New Study Supports Conclusion of Retracted 2020 Study Showing Unvaxxed Kids Healthier Than Vaxxed
A new study by James Lyons-Weiler, Ph.D. and Dr. Russell Blaylock supports the conclusions of a study by Dr. Paul Thomas, published in November 2020 and later retracted after an anonymous reader expressed concerns.
In November 2020, a study that carefully examined 10 years’ worth of data from a pediatric practice in Oregon run by Dr. Paul Thomas was published. Five days following the publication of the study, Thomas’ license was suspended.
A month after that, the journal decided to inform the authors that an anonymous reader had expressed some concerns about the study.
This single reader’s comments that involved bad guesswork led ultimately to the journal’s decision to retract the paper, leaving the authors stunned.
The authors knew that the reader’s concerns had already been addressed during peer review, and expected the journal to rule in favor of not retracting the paper. The journal editorial board knew this, too.
The concern centered primarily on the question of whether the large differences in the number of medical visits required for attention to specific health conditions like anemia, gastroenteritis, asthma, ear infections and many others, were due to parents who did not vaccinate not showing up to their well-baby and well-child visits.
Because Thomas’ license was suspended, he had to focus on his case and try to keep his life from falling apart; the medical board kept postponing the hearing, and no hearing had occurred.
In fact, no hearing has been held to date.
James Lyons-Weiler, Ph.D. suggested to Thomas that perhaps the medical board had overreached by applying a penalty without due process, a fact that Thomas then shared with his lawyer.
When his lawyer wrote the medical board pointing out that Thomas had suffered a penalty without due process, they offered to reinstate his license, pending the outcome of a hearing, on the condition that he do no more research.
This clearly shows the agenda of the medical board was not to ensure that the children in the practice were receiving good pediatric medical care.
It is now clear that the singular priority of the medical board was to shut down Thomas’ practice of abiding by informed consent — as required by Oregon state law for all medical procedures — and to prevent him from sharing any additional findings from the 10 years of data that had been collected from his practice.
New study supports earlier conclusions by Thomas
Today, the study is revived by a second study, this time conducted by Lyons-Weiler and his medical collaborator, Dr. Russell Blaylock.
In this second study, the following questions were addressed:
Which group of patients adhered to the regular well-child visit better, the vaccinated patients or those who had refused vaccines?
In groups of patients matched for health check visitation usage, which adverse health outcomes following vaccination differed between vaccinated patients and those who refused vaccines?
After adjusting for healthcare visitations and age, do vaccines still significantly affect overall adverse health conditions in a manner independent of their interaction with healthcare visitations and age?
Did older patients in the practice who stopped vaccinating experience a decrease in the adverse health outcomes that have been attributed to vaccines?
The study results, which are found in the paper entitled “Revisiting Excess Diagnoses of Illnesses and Conditions in Children Whose Parents Provide Informed Permission to Vaccinate Them” show that the anonymous reader’s concerns were unfounded; the unvaccinated families made their well-child visits with greater frequency than the vaccinated families.
The answer to the second question is “results vary,” but this may be due to smaller sample sizes reducing power (see the study for details).
The study split the patients into high, medium and low health care visitation usage blocks, and many of the adverse health effects are seen increased in the vaccinated group of patients within these blocks (blocks are groups of patients matched on health care visitation usage).
For the third question, the scientists found that after defining a model that included healthcare visit utilization and age, vaccines were still a significant factor that increased adverse health outcomes, many of which had previously been associated with vaccines.
Moreover, the authors also determined that vaccines were still significant following consideration of the interaction term between vaccination status and the other model factors.
Importantly, had the study authors not considered the interaction term, the results would have seemed to imply that vaccination was negatively predictive of adverse health outcomes.
In the model in which vaccines, health care visits per age and the interaction term was considered, the number of vaccines was a positive significant predictor of overall adverse health.
Interaction terms are usually ignored by studies that “adjust for” variables. Adding covariates into the model without considering the interaction term with the main effect — vaccines — can mask a significant effect on the rates of post-vaccination health issues, providing a misleading result.
It’s worth noting that breastfeeding — another correlate of lifestyle measures — had no significant singular or interaction effects.
Blaylock posed the final question to Lyons-Weiler, who conducted the data analysis.
