https://www.lymedisease.org/cdc-chronic-lyme-iaccpac/
CDC now lists Lyme as infection that can cause chronic symptoms
A new page on the CDC website is headlined Chronic Symptoms Following Infections.
It goes on to say: “Infections can sometimes leave people with symptoms that last for weeks to months or longer, even after appropriate treatment.”
(I quibble with their use of “appropriate.” But I’ll leave that alone for now.)
Look what the CDC web page says next–and notice what’s at the top of the list:
Some disease agents that have been linked to chronic symptoms
- Borrelia burgdorferi (bacteria causing Lyme disease)
- Campylobacter
- Chikungunya virus
- Coxiella burnetii (bacteria causing Q fever)
- Dengue virus
- Ebola virus
- Epstein Barr virus
- Enterovirus
- Poliovirus
- SARS-CoV-2 (COVID-19)
- West Nile virus
Some people with chronic symptoms following infections may not know which infection triggered the symptoms, or even recognize that they had an infection before their chronic symptoms began. People with chronic symptoms and unknown preceding infection may be diagnosed with myalgic encephalomyelitis/chronic fatigue syndrome.
Why is this significant?
For years, the CDC and others in the medical establishment have been loathe to acknowledge that Lyme disease can turn chronic.
For a long time, the agency openly endorsed the IDSA Lyme treatment guidelines, which flatly deny that chronic Lyme exists. Even when the CDC removed the link to the IDSA guidelines from their website and softened some language, there was little support for the concept of persistent symptoms of Lyme disease.
Then along came COVID…
COVID-19 changed all that. Soon after the beginning of the pandemic, so many people began experiencing long-term symptoms of the illness that the term “long COVID” entered the national lexicon. Among the most prominent symptoms of long COVID were debilitating fatigue and brain fog–two symptoms also common in people with persistent Lyme disease, ME/CFS, and a host of other chronic conditions.
According to a 2022 CDC survey, nearly 18 million Americans have suffered from long COVID at some point since the pandemic began, and almost 9 million did at the time of the survey.
Those numbers were too big to ignore–and it opened the door for looking at other chronic conditions that shared symptoms with long COVID.
In June 2023, the National Academy of Science, Engineering and Medicine (NASEM), brought together high-level health officials, academic researchers, and knowledgeable patient advocates to look at the question of “infection-associated chronic illnesss.”
And just this past week, patient advocates that have joined IACCPAC–the Infection-Associated Chronic Conditions Patient Advocacy Coalition–held an online webinar introducing the coalition and its goals.
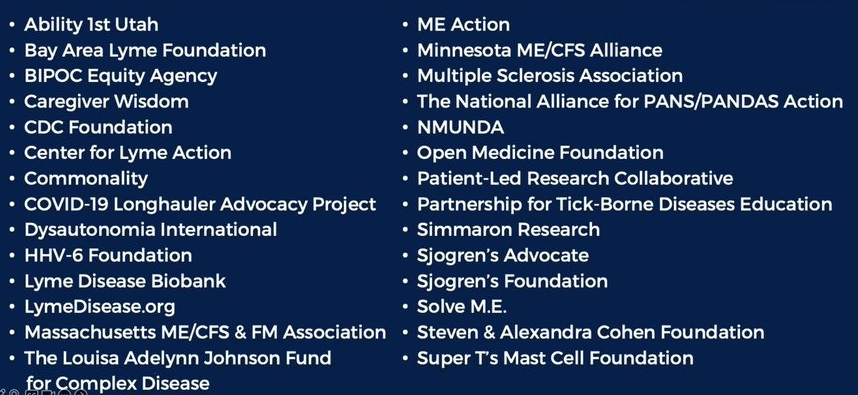
These are the groups currently involved in IACCPAC:
LymeDisease.org’s Lorraine Johnson was among the panelists at the IACCPAC workshop. She emphasized that patients can’t wait for decades-long studies to determine which treatments are best. It’s essential to accelerate research now.
The various conditions listed above are different in many ways, but they share many unique challenges. By working together, we’ll be able to accomplish things that are much harder to do individually.
I believe things are starting to shift. Stay tuned.
TOUCHED BY LYME is written by Dorothy Kupcha Leland, President of LymeDisease.org. She is co-author of When Your Child Has Lyme Disease: A Parent’s Survival Guide, and of Finding Resilience: A Teen’s Journey Through Lyme Disease. Contact her at dleland@lymedisease.org.
_______________
**Comment**
The only reason the CDC changes anything is if it benefits their bottom-line and their vested interests. Admitting diseases can be “chronic,” “persistent,” or “long haul” will assist their “vaccine” narrative – particularly using the mRNA platform. Rather than finding safe, cheap, repurposed drugs to help patients, or accurate testing, it will all be used for lucrative “vaccine” research and development.
I don’t expect much to happen from this, other than many Lyme advocates will continue to support government agencies that have only gas-lit and ignored patient suffering.
If you click on the Lyme link, it leads you here with the infamously biased title Post-Treatment Lyme Disease Syndrome. While it at least states that some experts believe it’s an auto-immune response while others hypothesize that PTLDS is from persistent but difficult to detect infection, while yet others believe it’s due to other causes unrelated to Borrelia burgdorferi infection, here’s the kicker:
Studies funded by the National Institutes of Health (NIH) have found that long-term outcomes are no better for patients who received additional prolonged antibiotic treatment than for patients who received placebo. Long-term antibiotic treatment for Lyme disease has been associated with serious, sometimes deadly complications, as described in the links below. Patients with PTLDS usually get better over time, but it can take many months to feel completely well.
This right here means nothing is going to change. While long-term antibiotics may not be the answer for every Lyme/MSIDS patient, they saved my life, my husband’s life, and the lives of countless others, but due to this unchanging threatening verbiage – no mainstream doctor will dare to prescribe the very thing that could save lives.
I’m not a negative person, but I am a realist. A pig with lip-stick on is still a pig.
Don’t expect much from this other than gad-loads of money continuing to be spent on the wrong things – including “climate change.”
Just like Fauci told the government NOT to do autopsies on COVID deaths, and just like they made it illegal to analyze what was in the COVID injections, the very thing that could end the Lyme wars are chronic Lyme post-mortem studies, but mark my words: these will not be done.