Petition: Vaccine Mandates For Air Travel
https://standforhealthfreedom.com/action/vaccine-mandates-wont-fly/ Sign Petition Here
Vaccine Mandates for Air Travel Won’t Fly
Why Sign This Petition
- A bad bill was filed to make it law that you must be vaccinated to fly. Bad bills die in committee. Sign this petition today to make it loud and clear Americans do not want forced vaccination to fly.
- Showing a big opposition to this bill, early in the legislative process, is the best way to stop it from getting to a vote.
- When signing this petition you will hold your representatives accountable for their oath to protect Constitutional rights. You will show them the formidable bloc standing against threats to our liberty. We are not going away, and they will have to answer to us again and again and again until they stand with us.
- Freedom to travel is a fundamental right and crucial for other rights such as who we visit, where we go, how we express ourselves. This bill especially impacts all airline workers, and those dependent on the industry. It would further entrench socioeconomic disparities by disproportionally affecting marginalized communities who are the least vaccinated Americans. You can support the economic livelihoods and Constitutional rights of millions by letting our representatives know you oppose H.R. 4980.
How Will This Petition Be Used?
- The petition will be delivered to the committee considering the bill when we reach 100,000 signatures. SHF’s team will watch this bill and let you know if or when it is time to contact your representatives again. Stay tuned for action alerts on this issue!
https://standforhealthfreedom.com/federal/experiment-consent-choice/ Go here for excellent, informative article on the following:
- FDA approval of Pfizer injection expected by Labor Day
- FDA approval will trigger vaccine mandates across the country, the military, entire cities, federal government, college campuses, etc.
- FDA approval gives doctors discretion in off-label uses like boosters or giving it to younger children
- America’s Frontline Doctors filed a lawsuit to halt EUA’s and FDA approval. CDC safety data is faulty.
- FDA approval typically takes 10-15 years with lab research preceding pre-clinical animal testing.
- Next, 20–100 healthy, unexposed, humans are recruited for Phase 1 studies of immune response and dosing.
- Phase 2, Randomized Control Trials, includes 100s of people of mixed health, age, and ethnicity, expanding to thousands for Phase 3.
- Safety is the primary focus early in the process, which gives way to a focus on efficacy and strategy for scalable manufacture. It is at this point that the vaccine candidate would have enough data to submit a Biologics License Application (BLA). Until the BLA is approved, the vaccine is experimental.
- Prior to COVID, the fastest vaccine development was in 4 years for the mumps.
- COVID shots, which aren’t vaccines, were authorized 1 year from the first known COVID case.
- mRNA technology for vaccines has never been used before.
- Software was used to design the candidates, rather than lengthy test-tube cultivation.
- Pfizer and BioNTech partnered to make flu shots in 2018 which haven’t come to market yet.
- Researchers combined phases, tested multiple candidates simultaneously, and manufactured them BEFORE authorization to further speed up the process.
The company had unexpected trouble enrolling patients. “[F]ewer subjects than expected had become sick,” perhaps due to health precautions or maybe, questioned lead scientist Dr. Jansen, “the FDA-authorized tests Pfizer was using to confirm cases weren’t accurate.”
Somehow the issue resolved itself and enough cases were confirmed. (You can dive deeper into the trials in a paper published by Dr. Henry Ealy with GreenMedInfo, on page 153 – entire 444 page document).
- Emergency Use Authorizations (EUA) were created to bypass FDA approval laws
- EUA law was created for off-label use of the Anthrax vaccine by the military. In response to losing a court case where service members objected to off-label mandates, President Bush signed Project Bioshield into law, bypassing the court ruling upholding FDA approval law, and creating EUAs in the process. x xi DoD was then able to administer the Anthrax vaccine off label (approval was for skin absorption, not inhalation). xii FDA had 64 years of data – 30 years of research and 34 years post market to scrutinize the Anthrax vaccine.
- EUAs, experimental treatments, and informed consent require an option to refuse. Law dictates a recipient understand the option to accept or refuse, along with the consequences of refusing.
- Arguments that COVID injections are not experimental is an attack on informed consent and right to refusal. They are legally and logically unsound.
- The DOJ asserted the option to refuse was itself an option for the government to offer and exercising the option could be met with serious consequences. (See SHF’s recent post, Is the Government Weaponizing Data?). A Texas court ruled that an employer mandate could stand because the employee had the option to refuse. The Plaintiff asserted she was being forced to take the jab or be fired. The court responded, “This is not coercion…[She] can freely choose to accept or refuse a Covid-19 vaccine; however, if she refuses, she will simply need to work somewhere else.” xix
- “My way or the highway” governance feels and looks like extortion.
