
FDA Refuses to Enforce EUA Ad Restriction. ‘Vaccine’Coercion, Lockdowns, & Mask Mandates Need to be Criminalized – Make Manufacturers Liable For Injuries Again
https://rumble.com/v4i1b5x-fda-refuses-to-enforce-eua-advertising-restriction-but-also-insists-it-must.html Video Here (Approx. 2 Min)
FDA Refuses to Enforce EUA Advertising Restriction — But Also Insists it Must Keep the Provision!
During the pandemic, ICAN witnessed many instances where state and federal public health entities falsely referred to COVID-19 vaccines released under Emergency Use Authorization (EUA) as “approved” or “safe and effective” in direct violation of federal law and the conditions of the vaccines’ EUAs. ICAN’s attorneys sent two petitions to the FDA demanding it either enforce the terms of its own EUAs that prohibit advertisements with this illegal language or rescind the advertising restrictions entirely.
FDA chose to do neither.
Go here to see many other instances where ‘health’ agencies made unsupported claims to the public.
https://hillmd.substack.com/p/lawmakers-need-to-criminalize-vaccine? Video Here (Approx. 2 Min)
Criminalize vaccine coercion, lockdowns, and mandates of masks and shots now
The Covid bioweapon operation exposed vast lies by government and media about injections, masks, and lockdowns, injuring and killing millions and enriching a few overlords.
Action needed
Tell your congressperson and senator (who will probably ignore you) and your state legislators (who might pay attention) you insist they pass laws banning injection mandates.
And while you’re at it, tell them no more mask mandates or lockdowns, either.
[Sample letter with references: Letter to WI reps – Banning lockdowns, masks, shots copy]
If, unlike Covid jabs, future immunizations can confidently be shown to be safe, effective, and necessary in view of a significant threat, based on data and analysis that are fully transparent and verifiable by the public, then many will choose to take the shots.
But to coerce or require such shots must be made illegal.
This goes for schools and airlines too.
Impose mandates, go straight to prison. That must be the message.
Criminal law
Here is a sample draft statute for legislators:
Anyone who deprives a person of any right or privilege on the basis of whether that person has received, ingested, or had administered any medicine, therapy, medical procedure, prophylactic, vaccine, or immunization, or worn any mask or face covering, shall be guilty of a felony subject to imprisonment for not less than five years and a fine of up to $10,000.
Government officials or corporate executives found guilty under this section shall be subject to imprisonment for between 20 years and a life term.
(See link for article and videos)
______________
**Comment**
I highly recommend reviewing the words spoken in the videos in the above article where talking heads didn’t want the unvaccinated to sit next to them, to be able to buy food or to even to be able to receive needed medical help. This history must not be forgotten or downplayed or it will happen again. People should be ashamed of the heartlessly selfish words uttered.
SUMMARY: Just the facts
- The shots don’t reduce the spread, severity, hospitalizations, or death from COVID.
- The shots have caused more adverse reactions and death than any other ‘vaccine’ in the history of VAERS.
- The CDC just released a 148 page study on myocarditis after COVID shots – ALL REDACTED.
- Data continues to show that the more shots a person gets, the more likely they are to contract COVID and other respiratory diseases due to antibody dependent enhancement (ADE).
- Research shows the shots caused at least 17 million deaths.
- 98% have natural or ‘vaccine’ immunity to COVID.
- The CDC has downgraded COVID to the same severity as the flu.
- Yet, despite all of these facts, many people lost their jobs due to unethical ‘vaccine’ mandates.
- Many people took the gene therapy shots simply to keep their jobs, and were damaged or killed, yet there’s no end to the cover-ups.
- The unvaccinated were treated like second class citizens, animals, and even criminals and were prohibited from freely moving about and were fined and put in jail.
- People should be able to bring lawsuits for monetary damages against media personalities, journalists, and government officials who used their positions to deceive, coerce, defraud, bribe, threaten, or cajole them into taking injections that lead to injury. Shame on them.
