
In fact, one study found 89% of the pediatric patients were bed- or wheelchair-bound or required assisted ventilation.
In this case report, Colot et al. provides evidence that the clinical presentation of neuroborrelial transverse myelitis differs from classical TM.
“TM secondary to Lyme disease is more often subacute with gait preservation and is limited to the cervical spine,” the authors wrote.
Lyme disease triggers inflammation in spinal cord
A 10-year-old boy presented to his pediatrician with “persistent nocturnal and rotational neck pain with irradiation in the upper limbs for 13 days with a feeling of heaviness and paresthesia in the fingers.”
The boy also had a fever for 11 days, along with fatigue and headaches.
MRI findings of the spine suggested longitudinal extensive transverse myelitis (LETM).
“A spinal MRI showed an extensive T2 hypersignal between C1 and C7, with a normal T1 signal confirming the diagnosis of LETM.”
An extensive workup was performed using blood serologies and autoimmune factors. A CSF analysis found an increased white blood cell count in cerebrospinal fluid.
“The patient was treated with high-dose methylprednisolone IV for 5 days and Ceftriaxone IV,” the authors wrote. After 48 hours, the boy’s symptoms decreased, his CSF bacterial culture was negative and Ceftriaxone was stopped.
He remained on steroids but 2 days later, his neck pain and laterocollis (head tilted to one side) reappeared.
“Our case illustrates that neuroborrelial TM should be treated with long-term [antibiotic] therapy and that steroids do not seem to improve the prognosis.”
Since the patient lived in a tick-endemic area, he was tested for Lyme disease.
“The test results of Borrelia IgG in the blood and intrathecal IgG synthesis were positive, confirming the diagnosis of TM secondary to Lyme disease,” the authors explained.
“The patient reported that he had an erythematous spot in the neck a few months back, which was suggestive of an erythema migrans, but he did not remember that he had suffered from a tick bite,” the authors explained.
After 23 days of treatment with Ceftriaxone and Doxycycline, the patient made a complete recovery.
Authors Conclude:
“After an extensive review of the pediatric literature, we wish to emphasize five aspects of TM secondary to Lyme disease:”
presentation is more often subacute
lesions are mainly located in the cervical spine
gait is usually preserved
sphincter dysfunction is unusual
recovery is usually complete after prolonged antibiotic therapy
The authors suggest: “[Transverse myelitis] in a subacute presentation, gait preservation, a discrepancy between the severe mainly cervical imaging manifestations and the minimal clinical signs and symptoms, and the absence of sphincter dysfunction should raise suspicion of TM secondary to Lyme disease.”
References:
Colot C, Adler C, Mignon C, De Leucio A, Jissendi P, Fonteyne J, Aeby A. Case report: Subacute transverse myelitis with gait preservation secondary to Lyme disease and a review of the literature. Front Pediatr. 2023 Mar 16;11:1064234. doi: 10.3389/fped.2023.1064234. PMID: 37009275; PMCID: PMC10061057.
_______________
**Comment**
This patient, like all others presented in the literature, needs extensive follow-up, which never happens in mainstream medicine and/or research. My hunch is this poor kid will have symptoms later on that will never be connected to this event. I pray I’m wrong.
Further, nothing is mentioned about coinfections, which are the norm not the exception.
Tick-borne Powassan virus is being transmitted in concentrated clusters in New England, Yale study says
YALE SCHOOL OF PUBLIC HEALTH
April 11, 2023
By Jenny Blair, Yale School of Public Health
For New Englanders, tick-borne infections are a fact of life. Lyme disease, a bacterial infection carried by the deer tick, was first described in Connecticut in the 1970s and remains a major problem.
But deer ticks transmit other diseases to humans as well, including anaplasmosis, babesiosis, and an emerging virus called Powassan. Cases of Powassan virus have risen dramatically in recent years in the United States, mostly in the Northeast and Great Lakes region.
Most people infected with Powassan do not experience symptoms, but for some, it can result in brain swelling and even death. There are currently no vaccines or treatments for Powassan virus infection. Prevention is primarily dependent on education and control.
