Black-legged ticks, also known as deer ticks, are the species tick species most likely to carry Lyme disease. (Submitted by Vett Lloyd)
When science writer and journalist Brian Owens was approached by a publisher to write a book about Lyme disease, he was soon struck by how the history of the disease had some parallels to the COVID-19 pandemic.
The St. Stephen resident set out to write a resource guide to the tick-borne disease, but writing the book in the midst of the global outbreak brought a new perspective on his subject.
“There kept being reasons to mention COVID, beyond just marketing,” Owens said in an interview from his home.
And while the COVID-19 pandemic isn’t the focus of the book Lyme Disease in Canada, Owens said there are lessons from the past 18 months that could help people battling Lyme disease. (See link for article)
_____________________
**Comment**
A few points:
While the author states people struggle to get diagnosed and treated, he also states it’s “changing.” I would disagree. Very little has in fact changed,except more and more people are getting infected.
He points out that there is a completely different attitude by the public health community regarding people with long-term COVID, as they are immediately taken seriously, and are seen as partners, unlike long-term Lyme/MSIDS patients.
The author and a tick researcher in the article think the “effectiveness of COVID ‘vaccines’ could create more interest in a Lyme vaccine.” They obviously haven’t read anything but vaccine manufacturer propaganda as these COVID injections which aren’t vaccines aren’t effectiveat all. Break-through infections are only rising and more and more are dying from COVID that are fully “vaccinated.”
The author states that the previous Lyme vaccine was a “victim of strong anti-vaccine” reaction and that the company pulled it because it wasn’t profitable. Again, he must have missed the details of thousands of people struggling with debilitating Lyme-like symptoms after this vaccine. (People to this day contact me explaining they are still suffering from the vaccine’s effects). A new jab is in the works.
The tick researcher predictably blames climate change for growing tick populations. She must not be aware of her own countryman’s work that proves this tenet to be false. Ticks are impervious to weather.
The numbers listed in the above link concerning adverse reactions and deaths have greatly increased. The most current numbers are:
BETWEEN DEC. 14, 2020 AND AUGUST 20, 2021, THE FOLLOWING WERE REPORTED TO VAERS:
623,343 ADVERSE EVENTS
56,654 HOSPITALIZATIONS
14,104 LIFE THREATENING REACTIONS
13,627 DEATHS
393 BIRTH DEFECTS
982 MISCARRIAGE OR PREMATURE BIRTH
Go here for a mounting list of adverse reactions and deaths as well as much more data and pertinent information to know.
UK Scientists and doctors at the Evidence-based Consultancy (EBMC) state, “the MHRA now has more than enough evidence on the Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans.” The letter concludes with an ominous warning, stating that “Preparation should be made to scale up humanitarian efforts to assist those harmed by the COVID-19 vaccines and to anticipate and ameliorate medium to longer term effects. As the mechanism for harms from the vaccines appears to be similar to COVID-19 itself, this includes engaging with numerous international doctors and scientists with expertise in successfully treating COVID-19.”
An Irish doctor states these injections are ‘killing people’
An occupational therapist working in three COVID units states shots are killing more people than COVID
A pathologist and a doctor are asking for autopsies due to the high rate of vaccine-related deaths
A group of doctors have written a paper stating these experimental, fast-tracked injections are “unnecessary, ineffective, and unsafe”
A Pfizer whistleblower confirms the injection is a bioweapon
A cardiologist and a Juris Prudence Doctor of Law states the injections are the genetic code of the COVID-19 bioweapon which causes damage to the heart and makes your body a spike protein factory
A pathologist states the results of a study show that the “vaccinated” may be able to cause harm to the unvaccinated through shedding via sweat glands (perspiration)
A pathologist states, “This is a poisonous attack on our population and it needs to stop now!” (spike protein is a toxin that crosses the blood, brain barrier causing inflammation and heart damage)
CDC whistleblower states the true number of deaths is over 50,000
Nobel Prize winner states COVID injections don’t stop the virus but in fact drive variants. He calls mass vaccination programs a “scientific error as well as a medical error”
Another vaccine researcher states the injections will cause a steep incline in severe COVID
Medical doctor states COVID injections are increasing new infections and deaths
COVID jabs are mandated for the military despite the fact only 26 soldiers have died from COVID as of the end of June. A study on the military has linked heart inflammation to the COVID shots. Dr. states, “The vaccine program has ostensibly killed more of our young active duty people than COVID did”
Group of doctors have written a paper stating the COVID injections for children are ‘unnecessary, ineffective, and unsafe‘
Doctor states, “COVID-19 ‘vaccination’ is greatest threat humanity ever faced” and “violates the Nuremberg codex, such that everyone who is propagating their use should be put before tribunal.” He states the injections showed ‘absolutely zero benefit in clinical trails‘ and even failat reducing severity of infection symptoms
A July 1, 2021, commentary in The Lancet Microbe, Piero Olliaro, Els Torreele and Michel Vaillant also argue for the use of absolute risk reduction when discussing vaccine efficacy. They determined the following efficacy rate for each injection:
Irish Medical Doctor: The Shots are Killing People! We need to Stop This! Her Medical License was Just Suspended
Aug. 24, 2021
by Brian Shilhavy Editor, Health Impact News
An Irish medical doctor who had just worked all night in the hospital took time to give an impassioned plea to stop the COVID-19 injections. She states that other than the children, for whom the shots are not yet authorized, almost everyone she treated had two doses of COVID-19 shots.