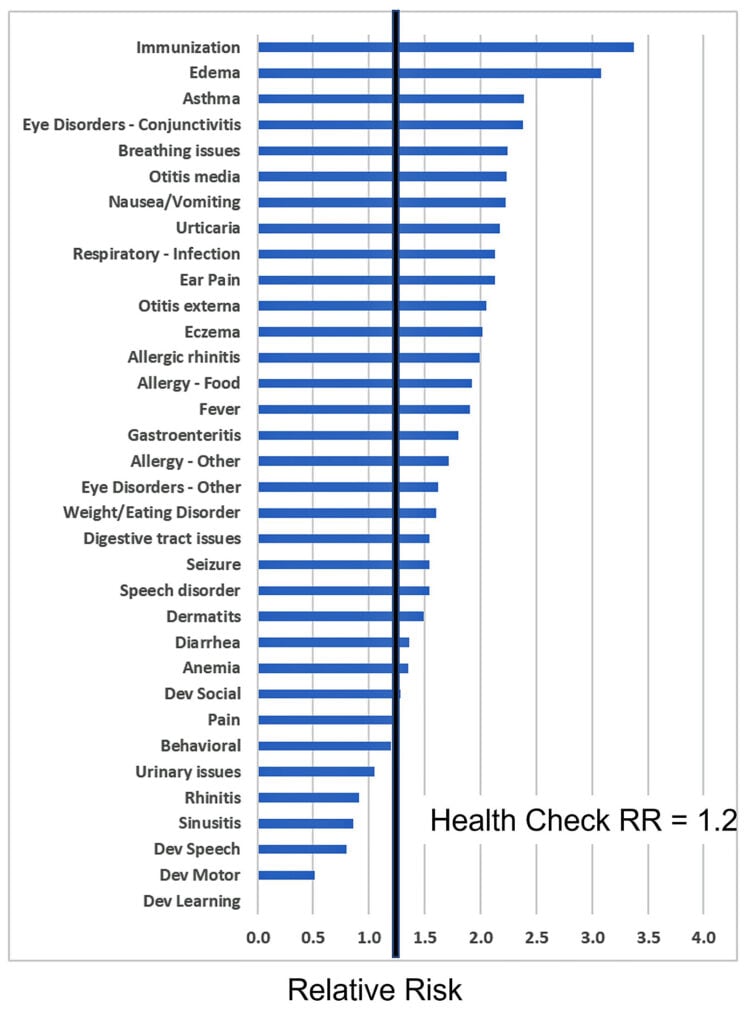
When older children were studied, and those who had the most vaccines were compared to those to those of the same age who had fewer vaccines, a clear pattern emerged for most of the adverse health outcomes: the risk of having a higher adverse health outcome was higher in the most-vaccinated older children compared to the least-vaccinated older children to a degree that was larger than that expected given any variation between the two groups in healthcare visit utilization.
The age-matched effects of vaccine cessation. High Relative Risk values denote increased risk of a given health outcome in patients receiving more vaccines in the older age group (>1,500 days of age). The black bar shows the Relative Risk of HCV between these groups as a baseline.
The relative risk of adverse health outcomes in older children who continued to vaccinate compared to those who ceased vaccination in Thomas’ practice.
Combined, all of these results mean that the method developed by Lyons-Weiler to consider the number of office visits needed for adverse health outcomes represents a robust, reliable and rigorous advance in methodology for the study of adverse health outcomes following medical exposures, including vaccines.
The method, “Relative Incidence of Office Visits,” had already been shown to be more powerful.
Lyons-Weiler reports that this is necessarily so because the measure contains more information than mere rates of diagnosis.
The RIOV measure has a higher dynamic range than odds ratios and relative risks based on diagnosis only. Studies that focus on the rates of diagnosis are using a subset of RIOV but are only limiting their count of office visits to that for the initial diagnosis.
The authors estimated that vaccination increases the need for visits to the doctor for vaccine-related health outcomes at a rate of 2.56 to 4.98 new chronic-illness-related visits per unit increase in vaccination per year.
“That translates into far more chronic illness in vaccinating children than in those not vaccinating, a disease burden that is not considered in risk: benefit considerations when it comes to vaccine policies and laws,” said Lyons-Weiler.
The views and opinions expressed in this article are those of the authors and do not necessarily reflect the views of Children’s Health Defense
Overall, kids in the study who received 3 mg or more of vaccine-related aluminum had at least a 36% higher risk of developing persistent asthma than kids who got less than 3 the study’s lead author, Dr. Matthew F. Daley, told The Associated Press. (See link for article)
It should be noted that the CDC has never done a study comparing the vaccinated with unvaccinated nor with children who weren’t exposed to aluminum at all in their vaccines. To date, the CDC has never studied the cumulative effects of all the vaccines together. Studies only look at one vaccine at a time typically compared to another vaccine (not a true placebo).