In a new study, researchers at the Yale School of Public Health provide insights into the transmission dynamics of the Powassan virus that could help focus public health efforts and limit infections. The study found that the virus appears to be highly localized in its spread, meaning that the virus is maintained in scattered local hotspots with very limited mixing between hotspot sites.
“It’s incredibly important to do surveillance to know what’s out there,” said Chantal Vogels, a research scientist in the Department of Epidemiology of Microbial Diseases at the Yale School of Public Health (YSPH) and a co-first author of the study.
By greatly expanding on what little genomic information scientists had before our study, Vogels said, “we were able to explore patterns of transmission and spread and unravel the ecology of the virus.”
Mapping viral spread
The team studied 279 samples of Powassan virus lineage 2 found in deer ticks (Ixodes scapularis, also called black-legged ticks) collected in Connecticut, New York, and Maine between 2008 and 2019.
By deciphering and comparing the virus’s complete genetic codes, or genomes, the researchers reconstructed the history of Powassan in the region. They estimated when branches of the virus’s “family tree” diverged and pieced together how the virus evolved and where it traveled via its hosts.
It’s incredibly important to do surveillance to know what’s out there.
Sometime between 1940 and 1975, a major branch of the lineage 2 virus appeared in the Northeast. This branch of the virus, which accounts for most Powassan cases in North America, first appeared in southern New York State and Connecticut. Then, several long-distance jumps occurred, likely when infected ticks caught rides on migrating birds or other vertebrate hosts. By 1991, it had reached Maine. During its initial decades in the region, Powassan became more populous in the wild, but this probably leveled off about 2005.
The virus now appears to be moving slowly or staying put, simmering in specific hotspots, and evolving independently in each one. For instance, the scientists could find no evidence that separate clades of the virus were mingling with each other across a 20-kilometer (or approximately 12.5 miles) stretch between two Connecticut sites. The scientists note, however, that they sampled only a limited number of locations, so it’s possible they missed hotspots.
Still, this new information could help health officials to target those hotspots, where Powassan is more likely to spill over into humans, for education and eradication efforts.
“If it’s anything like [the related] tick-borne encephalitis virus, [previous researchers have] estimated that these foci are typically about the size of a football field,” said Doug Brackney, a researcher in the Department of Entomology at The Connecticut Agricultural Experiment Station, and an assistant clinical professor in the Department of Epidemiology of Microbial Diseases at YSPH.
A quiet menace
Researchers first identified the virus in 1958 in a five-year-old boy from Powassan, Ontario, who developed severe encephalitis and died. After that, about one case per year was diagnosed until 2006. Then cases began to climb, and since the late 2010s dozens of diagnoses have been made nearly every year.
Given that the virus’s numbers appear to have leveled off in the wild, this increase in human disease may have happened because more humans are encountering ticks, and/or because more health professionals are checking for Powassan in patients with suspicious symptoms.
Unlike Lyme disease, which takes hours to pass from an infected tick to a human, Powassan can be transmitted just 15 minutes after the tick latches on. More New England residents have likely been infected with Powassan than have shown symptoms.
“We typically only see the most severe cases of disease, and those are the people that end up in the hospital. But it’s probably just the tip of the iceberg,” Vogels said.
“I think it’s really important to be early with this work,” she added, “to prevent a situation where everyone has heard of this virus, and it creates a huge burden on public health.”
The study’s four co-first authors are Vogels; Brackney; Alan P. Dupuis II of the New York State Department of Health (NYSDOH) and the State University of New York (SUNY) at Albany; and Rebecca M. Robich of the MaineHealth Institute for Research (MHIR).
The five co-senior authors are Robert P. Smith of MHIR; Philip M. Armstrong of The Connecticut Agricultural Experiment Station (CAES); Alexander T. Ciota of the New York State Department of Health (NYSDOH) and SUNY Albany; Simon Dellicour of KU Leuven and Université Libre de Bruxelles, both in Belgium; and Nathan D. Grubaugh of the Department of Epidemiology of Microbial Diseases, Yale School of Public Health, and the Department of Ecology and Evolutionary Biology, Yale University.