She states that she is seeing things that in all her years of practice she has never seen before, such as blood clots in the arm of a young girl in her 20s. Nobody is linking these injuries to the vaccines.
She states that the hospitals are short staffed because nurses are quitting, as they do not want to get the jab.
“The shots are killing people,” she states, and “We need to stop this!”
“I would take one of these vaccines, in fact all 4 of them, every hour on the hour, in all my four limbs, if they would just leave our children alone.”
NORTHERN Ireland’s most senior doctor last night said he was “personally appalled” by the anti-vaccine video posted by a Derry GP who has been suspended from practicing medicine.
Dr Anne McCloskey, a former Aontú councillor, expressed concerns in a social media video about young people being given the vaccine.
Chief Medical Officer (CMO) Sir Michael McBride also warned of the “great distress” caused by comments made by Dr McCloskey on social media after she inferred vaccinations were causing young people to become seriously ill- and falsely claimed “unapproved” vaccines were an “experimental genetic therapy”.
Following complaints by GP colleagues about the weekend post, the Health and Social Care Board (HSCB) yesterday moved to suspend Dr McCloskey as a “precautionary measure” as an investigation continues into “complaints and concerns against this doctor”.
The veteran GP retired in 2019 after more than 30 years working in the Shantallow area of the city but returned to the health service last April in response to the pandemic workforce appeal.
Dr McCloskey has been based in an out-of-hours GP centre in Derry for more than a year. (Source.)
This is what happens when you expose the Globalists’ agenda. Now it’s time for the rest of us to follow her example, no matter what the cost!
It appears these conflict-riddled public health ‘authorities’ have yet again scammed the public into believing the FDA has “approved” a safe COVID “vaccine.” When one reads the fine print it becomes clear they are attempting to off-load injections they have in stock that science and VAERS have exposed as dangerous and ineffective against the Delta variant. These injections, under EUA, are still experimental and can be refused.
IF SOMEBODY ORDERS YOU TO GET THE VACCINE: ASK TO SEE THE VIAL. IF IT SAYS “COMIRNATY,” IT’S A LICENSED PRODUCT. IF IT SAYS “PFIZER-BIONTECH,” IT’S AN EXPERIMENTAL PRODUCT, AND UNDER 21 U.S. CODE 360BBB, YOU HAVE THE RIGHT TO REFUSE. IF IT COMES FROM MODERNA OR JOHNSON & JOHNSON (MARKETED AS JANSSEN), YOU HAVE THE RIGHT TO REFUSE.
The change the nameswitcheroo tactic has been done before with the AstraZeneca shots to attempt to hide the deadly nature of the injections. Rest assured, the reason they changed the name is due to the fact Pfizer has “insufficient stocks” of Comirnaty but plenty of the Pfizer-BioNTech jab (EUA, experimental product that can be refused due to its designation).
Please read the long list of mounting adverse reactions and death reported after receiving these fast-tracked injections that aren’t vaccines.
Flip–flop” Fauci is now calling for a nation-wide vaccine mandate, irrespective of previous infection or health status – pushing a “one-size fits all” narrative. Despite the well known scientific fact that natural immunity is always far-superior to vaccines, which Fauci even admitted pre-2019, our corrupt government and any organization that follows in lock-step has misrepresented and denied this plain, simple fact. People have lost their jobs. Soldiers have been kicked out of the military. Children have lost out on educations due to this injustice.