“The idea is to concede the smallest possible ground on aluminum toxicity and at the same time reinforcing what they want readers to think by citing multiple papers by stooges and those working directly for the aluminum industry — a classic example being where the authors look to reinforce that ingested aluminum is not a health issue in infants.”
Please read the entire article for all the details.
Also, please read James Lyons-Weiler’s take on it as well. Cox proportional hazard models were used to evaluate the association between aluminum exposure and asthma inci- dence, stratified by eczema presence/absence.
Raise your hand if you’re a parent and you have noticed that your child with eczema seems at risk of autoimmune conditions, including autoimmune diseases of the airways like persistent asthma when exposed to vaccines.
The risk was associated with vaccine-associated aluminum dose – and the increased risk was HUGE. “aHz of 1.26 per 1 mg increase in aluminum” means a 26% increase in the risk of asthma per 1,000 mcg aluminum-containing vaccine received. Children on the CDC’s schedule receive 5,640 mcg of aluminum by age 13, so children with eczema have a 78% increase in their risk of developing asthma by age 13 compared to kids who receive no aluminum-containing vaccines.
Kids without eczema had a 19% increase in asthma risk per 1 mg increase in vaccine-sourced aluminum; by age 13, they have a 57% increased risk of asthma compared to kids who receive no aluminum-containing vaccines.
He then proceeds to wipe the floor with Dr. Paul Offit, who is calling for “extraordinary evidence” which Weiler states means randomized controlled trials (RCTs) which will never happen (just like in Lymeland).
Comments Off on New Study Supports Conclusion of Retracted 2020 Study Showing Unvaxxed Kids Healthier Than Vaxxed & the Vaxxed Had a 36% Higher Risk of Asthma
There are some articles that are imperative reading. The following article is one such article. It goes through the entire Polio chronology and gives crucial history that is foundational for understanding not only Polio, but the corruption behind it and virtually every medical issue.
It’s important to understand the following facts about Polio which Big Media and the medical monopoly will never admit:
95% of people who contract Polio have ZERO symptoms
The majority of fatal Polio infections occur in those whose tonsils have been removed.
Before the rollout of the Polio vaccine in 1955, paralytic poliomyelitis was a low incidence disease. (about 1 in 22,000 or .005% of the US population and only 1 in 190,000 of children at normal risk contracted permanent paralysis or died)
The Polio vaccine does NOT prevent asymptomatic infection or transmission.
The Institute of Medicine has not ruled out that IPV vaccination can cause GBS or SIDS.
1 in 829 children may have seizures with the IPV vaccine.
A study shows a 38 times increased risk of permanent injury from the IPV vaccine vs Polio infection.
The Polio vaccine has not been proven to be safer than Polio infection for normal-risk children. Source
Recently, I postedand article and a video of Dr. Aseem Malhotra stating the following:
“You need to understand that the current system is encouraging good people to do bad things. And the root of this problem are big, very powerful corporations that have too much influence on government, on health care, on media, and their primary responsibility is to produce profit for their shareholders, not to give you the best treatment….these corporations, unfortunately, and the way that they go about their business, by misleading people, by their business model being fraud, they act like psychopaths, and they are a psychopathic entity….the conclusion is that we have a psychopathic entity influencing health policy, and that needs to stop and it needs to stop now. ~ Dr. Aseem Malhotra
The Polio Scam Makes a Comeback to Scare More Parents into Vaccinating Their Children – Vaccines NEVER Eradicated Polio: Vaccines CAUSE Polio
by Brian Shilhavy
Editor, Health Impact News
More and more people in the general public are waking up to the fact that the entire rationale used to vaccinate people is based on dogma, and not science, as many are now questioning those who control the vaccine agenda worldwide for perhaps the first time, with the result of many people choosing to not participate in this religious-like cult anymore.
This can currently be seen by the very low number of parents choosing to give the deadly COVID-19 “vaccines” to their young children. For example, in an article published in the Philadelphia Inquirer a few weeks ago, they reported:
Only 4% of children under 5 in Pennsylvania have received a dose of the COVID-19 vaccine.
The Globalists have already publicly published their plans for the next big “plandemic” which is currently in operation now and revolves around the “monkeypox outbreak” among gay men.
But within the past couple of weeks the corporate media has ramped up another scare tactic that seems to be targeted at children, by stating that polio is making a comeback, based on alleged detections of the “polio virus” in sewage and water treatment systems.