Other co-authors are Joseph R. Fauver of the Yale School of Public Health and the University of Nebraska Medical Center; Anderson F. Brito of the Yale School of Public Health and Instituto Todos pela Saúde, São Paulo, Brazil; Scott C. Williams and John F. Anderson, both of CAES; Charles B. Lubelczyk of MHIR; Rachel E. Lange and Laura D. Kramer, both of NYSDOH and SUNY Albany; Melissa A. Prusinski of NYSDOH; Jody L. Gangloff-Kaufmann and Laura B. Goodman, both of Cornell University; and Guy Baele of Belgium’s KU Leuven.
The research was funded by the National Center for Advancing Translational Science, a component of the National Institutes of Health (NIH), and the National Institute of Allergy and Infectious Diseases of the NIH. Baele received funding from Internal Funds KU Leuven and the Research Foundation – Flanders. Dellicour received funding from the Research Foundation – Flanders, the Fonds National de la Recherche Scientifique, and European Union Horizon 2020.
_______________
**Comment**
Wisconsin is a hotspot for Powassan as well. It also is not rare. Again, this is an issue of it being “rarely reported.” Big diff.
Coppe Lab, a CLIA certified lab, right here Waukesha has been studying Powassan for quite some time. Their pdf below states that numbers look low because only severe cases are reported. Despite this, there’s been a 375% increase in the last 5 years.
They state the clinical picture of Powassan looks like many other tick-borne illnesses and is…
PROBABLY OVERLOOKED YET DIRECTLY CONTRIBUTES TO DISEASE LONG TERM.
About two-thirds are subclinical cases but around 30% of symptomatic adults contract a severe form called meningoencephalitis. One-third of those have incomplete recovery with neuropsychiatric symptoms that become chronic. The overall fatality rate is about 1% and severity of illness increases with the age of the patient.
https://wwwnc.cdc.gov/eid/article/23/8/16-1971_article A study in Marshfield, WI showed that when 95 patients were tested for suspected tick-borne disease, 66% showed evidence of current or prior Lyme infection. Of those patients, 17% had serologic evidence of acute POWV infection, demonstrating that POWV may affect more patients than we know.
Coppe states the following patients should be tested for POWV:
Patients with a recent tick bite. Studies have shown 2–9% of ticks to be infected with POWV in Lyme endemic areas.
Patients with Lyme or another tick-borne illness who have been treated with antibiotics and have persistent symptoms consistent with post-treatment Lyme disease.
Patients with tick exposure who have tested negative for Lyme disease or other tick-borne illnesses who continue to have symptoms.
Patients with tick exposure and unexplained neurologic symptoms.
Chronic Fatigue Syndrome (CFS) or Post-Infectious Fatigue (PIF) patients with tick exposure.
But don’t worry. There are a variety of things you can do to keep yourself and your pets safe from these pesky bloodsuckers, starting with knowing what types of ticks live in North Carolina.
Black legged tick, aka the deer tick (Lyme disease)
The lone star tick (STARI, ehrlichiosis, Alpha-gal allergy)
The American dog tick (Rocky Mountain Spotted Fever)
The brown dog tick
Check out your own state’s resources for local ticks and the diseases they carry, but one word of caution: just because something hasn’t been reported, doesn’t mean it doesn’t exist or can happen. A tick, is a tick, is a tick and ALL are suspect as they bite and exchange bodily fluids with whomever and whatever they bite. Ticks are constantly moving and being found in places they shouldn’t be, carrying things they shouldn’t have.