The collateral damage due to ignoring natural immunity can not be overstated.
Of course, FDA approval was needed first, and remains cloaked in a shroud of mystery and suspicion as approval happened in record time without any oversight.John F. Kennedy and Dr. Meryl Nass state:
“THE FDA’S CLEAR MOTIVATION IS TO ENABLE PFIZER TO QUICKLY UNLOAD INVENTORIES OF A VACCINE THAT SCIENCE AND THE VACCINE ADVERSE EVENTS REPORTING SYSTEM HAVE EXPOSED AS UNREASONABLY DANGEROUS, AND THAT THE DELTA VARIANT HAS RENDERED OBSOLETE.”
According to U.S. Surgeon General Dr. Vivek Murthy, if you’ve already recovered from a bout of COVID-19, the immunity mounted by your body may not be enough to prevent reinfection with the Delta variant, so your best bet is to get the COVID shot
August 6, 2021, the U.S. Centers for Disease Control and Prevention published a case control study claiming that unvaccinated people are “more than twice as likely to be reinfected with COVID-19 than those who were fully vaccinated after initially contracting the virus”
One of several drawbacks of this study is that it did not look at illness severity. It doesn’t tell us whether more vaccinated people were symptomatic than the unvaccinated, or vice versa
A far better gauge of how well the COVID jabs are working would be serious infection, hospitalization and death rates, and when we look at those, a different picture emerges
In Israel — where data suggest those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection — a majority of serious cases and deaths are occurring among those injected with two doses of Pfizer’s mRNA jab
According to U.S. Surgeon General Dr. Vivek Murthy, if you’ve already recovered from a bout of COVID-19, the full-spectrum immunity mounted by your body may not be enough to prevent reinfection with the Delta variant, so your best bet is to get the COVID shot. Mid-August 2021 he told CNN:1
“… what we’ve understood, actually, from the studies about natural immunity, we are seeing more and more data that tells us that while you get some protection from natural infection, it’s not nearly as strong as what you get from the vaccine, especially with the Delta variant, which is the hardiest and most contagious variant we’ve seen to date. We need all the protection that we can get. That’s why the vaccines are so effective.”
Data Analysis Claims Unvaccinated More Prone to Reinfection
August 6, 2021, the U.S. Centers for Disease Control and Prevention published a case control study2,3 claiming that unvaccinated people are “more than twice as likely to be reinfected with COVID-19 than those who were fully vaccinated after initially contracting the virus.”
The study used data reported to Kentucky’s National Electronic Disease Surveillance System (NEDSS) to assess SARS-CoV-2 reinfection rates in Kentucky during May through June 2021 among those who’d had confirmed SARS-CoV-2 infection between March and December 2020.
The NEDSS data were then imported into a REDCap database that tracks new COVID-19 cases. A case-patient was defined as a resident with laboratory-confirmed SARS-CoV-2 infection in 2020 and a subsequent positive test result during May 1, 2021, through June 30, 2021.
Vaccination status was determined using data from the Kentucky Immunization Registry. Patients were considered fully vaccinated if a single dose of Johnson & Johnson or a second dose of an mRNA vaccine (Pfizer or Moderna) had been administered at least 14 days before reinfection. Compared to fully vaccinated residents, unvaccinated residents were 2.34 times more likely to test positive for SARS-CoV-2 reinfection.
The Obvious Flaw in CDC’s Study
The elephant in the room, however, is the absence of actual symptomatic illness. The study only looked at positive test results, and we do not know whether more vaccinated people were symptomatic than the unvaccinated, or vice versa.
As has been explained many times before, a positive test result is not the same as active infection. A person with natural immunity may be re-exposed to the virus, and traces of it may show upon testing, but their immune system has effectively killed the virus and prevented illness.
So, merely looking at positive test results is not the best way to ascertain whether the COVID jab actually provides better protection than natural immunity. And there are many reasons to suspect that it does not.
Other Shortcomings
The study authors also admit there are several other limitations to the findings, including the following:4
“First, reinfection was not confirmed through whole genome sequencing, which would be necessary to definitively prove that the reinfection was caused from a distinct virus relative to the first infection …
Second, persons who have been vaccinated are possibly less likely to get tested. Therefore, the association of reinfection and lack of vaccination might be overestimated.