- The injection experiment is happening this moment with all takers part of an ongoing trial. This is not just about an injection. It’s about civil rights with the constitution being bypassed.
Steps You Can Take
- Tell your governor and local legislators that COVID-19 vaccines must be voluntary! TAKE ACTION
- Stand with the Frontline Doctors by asking our legislators to call for an investigation into CDC data. Without trustworthy and replicable data, we cannot make informed decisions about our health. SIGN PETITION
Go to link for sources and references
For an informative article on the topic: https://articles.mercola.com/sites/articles/archive/2021/08/17/should-unvaccinated-be-put-on-no-fly-list.aspx
STORY AT-A-GLANCE
- In June 2021, the U.S. National Security Council released a new National Strategy for Countering Domestic Terrorism document. While it’s being largely framed as a tool to fight extremism, the definition of what constitutes a “domestic terrorist” is incredibly vague and based on ideologies rather than specific behaviors
- This policy can easily be used to silence political opposition simply by labeling anyone who disagrees with the government as a domestic terrorist and charging them with a hate crime, and we’re already seeing signs of this
- Dr. Peter Hotez recently published a paper in PLOS Biology, in which he suggests criticizing Dr. Anthony Fauci and other scientists ought to be labeled a “hate crime”
- Former assistant secretary for Homeland Security Juliette Kayyem is urging the U.S. government to put unvaccinated citizens on a no-fly list
- The San Francisco Chronicle editorial board believes we ought to “make vaccination the price of admission to society”
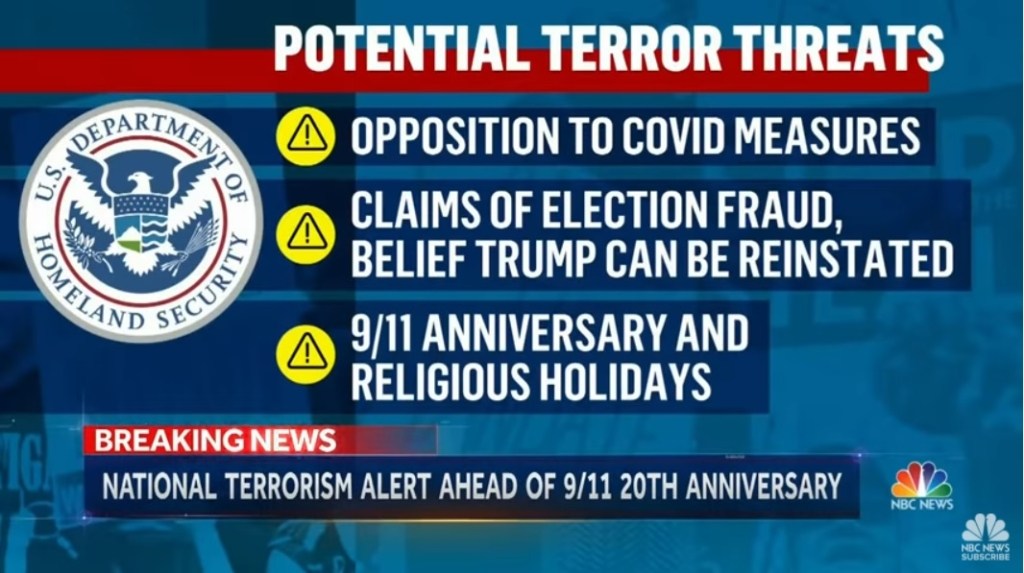
You are now considered a potential terror threat if you oppose COVID measures.
France has a message to the U.S.:
- Society is essentially closed to anyone who hasn’t taken the COVID jab with proof on a “Health” Pass.
- There is a 6-month prison sentence if you are caught without the pass.
- Businesses have closed their doors due to lack of staff as they can make more on welfare.
- All medical professionals have been mandated to take the jab or lose their license.
- Hospitals look like 3rd world hospitals as all the good doctors left the country 5 years ago and there’s no money for repairs.
- Nurses are doing double the work as the health care system is nearly bankrupt.
- All large retail stores requiring the jab and “health” pass.
- Truckers are going on strike nation wide blocking all access roads in and out of Paris.
- An airport closed due to a majority of staff quitting.
- As of Sept. 15, all public areas and access will be off limits.
- As of Oct. 1, all small venders will be off limits, which means people can only buy food via internet.
If you believe all of this to be too far-fetched for the U.S., please know President Biden is discussing setting up highway checkpoints to mandate “vaccines” for interstate travel.