The website points out the following and I’ve added more:
Black legged tick (Lyme disease, Anaplasmosis) – for some reason they forgot Powassan or Deer tick virus, Borreia miyamotoi, Bartonella, Babesia, Mycoplasma, Tularemia, Ehrlichia muris eauclairenis,hemocytic rickettsia-like organisms, tick paralysis from fully engorged female
lone star tick or seed tick (Ehlichia chaffeensis, Ehrlichia ewingii, Alpha-gal allergy – they have found Lyme in it but no reported cases. They also suspect rickettsia) for some reason they forgot STARI, tularemia, Anaplasma, Rickettsia amblyommatis, tick paralysis)
American dog tick or wood tick (RMSF, tularemia – they have found Lyme in it but no reported cases) for some reason they forgot Anaplasma and tick paralysis.
brown dog tick (RMSF) can also transmit Ehrlichia canis, Babesia canis vogeli, Babesia gibsoni-like to dogs which makes them suspect for humans as well. Source
For some reason there’s been a continual downplaying of where ticks are and what they carry.Prudence would err on the side of caution, but it simply doesn’t regarding Lyme/MSIDS. Take EACH and EVERY tick bite as seriously as a heart attack. If bitten, go here for excellent advice.
While the original article was written for North Carolina, please know that those bitten by ticks in the South have been ignored, denied, and gas-lit for decades. These folks are denied diagnosis and treatment and are told it can’t be Lyme/MSIDS because it doesn’t exist there despite the fact migrating birds are dropping ticks virtually everywhere and the fox, deer, mouse, lizard, and 1,000 other carriers are crossing state borders daily. It’s also important to note that tick researchers admit to tweaking ticks in the lab with the CIA dropping them out of airplanes. Independent researchers that aren’t conflicted due to government grant money admit that ticks are being found in places they never existed before, carrying things they never had before.
I am greatly alarmed as a study of feral dogs living in the Chernobyl Exclusion Zone were found to be rapidly mutating/evolving. The reason for the alarm is the WHY! Once again, we find that the Spike Protein of SARS-CoV-2 is MIMICKING IONIZING RADIATION – and in ways that directly cause mutations/evolution.
We found that 52 of the genes had associated Gene Ontology (GO) terms for the molecular functions of gene products that are of interest based on a putative response to the exposures from the Chernobyl disaster. These candidate genes were of particular interest because they are involved in functions such as DNA repair and cell cycle checkpoint progression, immune response, and calcium ion binding.
(See link for article and graphs)
_________________
SUMMARY:
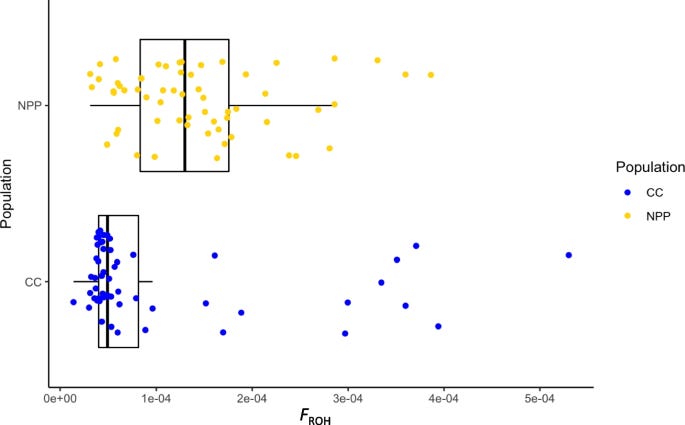
Chesnut references a study on wild dogs in the Chernobyl Exclusion Zone which found significant genetic differences between dogs occupying areas just 16 km apart due to ionizing radiation.
Regarding DNA repair, the Spike Protein of SARS-CoV-2 is MIMICKING IONIZING RADIATION – and in ways that directly cause mutations/evolution.
He takes an excerpt from that retracted paper which states that using an in vitro cell line, the spike protein inhibits DNA repair by impeding BRCA1 and 53BP1, which are required for adaptive immunity and that the protein localizes in the nucleus.
Chesnut states that viruses drive evolution and questions if this is being done with manufactured intent.
And all of this could now easily be put into the entire populace through the food supply.
It’s one thing to willingly consent to an experimental, fast-tracked gene therapy injection. It’s another thing entirely to put into the food supply without consent or knowledge.
100 Million animals have already been injected with mRNA technology, and hardly anyone knows about it. They’ve also injected it into vegetables.