Third, vaccine doses administered at federal or out-of-state sites are not typically entered in KYIR, so vaccination data are possibly missing for some persons in these analyses …
Fourth, although case-patients and controls were matched based on age, sex, and date of initial infection, other unknown confounders might be present. Finally, this is a retrospective study design using data from a single state during a 2-month period; therefore, these findings cannot be used to infer causation.”
It is correct that association does not equate to causation, and we’ve been repeatedly told to dismiss Vaccine Adverse Event Reporting System (VAERS) data for this very reason. Perhaps the same standard should be applied to this CDC investigation, as it tells us very little about the actual risk associated with reinfection.
For all we know, those with natural immunity tested positive for reinfection but had no symptoms, while vaccinated people tested positive and were actually ill. Which, in that case, would be the preferable outcome?
Hospitalization and Mortality Rates Are a Better Gauge
A far better gauge of how well the COVID jabs are working would be serious infection, hospitalization and death rates, and when we look at those, a different picture emerges.
In Israel, where vaccine uptake has been very high due to restrictions on freedom for those who don’t comply,5 data show those who have received the COVID jab are 6.72 times more likely to get infected than people who have recovered from natural infection.6,7,8
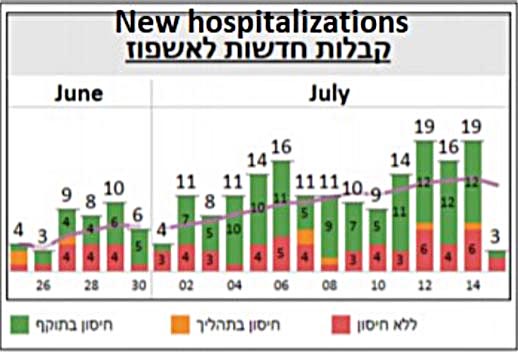
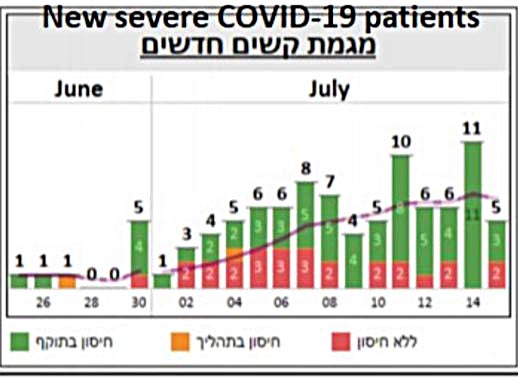
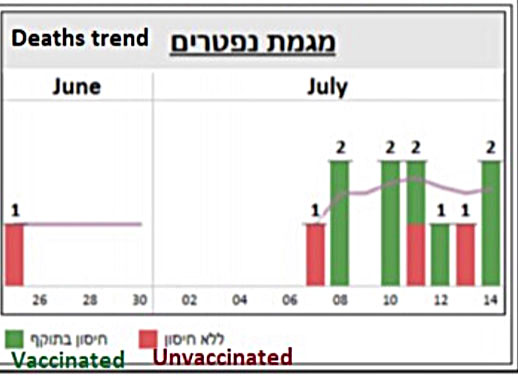
That too refers to test results, so let’s look at hospitalization rates instead. Here, we find a majority of serious cases and deaths are in fact occurring among those injected with two doses.
The following is a screenshot of graphs posted on Twitter.9 The red is unvaccinated, yellow refers to partially “vaccinated” and green fully “vaccinated” with two doses. The charts speak for themselves.
Do not be deceived by claims that unvaccinated patients make up 99% of COVID-19 deaths and 95% of COVID-related hospitalizations in the United States.10
These statistics were manufactured by looking at hospitalization and mortality data from January through June 2021 — a time frame when COVID jab rates were low. January 1, 2021, only 0.5% of the U.S. population had received a COVID shot so, clearly, unvaccinated made up the bulk of COVID-related hospitalizations last winter. By mid-April, an estimated 31% had received one or more shots,11 and as of June 30, just 46.9% were “fully vaccinated.”12
Why COVID Shot Cannot End COVID Outbreaks
Overall, it doesn’t appear as though COVID-19 gene modification injections have the ability to effectively eliminate COVID-19 outbreaks, and this makes sense, seeing how it’s mathematically impossible for them to do so.