Children ages 1-9 in London were made eligible for booster doses of a polio vaccine Wednesday after British health authorities reported finding evidence the virus has spread in multiple areas of the city but found no cases of the paralytic disease in people.
Britain’s Health Security Agency said it detected viruses derived from the oral polio vaccine in the sewage water of eight London boroughs. The agency’s analysis of the virus samples suggested “transmission has gone beyond a close network of a few individuals.”
The agency said it had not located anyone infected with the virus and that the risk to the wider population was low. The decision to offer young children boosters was a precaution, it said.
“This will ensure a high level of protection from paralysis and help reduce further spread,” the agency said. (Source.)
But here’s the truth that is either not mentioned or buried in the details of the reports: these alleged “polio viruses” originate from individuals, mostly children, who have been vaccinated with the “live” oral polio vaccine (OPV), which has been banned for decades now in the wealthier nations because it is a well-known fact that these vaccines “shed” causing the infectious agent to pass through stools and urine and infect sewage and water treatment systems.
Rather than ban these highly toxic and dangerous vaccines, however, they have been continued to be distributed to poorer countries in Africa and Asia (particularly Afghanistan and Pakistan in recent years.)
The history of the polio vaccine and the corruption behind it is a topic we have covered for over a decade now on Health Impact News. We have been attacked and censored on this topic, as we have made the claims that based on the evidence:
the polio vaccine never eradicated “polio” as they simply renamed the symptoms associated with “polio” to make it look like polio disappeared, and
the only people being infected with a “polio virus” today are those who were vaccinated for it with the live, oral polio vaccine.
This was called a “conspiracy theory” for years by the corporate media, but the truth became so obvious that in 2019, just a few months before the “COVID Pandemic” arrived, the corporate media finally admitted that the only cases of polio worldwide were caused by the polio vaccine. NPR even did an entire show on it. See:
Just as there has been throughout the COVID-19 scam, honest doctors came forward over the years to expose the corruption in the polio vaccination campaigns, stating clearly that the polio vaccines were the problem, not the solution, but they were censored and even silenced.
Dr. Nicholas Gonzalez, M.D., was one of those critics, and we republished an article he wrote back in 2015:
I think, in the current debate, it would be a most useful exercise to go back in time, to review historical examples of allegedly or presumably catastrophic infectious disease, specifically two examples, that of polio and Keshan’s disease, for which in both cases a vaccine was thought to be the only solution.
I remember the hysteria generated in the media by polio, the well-funded advertising campaigns by organizations such as the March of Dimes, relying on, of course, emotional arguments to raise money from “regular” moms and dads and Girl Scout and Boy Scout troops all over the country.
My childhood vision of polio was that of a true catastrophe, threatening the entire population of the United States, with our only hope the dedication and hard work of our wonderful research scientists who were extolled in the press on a near daily basis.
As a fledgling research immunologist under Dr. Good somewhat fascinated by DuBos’ perspective, I began to investigate the actual epidemiology and ecology of polio. As I was to learn it turned out that polio “epidemics” as they were called, didn’t really emerge until the late 19th, and early 20th century.
I had been taught in medical school that the epidemic nature of polio showed itself because of growing population density in urban areas associated with poor sanitation. Though this position seemed logical, since polio transmits through a fecal oral route, the opposite has proven to be the case.
Studies from the late 1940s, before the availability of the Salk vaccine, indicated that in low-income urban areas up to 90% of the population showed antibodies to polio, though most who tested positive had no recollection of having been infected and had not experienced any residual neuro-muscular problems. For them, the disease seemed no more serious than a brief upper respiratory infection or gastroenteritis.
I think myself so fortunate that I contracted, and endured, the usual childhood illnesses, including measles, mumps, and chicken pox, even a minor brush with Epstein Barr. For me, and for all my school friends, these diseases were hardly anything worth remembering particularly, leaving us somewhat disabled for a few days, with much-appreciated time off from school and a certain amount of parental pampering.
No one I knew was left with encephalomyelopathy, nor any other serious neurological deficit as a result of their experiences with any of these viruses. I do believe these illnesses served me a valuable function, testing my immune system, letting it flex its muscles, teaching it how to work against a mild infection so that someday it might effectively deal with a more serious organism.
I see so many patients in their 20s and 30s, the first of the highly-vaccinated generation, coming to my office unable to function, having been exposed to some viral illness like Epstein-Barr, or Borrelia, or some associated “coinfection,” who five and ten and fifteen years later despite aggressive treatments of all types, both alternative and conventional, are unable to function, finish school, hold a job, at times – and you all know patients like this – unable to leave their room (except initially to see me).