That would include this lot among many others:
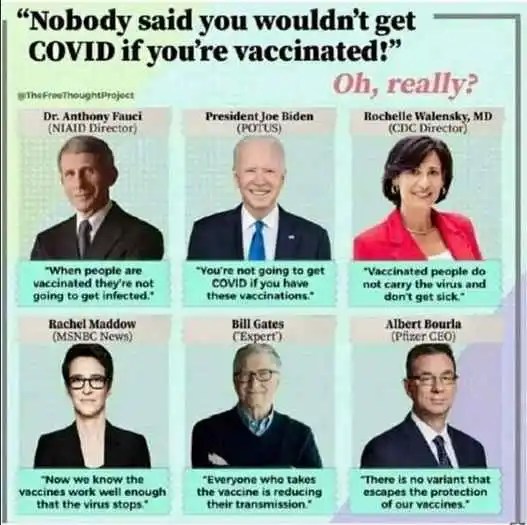

It is 2024 and there is STILL no cure or proven ‘vaccine’ for respiratory disease.
______________
https://childrenshealthdefense.org/defender/chip-roy-liable-act-covid-vaccine-manufacturers
New Law Would Make COVID Vaccine Makers Liable for Injuries, Deaths
Children’s Health Defense is among the organizations that support a bill introduced Tuesday by Rep. Chip Roy (R-Texas) that would remove the liability shield for manufacturers of COVID-19 vaccines and open the door for vaccine-injured Americans to sue companies like Pfizer and Moderna.
Rep. Chip Roy (R-Texas) on Tuesday introduced a bill that would allow Americans to sue the manufacturers of COVID-19 vaccines for vaccine-related adverse events, including deaths by removing the vaccine makers’ liability shield.
The Let Injured Americans Be Legally Empowered Act, or the LIABLE Act, would “allow Americans who took vaccines that were misleadingly promoted and forced onto many Americans via federal mandates to pursue civil litigation for their injuries,” according to a summary of the bill publicized by Fox News.
“These vaccines were given emergency use authorization unilaterally and did not go through the normal FDA [U.S. Food and Drug Administration] approval process,” the summary stated.
For more:
- https://madisonarealymesupportgroup.com/2018/02/28/corruption-in-fda-states-constitutional-attorney/
- https://madisonarealymesupportgroup.com/2018/10/05/drug-companies-pay-fda-nih-to-fast-track-market-vaccines/
- https://madisonarealymesupportgroup.com/2019/07/30/pharmaceutical-fraud-the-hidden-side-of-clinical-trials/
- https://madisonarealymesupportgroup.com/2019/03/18/fda-medical-adviser-congress-is-owned-by-pharma/
- https://madisonarealymesupportgroup.com/2022/08/10/insider-states-the-fda-has-lost-its-soul/
- https://madisonarealymesupportgroup.com/2023/10/17/action-alert-the-fda-legalized-censorship/
- https://madisonarealymesupportgroup.com/2022/02/17/fda-exec-biden-wants-to-inoculate-as-many-people-as-possible-almost-a-billion-dollars-a-year-going-into-fdas-budget-from-the-people-we-regulate-califf-to-head-fd/
- https://madisonarealymesupportgroup.com/2022/01/03/bidens-fda-chief-pick-used-to-work-as-big-pharma-consultant-has-millions-in-pharma-investments
- https://healthimpactnews.com/2022/obama-fda-head-that-allowed-opioid-crisis-to-increase-confirmed-to-lead-the-fda-again-as-covid-shots-set-to-join-annual-flu-shots-in-windfall-for-big-pharma/
- https://madisonarealymesupportgroup.com/2022/01/10/experts-weigh-in-after-suing-fda-for-access-to-pfizer-data/
- https://madisonarealymesupportgroup.com/2022/01/07/court-win-fda-must-produce-55000-pages-of-pfizer-injection-data-per-month/
- https://madisonarealymesupportgroup.com/2018/10/19/fda-official-uses-revolving-door-to-join-biotech-company-developing-mrna-vaccines/
- https://madisonarealymesupportgroup.com/2021/10/21/groundbreaking-nebraska-ag-says-doctors-can-legally-prescribe-ivermectin-hcq-for-covid-calls-out-fda-cdc-fauci-media-for-fueling-confusion-misinformation/


 Please note: Daylight Saving Time begins in the US, Canada, some parts of Mexico, etc. this weekend, making Monday’s show one hour later than previously.
Please note: Daylight Saving Time begins in the US, Canada, some parts of Mexico, etc. this weekend, making Monday’s show one hour later than previously.