The four available COVID shots in the U.S. provide an absolute risk reduction between just 0.7% and 1.3%.13,14 (Efficacy rates of 67% to 95% all refer to the relative risk reduction.) Meanwhile, the noninstitutionalized infection fatality ratio across age groups is a mere 0.26%.15
Don’t believe it? There’s proof. July 14, 2021, BBC News reported16 there’d been an outbreak on the British Defense aircraft carrier HMS Queen Elizabeth. Despite the entire crew being fully injected, 100 crew members tested positive. (It’s unclear whether any of them actually had symptoms.)
The recent outbreak onboard a Carnival cruise line ship is another example. All crew and passengers had presented proof of being jabbed, yet that didn’t prevent an outbreak from taking place.17
The reason is very simple. Just as we have been telling you from the beginning, the shot does not prevent you from getting infected with the virus or spreading it around.“Vaccinated” individuals have actually been shown to be just as infectious as unvaccinated people. Even if they have fewer or milder symptoms, their viral load is just as great when infected, according to the CDC.18
There’s No Control Group to Compare Against Anymore
For some reason, government leaders and health officials want a needle in every arm, and they don’t care what the side effects of the shots might be. This is evident by the fact that we now have tens of thousands of reported deaths (according to one whistleblower, 45,000 deaths have occurred within three days of injection19,20) and well over half a million injury reports following COVID “vaccination,”21 yet no action is taken to slow down or halt the campaign.
Historically, mass vaccination campaigns have been halted and drugs withdrawn after 25 to 50 deaths (depending on the product). We’re so far past that now, one wonders if there actually is a threshold at which authorities will take action to protect the public from unnecessary medical injury and death.
VAERS is tricky to maneuver, so the easiest way to get a glimpse into the current status is to go to OpenVAERS.com, where you get a simple summary breakdown of current COVID-related reports.
Equally telling is the fact that all control groups have been eliminated from the still-ongoing injection trials,22 with full support from a World Health Organization Expert Working Group23 so, in the end, we’ll have no way of really evaluating side effects.
This is the perfect way to hide the truth about these shots, and it violates the very basics of what a safety trial has always been required to have. You simply must incorporate a control group to compare the effects of the drug against in the long term, otherwise you will have no clue as to what complications have arisen.
Safety evaluations have also been intentionally undermined by the U.S. Food and Drug Administration, which chose not to require vaccine makers to implement robust post-injection data collection and follow-up on the general public.
On top of that, the trials also do not appear to have oversight boards, which is standard practice for all human clinical trials. There’s no Data Safety Monitoring Board, no Clinical Event Committee and no Clinical Ethics Committee. How could this be?
If vaccine makers simply forgot to follow standard practices, it would mean we’re dealing with a truly staggering level of incompetence, as all COVID jab developers have made the same mistake. Which might be worse in this case? Intentional negligence or unintentional incompetence?
COVID-19 Shots Confer Narrow Immunity
Getting back to the issue of whether the COVID jab actually confers better protection against SARS-CoV-2 and its variants, this is highly unlikely seeing how the shot confers a very narrow and specific kind of protection, whereas natural immunity is broad.
When it comes to SARS-CoV-2 — which is clearly a genetically manipulated virus designed to attack your cardiovascular system and basic immune function — the spike protein is the most dangerous part and acts as a toxin in and of itself. This is why the spike protein was chosen as the antigen in these shots, but it’s also why so many are having side effects from them.
When you get a COVID shot, your body is instructed to manufacture the spike protein. In response, your body then produces antibodies against that spike protein. Those antibodies recognize only the spike protein and not other parts of the virus.
When you recover from a natural infection, your body has antibodies against all parts of the virus, so the spike protein plus four other proteins. In addition to that, you have memory T cells, which appear even more important than antibodies when it comes to battling viruses.
Does it make sense that one type of antibody would be more effective against a virus that may have mutated one or more of its proteins? Or is it more likely that having several types of antibodies plus memory T cells will offer greater protection?
If you pay attention, you will find that no one ever offers a sensible explanation as to why a single anti-spike antibody would be better than T cells and antibodies against all parts of the virus.
Natural Immunity Is Robust and Long-Lasting
Many studies have been published demonstrating that natural immunity against SARS-CoV-2 is both robust and long-lasting. For example, a May 2020 study24,25 found 70% of samples from patients who had recovered from mild cases of COVID-19 had resistance to SARS-CoV-2 on the T-cell level.