These are young adults with immature immune systems, whose immune cells either underperform, don’t perform at all, or that over-react, with immune regulation gone haywire. We can get these patients well, fortunately, but they often endured quite a bit a suffering for long periods of time.
And these aren’t the kids with autism, these are young people with promising futures and careers ahead, sidelined and sidetracked by some trivial little virus.
When we think about the child paralyzed by polio or the poor debilitated diphtheria-infected Asian children, we need to step back for a moment, and realize Nature really isn’t the enemy, it’s so often – as Dubos made clear 50 years ago – what we do as individuals, as cultures, and as governments that makes a tolerable, manageable problem into something worse, and this includes force-feeding vaccination.
When these discussions begin, just remember the negative blowback from those “improved” public health measures in urban areas, that made polio a much worse disease than it had been, and left in their wake death and disability.
Speaking scientifically, it appears that no polio vaccine was really needed any more than it was needed for Keshan’s. Instead, we should have let kids be kids, playing in the mud, letting their immune systems grow and mature as Nature intended, without interference by well-intentioned and completely misguided science. (Source.)
Shortly after writing this, Dr. Gonzalez died “suddenly” at the age of 67, from apparent “cardiac issues.”
Dr. Bernard Greenberg’s 1962 Congressional Testimony on Polio
In testimonies given at US Congressional Hearings in 1962, Dr. Bernard Greenberg, head of the Department of Biostatistics of the University of North Carolina School of Public Health, testified that not only did polio increase substantially (50 percent from 1957 to 1958 and 80 percent from 1958 to 1959) after the introduction of mass vaccination programs, but statistics were manipulated to give the impression of the effectiveness of the Salk vaccine. Dr. Greenberg gave the following reasons why it appeared that polio decreased after the vaccine was given:
* Redefinition of an epidemic: More cases were required to refer to polio as epidemic after the introduction of the Salk vaccine (from 20 per 100,000 to 35 per 100,000 per year) ·
* Redefinition of the disease: In order to qualify for classification as paralytic poliomyelitis, the patient had to exhibit paralytic symptoms for at least 60 days after the onset of the disease. Prior to 1954 the patient had to exhibit paralytic symptoms for only 24 hours. Laboratory confirmation and the presence of residual paralysis were not required. After 1954, residual paralysis was determined 10 to 20 days and again 50 to 70 days after the onset of the disease. “This change in definition meant that in 1955 we started reporting a new disease, namely, paralytic poliomyelitis with a longer lasting paralysis,” testified Dr. Greenberg. ·
* Mislabeling: After the introduction of the Salk vaccine, “Cocksackie virus and aseptic meningitis have been distinguished from paralytic poliomyelitis, whereas prior to 1954 large numbers of these cases undoubtedly were mislabeled as paralytic polio,” explained Dr. Greenberg.
Source: Intensive Immunization Programs, Hearings before the Committee on Interstate & Foreign Commerce, House of Representatives, 87th Congress, 2nd Session on H.R. 10541, Washington DC: US Government Printing Office, 1962; pp. 96-97
Doctors and Scientists Have Been Calling for an END to the Dangerous Oral Polio Vaccine Since at Least 2005
Doctors and researchers who understand the dangers and risks of the oral polio vaccine (OPV) have been calling for an end to this terrible vaccine for years now. An editorial appeared in the Oxford Journals Clinical Infectious Diseases periodical in 2005 titled, “When Can We Stop Using Oral Poliovirus Vaccine?”
It was written by Dr. Harry F. Hull of the Minnesota Department of Health, and Dr. Philip D. Minor of the Division of Virology, National Institute for Biological Standards and Control, in the United Kingdom. They requested that the oral polio vaccine be stopped:
Why must OPV vaccination be stopped? Vaccine-associated paralytic poliomyelitis was recognized shortly after the introduction of OPV, with cases occurring in both vaccines and their contacts.
The time is coming when the only cause of polio is likely to be the vaccine used to prevent it. Ample molecular data are now available to demonstrate that vaccine viruses can revert to full neurovirulence.
Outbreaks of polio in China, Egypt, Haiti, Madagascar, and the Philippines caused by circulating, neurovirulent vaccine-derived polioviruses (VDPVs) demonstrate that these revertent strains are fully transmissible and pose significant population risks. (Source.)
Again, in 2009, an editorial was published in the Oxford Journals Clinical Infectious Diseases periodical titled, “Time for a Worldwide Shift from Oral Polio Vaccine to Inactivated Polio Vaccine“, by Dr Aamir Shahzad of the Department of Structural Biology and Biomolecular Chemistry at the University of Vienna. He wrote:
OPV has lost its effectiveness in providing herd immunity. It seems that children are getting polio from OPV, and it also seems that OPV is proving to be ineffective in stopping polio transmission from another source. Therefore, the whole world—and especially developing countries—should shift from OPV to IPV. (Source.)
Polio Vaccine Pioneer Doctor Admits Polio Vaccine Caused Cancer
Dr. Maurice Hilleman was the developer of Merck’s vaccine program. He developed over three dozen vaccines, more than any other scientist in history. He was a member of the U.S. National Academy of Science, the Institute of Medicine, the American Academy of Arts and Sciences, and the American Philosophical Society.
He received a special lifetime achievement award from the World Health Organization. Hilleman was one of the early vaccine pioneers to warn about the possibility that simian viruses might contaminate vaccines. In the interview below he states: “vaccines have to be considered the bargain basement technology for the 20th century.”
In a censored interview with Dr. Maurice Hilleman that has been published on YouTube, Hilleman admits Merck’s responsibility in unleashing the SV40, a cancer-causing monkey virus, via their polio vaccine. He also reveals that they probably also spread the AIDS virus in the same manner.
(Let us know if this video disappears from YouTube. We have a backup copy.)
Transcript
Dr. Len Horowitz: Listen now to the voice of the world’s leading vaccine expert Dr Maurice Hilleman, Chief of the Merck Pharmaceutical Company’s vaccine division relay this problem he was having with imported monkeys. He best explains the origin of AIDS, but what you are about to hear was cut from any public disclosures.
Dr Maurice Hilleman: and I think that vaccines have to be considered the bargain basement technology for the 20th century.
Narrator: 50 years ago when Maurice Hilleman was a high school student in Miles City Montana, he hoped he might qualify as a management trainee for the local JC Penney’s store. Instead he went on to pioneer more breakthroughs in vaccine research and development than anyone in the history of American medicine. Among the discoveries he made at Merck, are vaccines for mumps, rubella and measles…
Dr Edward Shorter: Tell me how you found SV40 and the polio vaccine.
Dr Maurice Hilleman: Well, that was at Merck. Yeah, I came to Merck. And uh, I was going to develop vaccines. And we had wild viruses in those days. You remember the wild monkey kidney viruses and so forth? And I finally after 6 months gave up and said that you cannot develop vaccines with these damn monkeys, we’re finished and if I can’t do something I’m going to quit, I’m not going to try it. So I went down to see Bill Mann at the zoo in Washington, DC, and I told Bill Mann, I said “look, I got a problem and I don’t know what the hell to do.” Bill Mann is a real bright guy. I said that these lousy monkeys are picking it up while being stored in the airports in transit, loading, off loading. He said, very simply, you go ahead and get your monkeys out of West Africa and get the African Green, bring them into Madrid unload them there, there is no other traffic there for animals, fly them into Philadelphia and pick them up. Or fly them into New York and pick them up, right off the airplane. So we brought African Greens in and I didn’t know we were importing the AIDS virus at the time. [emphasis added]
Miscellaneous background voices:…(laughter)… it was you who introduced the AIDS virus into the country. Now we know! (laughter) This is the real story! (laughter) What Merck won’t do to develop a vaccine! (laughter)
Dr Maurice Hilleman: So what he did, he brought in, I mean we brought in those monkeys, I only had those and this was the solution because those monkeys didn’t have the wild viruses but we…
Dr Edward Shorter: Wait, why didn’t the greens have the wild viruses since they came from Africa?
Dr Maurice Hilleman: …because they weren’t, they weren’t, they weren’t being infected in these group holding things with all the other 40 different viruses…
Dr Edward Shorter: but they had the ones that they brought from the jungle though…
Dr Maurice Hilleman: …yeah, they had those, but those were relatively few what you do you have a gang housing you’re going to have an epidemic transmission of infection in a confined space. So anyway, the greens came in and now we have these and were taking our stocks to clean them up and god now I’m discovering new viruses. So, I said Judas Priest. Well I got an invitation from the Sister Kinney Foundation which was the opposing foundation when it was the live virus…
Dr Edward Shorter: Ah, right…
Dr Maurice Hilleman: Yeah, they had jumped on the Sabin’s band wagon and they had asked me to come down and give a talk at the Sister Kinney Foundation meeting and I saw it was an international meeting and god, what am I going to talk about? I know what I’m going to do, I’m going to talk about the detection of non detectable viruses as a topic.