Interestingly, 40% to 60% of people who had not been exposed to SARS-CoV-2 also had resistance to the virus on the T-cell level. According to the authors, this suggests there’s “cross-reactive T cell recognition between circulating ‘common cold’ coronaviruses and SARS-CoV-2.”
A German paper26 came to a similar conclusion. Here, they found helper T cells that targeted the SARS-CoV-2 spike protein in 15 of 18 patients hospitalized with COVID-19. Yet another study,27,28,29 this one by Singaporean researchers, found common colds caused by the betacoronaviruses OC43 and HKU1 might make you more resistant to SARS-CoV-2 infection.
What’s more, they found that patients who became infected with the original SARS virus back in 2003 still had memory T cell immunity against SARS-CoV-2, despite the virus being only 80% similar. This study suggests natural immunity is likely to last decades, not months, like the COVID shot.
Unvaccinated Falsely Accused of Being ‘Disease Factories’
While mainstream media are now pushing the idea that those who refuse the COVID shot are to blame for the emergence of SARS-CoV-2 variants, a number of health experts have warned that the complete opposite scenario would occur — that mass injections, causing a very narrow band of antibodies, will force more rapid mutations of the virus.30
A general principle in biology, vaccinology and microbiology is that if you put living organisms like bacteria or viruses under pressure, via antibiotics or antibodies, for example, but don’t kill them off completely, you can inadvertently encourage their mutation into more virulent strains. Those that escape your immune system end up surviving and selecting mutations to ensure their further survival.
If an individual who does not have a narrow band of antibodies becomes infected, then, if mutation does occur, it’s far less likely to result in a more aggressive virus. So, while mutation can occur in both vaccinated and unvaccinated people, vaccinated individuals are actually far more likely to pressure the virus into a mutation that strengthens it and makes it more dangerous.
CDC Misrepresents Data to Push Jab on Those With Immunity
So far, the CDC has refused to change its stance on the matter. Instead, officials at the agency seem to have doubled down and actually go out of their way to misrepresent data in an effort to harass those with natural immunity to inappropriately take the jab, which is clinically unnecessary and potentially dangerous.
In a report issued by the CDC’s Advisory Committee on Immunization Practices (ACIP) December 18, 2020, the Pfizer-BioNTech COVID-19 vaccine was said to have “consistent high efficacy” of 92% or more among persons with underlying medical conditions as well as among participants with evidence of previous SARS-CoV-2 infection.31
After looking at the Pfizer trial data, Rep. Thomas Massie — a Republican Congressman for Kentucky and an award-winning scientist — discovered that’s completely wrong. In a January 30, 2021, Full Measure report, investigative journalist Sharyl Attkisson described how Massie tried, in vain, to get the CDC to correct its error. According to Massie:32,33
“There is no efficacy demonstrated in the Pfizer trial among participants with evidence of previous SARS-CoV-2 infections and actually there’s no proof in the Moderna trial either … It [the CDC report] says the exact opposite of what the data says.”
After multiple phone calls, CDC deputy director Dr. Anne Schuchat finally acknowledged the error and told Massie it would be fixed.
“As you note correctly, there is not sufficient analysis to show that in the subset of only the people with prior infection, there’s efficacy. So, you’re correct that that sentence is wrong and that we need to make a correction of it,” Schuchat said in the recorded call.
January 29, 2021, the CDC issued its supposed correction, but rather than fix the error, they simply rephrased the mistake in a different way. This was the “correction” they issued:
“Consistent high efficacy (≥92%) was observed across age, sex, race, and ethnicity categories and among persons with underlying medical conditions. Efficacy was similarly high in a secondary analysis including participants both with or without evidence of previous SARS-CoV-2 infection.”
As you can see, the “correction” still misleadingly suggests that vaccination is effective for those previously infected, even though the data showed no such thing.
I don’t know why the surgeon general insists the COVID jab offers better protection against variants than natural immunity. I don’t see how it could. The lack of rational medical explanation is suspicious, and perhaps that’s why 40% of the American population has yet to take the jab.34
A new Israeli study came out showing natural immunity protects up to 13 times more than the jabs, and that the vaccinated are at a greater risk for COVID related hospitalizations.