Dr Albert Sabin …there were those who didn’t want a live virus vaccine… (unintelligible) …concentrated all its efforts on getting more and more people to use the killed virus vaccine, while they were supporting me for research on the live viruses.
Dr Maurice Hilleman: So now I got to have something (laughter), you know that going to attract attention. And gee, I thought that damn SV40, I mean that damn vaculating agent that we have, I’m just going to pick that particular one, that virus has got to be in vaccines, it’s got to be in the Sabin’s vaccines so I quick tested it (laughter) and sure enough it was in there.
Dr Edward Shorter: I’ll be damned
Dr Maurice Hilleman: … And so now…
Dr Edward Shorter: …so you just took stocks of Sabin’s vaccines off the shelf here at Merck…
Dr Maurice Hilleman: …yeah, well it had been made, it was made at Merck…
Dr Edward Shorter: You were making it for Sabin at this point?
Dr Maurice Hilleman: …Yeah, it was made before I came…
Dr Edward Shorter: yeah, but at this point Sabin is still just doing massive field trials…
Dr Maurice Hilleman: …uh huh
Dr Edward Shorter: okay,
Dr Maurice Hilleman: …in Russia and so forth. So I go down and I talked about the detection of non detectable viruses and told Albert, I said listen Albert you know you and I are good friends but I’m going to go down there and you’re going to get upset. I’m going to talk about the virus that it’s in your vaccine. You’re going to get rid of the virus, don’t worry about it, you’re going to get rid of it… but umm, so of course Albert was very upset…
Dr Edward Shorter: What did he say?
Dr Maurice Hilleman: …well he said basically, that this is just another obfuscation that’s going to upset vaccines. I said well you know, you’re absolutely right, but we have a new era here we have a new era of the detection and the important thing is to get rid of these viruses.
Dr Edward Shorter: Why would he call it an obfuscation if it was a virus that was contaminating the vaccine?
Dr Maurice Hilleman: …well there are 40 different viruses in these vaccines anyway that we were inactivating and uh,
Dr Edward Shorter: but you weren’t inactivating his though…
Dr Maurice Hilleman: …no that’s right, but yellow fever vaccine had leukemia virus in it and you know this was in the days of very crude science. So anyway I went down and talked to him and said well, why are you concerned about it? Well I said “I’ll tell you what, I have a feeling in my bones that this virus is different, I don’t know why to tell you this but I …(unintelligible) …I just think this virus will have some long term effects.” And he said what? And I said “cancer”. (laughter) I said Albert, you probably think I’m nuts, but I just have that feeling. Well in the meantime we had taken this virus and put it into monkeys and into hamsters. So we had this meeting and that was sort of the topic of the day and the jokes that were going around was that “gee, we would win the Olympics because the Russians would all be loaded down with tumors.” (laughter) This was where the vaccine was being tested, this was where… so, uhh, and it really destroyed the meeting and it was sort of the topic. Well anyway…
Dr Edward Shorter: Was this the physicians… (unintelligible) …meeting in New York?
Dr Maurice Hilleman …well no, this was at Sister Kinney…
Dr Edward Shorter: Sister Kinney, right…
Dr Maurice Hilleman: …and Del Becco (sp) got up and he foresaw problems with these kinds of agents.
Dr Edward Shorter: Why didn’t this get out into the press?
Dr Maurice Hilleman: …well, I guess it did I don’t remember. We had no press release on it. Obviously you don’t go out, this is a scientific affair within the scientific community…
Voice of news reporter: …an historic victory over a dread disease is dramatically unfolded at the U of Michigan. Here scientists usher in a new medical age with the monumental reports that prove that the Salk vaccine against crippling polio to be a sensational success. It’s a day of triumph for 40 year old Dr. Jonas E Salk developer of the vaccine. He arrives here with Basil O’Connor the head of the National Foundation for Infantile Paralysis that financed the tests. Hundreds of reporters and scientists gathered from all over the nation gathered for the momentous announcement….
Dr Albert Sabin: …it was too much of a show, it was too much Hollywood. There was too much exaggeration and the impression in 1957 that was, no in 1954 that was given was that the problem had been solved, polio had been conquered.
Dr Maurice Hilleman: …but, anyway we knew it was in our seed stock from making vaccines. That virus you see, is one in 10,000 particles is not an activated… (unintelligible) …it was good science at the time because that was what you did. You didn’t worry about these wild viruses.
Dr Edward Shorter: So you discovered, it wasn’t being inactivated in the Salk vaccine?