“In COVID-19 patients, immune responses were characterized by a highly augmented interferon response which was largely absent in vaccine recipients. Increased interferon signaling likely contributed to the observed dramatic upregulation of cytotoxic genes in the peripheral T cells and innate-like lymphocytes in patients but not in immunized subjects.” “Analysis of B and T cell receptor repertoires revealed that while the majority of clonal B and T cells in COVID-19 patients were effector cells, in vaccine recipients clonally expanded cells were primarily circulating memory cells.”
In sum, those with natural immunity developed a quicker and more durable innate response.
“People who recover [even] from mild COVID-19 have bone-marrow cells that can churn out antibodies for decades.”
An in-vitro study in Singapore found the immunity against SARS-CoV-2 to last even 17 years later from SARS-1-infected patients who never even had COVID-19.
In a study of 1,359 previously infected health care workers in the Cleveland Clinic system, not a single one of them was reinfected 10 months into the pandemic, despite some of these individuals being around COVID-positive patients more than the regular population.
“Natural infection induced expansion of larger CD8 T cell clones occupied distinct clusters, likely due to the recognition of a broader set of viral epitopes presented by the virus not seen in the mRNA vaccine” (emphasis added).
“In infection-naïve individuals, the second dose boosted the quantity but not quality of the T cell response, while in convalescents the second dose helped neither. Spike-specific T cells from convalescent vaccinees differed strikingly from those of infection-naïve vaccinees, with phenotypic features suggesting superior long-term persistence and ability to home to the respiratory tract including the nasopharynx.”
This shows natural infection conveys a much stronger mucosal immunity making the recovered much safer to be around than the vaxxed. It is natural infection that conveys mucosal immunity. In fact, studies now show that infected vaccinated people contain just as much viral load in their nasopharynx as those unvaccinated, a clearly unmistakable conclusion from the virus spreading wildly in many areas with nearly every adult vaccinated.
“In vaccinated subjects, antibody titers decreased by up to 40% each subsequent month while in convalescents they decreased by less than 5% per month.”
In patients with supporting evidence of reinfection, researchers estimate the risk at 0.66 per 10,000 person-weeks. Most importantly, the study found no evidence of waning of immunity for over seven months of the follow-up period. The few reinfections that did occur “were less severe than primary infections.”
Israeli researchers studied 6.3 million Israelis and their COVID status and were able to confirm only one death in the entire country of someone who supposedly already had the virus, and he was over 80 years old. Contrast that to the torrent of hospitalizations and deaths we are seeing in those vaccinated more than five months ago in Israel.
Researchers tested blood samples from health care workers who never had the virus but got both Pfizer shots against blood samples from those health care workers who had a previous mild infection and a third group of patients who had a serious case of COVID. They found, “No neutralization escape could be feared concerning the two variants of concern [Alpha and Beta] in both populations” of those previously infected.
“Asymptomatic SARS-CoV-2–infected individuals are not characterized by weak antiviral immunity; on the contrary, they mount a highly functional virus-specific cellular immune response,” wrote the authors after studying T cell responses from both symptomatic and asymptomatic convalescent patients. If anything, they found that those with asymptomatic infection only had signs of non-inflammatory cytokines, which means that the body is primed to deal with the virus without producing that dangerous inflammatory response that is killing so many hospitalized with the virus.
“express increasingly broad and potent antibodies that are resistant to mutations found in variants of concern.” They conclude that “memory antibodies selected over time by natural infection have greater potency and breadth than antibodies elicited by vaccination.”
“in individuals with a pre-existing immunity against SARS-CoV-2, the second vaccine dose not only fails to boost humoral immunity but determines a contraction of the spike-specific T cell response…..the second vaccination dose appears to exert a detrimental effect in the overall magnitude of the spike-specific humoral response in COVID-19 recovered individuals.”
The biology behind ‘breakthrough’ cases and the confusing CDC mask guidance.
WSJ Opinion: Delta Shakes Up the Politics of Vaccines and Masking
Journal Editorial Report: Biden’s attacks on Govs. DeSantis and Abbott are a distraction. Image: Michael M. Santiago/Getty Images
By Michael Segal
The Centers for Disease Control and Prevention’s latest Covid guidelines have many Americans confused. Vaccinated people are supposed to resume wearing masks, lest they contract and spread the virus. Yet unvaccinated people are still strongly urged to get the shots, which are said to be highly effective. How can both these claims be true?
The answer is that there’s more than one kind of immunity. Internal immunity protects the inside of the body, including the lungs. This occurs by release of antibodies of the Immunoglobulin G type, or IgG, into the blood and production of T-cells. Vaccines injected into our muscles are highly effective at stimulating internal immunity. This largely protects vaccinated people from being overwhelmed by the coronavirus, unless they have an immunodeficiency or are exposed to an unusually large amount of the virus. Vaccination will dramatically reduce your likelihood of serious illness or death if you’re exposed to SARS-CoV-2.
In contrast, mucosal immunity provides the first line of defense by protecting the nose and mouth, and by doing so also reduces spread to others. The mucous membranes secrete a particular form of antibodies of the Immunoglobulin A type, or IgA. But vaccines injected into our muscles—including all the approved inoculations against Covid—are largely ineffective at stimulating the secretion of IgA into our noses that occurs after actual infection with a virus. As a result, vaccinated people can contract a Covid-19 infection confined to the mucous membranes. They may get the sniffles but can spread the virus to others even if they are asymptomatic. That’s why it makes sense for them to wear a mask under some circumstances. (See link for article)
_____________________
**Comment**
Summary of points:
An outbreak in Massachusetts showed similar nose viral loads in both the “vaxxed” & unvaxxed.
This demonstrates the “vaccine’s” efficacy in the nose has fallen to zero.
Herd immunity through vaccination is impossible.
Data from Mayo also shows “vaccine” efficacy against nasal infections has fallen.
Don’t shun the previously infected.
Exceptions should be made for those who have recovered from COVID since their natural immunity puts them “at less risk than never-infected ‘vaccinated’ people of spreading the virus.”
Absent from this article are the two huge elephants in the room:
Masks do not protect you from this “virus” as it’s smaller than the holes in the mask. There’s evidence they are dangerous to the wearer (especially over long periods of time) and actually harbor infections. They also lower the oxygen content of air you are breathing.
With three invasive tick species thriving in Connecticut, state scientist warns of major public health hazard
Stratford, Ct. – 08/13/2021 – Dr. Goudarz Molaei, with Connecticut’s Agricultural Experiment Station, searches for ticks trapped on a canvas dragged through shoreline vegetation. Photograph by Mark Mirko | mmirko@courant.com (Mark Mirko/The Hartford Courant)
State scientist Goudarz Molaei pulled a square of cloth through brush and grass on the Stratford coast recently, then stopped and pointed to a crawling smear of larvae on the white fabric.
The tiny arachnids were either Gulf Coast or lone star ticks, two of three invasive species, along with the Asian long-horned tick, that have recently established footholds in Connecticut.
First seen only in pockets near the coast, the blood-sucking, disease-carrying ticks have spread into other parts of the state. Compared with past years, many more worried residents and visitors have submitted ticks to the Connecticut Agricultural Experiment Station, mostly deer ticks that may carry Lyme disease, Molaei said. The tally so far in 2021 is 4,700 tick submissions to the testing laboratory, compared with a total annual average of 3,000 submissions.
Milder winters and warmer temperatures overall are helping the ticks survive and thrive in Connecticut.
“This is going to be a major public health concern in the near future, if it is not already,” Molaei said. (See link for article)
_____________________
**Comment**
Important takeaways:
Previously only .2% of submitted ticks were lone star ticks which increased to 4.2% this year. They transmit ehrlichiosis, STARI, spotted fever rickettsiosis, tularemia, Alpha-gal allergy, and Heartland and Bourbon Viruses.
The researcher states that it’s a matter of time before the entire state of Connecticut will be infested with Asian long-horned tick – the tick that can reproduce by cloning. It is supposedly less attracted to human skin but can spread diseases that make both animals and humans seriously ill.
The Gulf Coast tick overwintered successfully in Connecticut but currently is limited to coastal areas. Thirty percent tested there were infected with rickettsiosis, which is similar to but less serious than Rocky Mountain Spotted Fever.
The deer tick, or blacklegged tick transmits Lyme disease and is active any time temperatures are above freezing. All life stages bite humans.
The following percentages of ticks were sent to the Experiment Station this year:
72.8% deer ticks (32% were positive for Lyme, 10% for Babesia, 4% for Anaplasmosis – and 2% tested positive for at least 2 disease agents concurrently)