Dr Maurice Hilleman: …Right. So then the next thing you know is, 3, 4 weeks after that we found that there were tumors popping up on these hamsters.
Dr. Len Horowitz: Despite AIDS and Leukemia suddenly becoming pandemic from “wild viruses” Hilleman said, this was “good science” at that time.
Smoke, Mirrors, and the “Disappearance” of Polio – Dr. Suzanne Humphries, MD
The person who has perhaps done more to expose the fraud about polio than anyone else in modern times, however, is Dr. Suzanne Humphries.
In 2011, she started publishing a ton of information exposing the Polio Scam. See:
There is plenty of confusion on the topic of vaccination, especially amongst brainwashed doctors who trusted their medical schools. Then the unsuspecting, trusting public trusts them…because the medical establishment must know best, right? And doctors are nice people, trying to do a good thing.
True. I was once one of those brainwashed doctors who believed in the benevolence of the medical system and believed that all I learned was the best that modern times had to offer. It is blazingly clear to me now though, that much of what is taught in medical school is enormously limited.
I now see that most doctors are little more than blind slave-technicians who follow the dogma they were taught and were rewarded for repeating, even as the truth unfolds in front of them dictating otherwise.
Unbeknownst to most doctors, the polio-vaccine history involves a massive public health service makeover during an era when a live, deadly strain of poliovirus infected the Salk polio vaccines, and paralyzed hundreds of children and their contacts. These were the vaccines that were supposedly responsible for the decline in polio from 1955 to 1961!
But there is a more sinister reason for the “decline” in polio during those years; in 1955, a very creative re-definition of poliovirus infections was invented, to “cover” the fact that many cases of ”polio” paralysis had no poliovirus in their systems at all. While this protected the reputation of the Salk vaccine, it muddied the waters of history in a big way.
Even during the peak epidemics, unifactorial poliovirus infection, resulting in long-term paralysis, was a low-incidence disease that was falsely represented as a rampant and violent crippler by Basil O’Connor’s “March Of Dimes” advertising campaigns. At the same time as Basil O’Connor was pulling in 45 million dollars a year to fund the Salk vaccine development, scientists started to realize that other viruses like Coxsackie, echo and enteroviruses, could also cause polio.
They also discussed the fact that lead, arsenic, DDT, and other commonly-used neurotoxins, could identically mimic the lesions of polio. During the great epidemics in the United States, the pathology called polio was reversed by alternative medical doctors who attested to great success, using detoxification procedures available at the time – yet they were categorically ignored.
Now it is admitted in the medical literature that other viruses can cause polio, yet few people on the street have any idea.
Prior to 1954, the following undoubtedly hid behind the name “poliomyelitis”: Transverse Myelitis, viral or “aseptic” meningitis, Guillain-Barre Syndrome (GBS)- (what Franklin Delano Roosevelt had)[4], Chinese Paralytic syndrome, Chronic Fatigue Syndrome, epidemic cholera, cholera morbus, spinal meningitis, spinal apoplexy, inhibitory palsy, intermittent fever, famine fever, worm fever, bilious remittent fever, ergotism, post-polio syndrome, acute flaccid paralysis(AFP).
Included under the umbrella term “Acute Flaccid Paralysis” are Poliomyelitis, Transverse Myelitis, Guillain-Barré syndrome, enteroviral encephalopathy, traumatic neuritis, Reye’s syndrome etc.
Before you believe that polio has been eradicated, have a look at this graph of AFP and Polio.
When people ask me where all the children on iron lungs are, I would answer that they should ask Dr. Douglas Kerr from Johns Hopkins, who stated on pg. xv in the Forward to Donna Jackson Nakazawa’s book “The Autoimmune Epidemic”…
“Infants as young as five months old can get Transverse Myelitis, and some are left permanently paralyzed and dependent upon a ventilator to breathe… my colleagues at the Johns Hopkins Hospital and I hear about or treat hundreds of new cases every year.”
Does the public have any idea that there are hundreds of cases of something that would once have been called polio, and some of those children will be dependent on a modern version of the iron lung? No. Parents today think that the Salk vaccine eliminated any need for ventilators, because the pictures of all these children on iron lungs are no longer paraded in front of people in order to create fear. Besides which, today’s “iron lungs” don’t look like a prototype submarine. They are barely recognizable as today’s “ventilators.”
The polio vaccine had the fastest licensing in FDA history (prior to COVID!) It was approved for commercial production after only a two-hour deliberation amongst the Licensing Committee, in a pressured environment. These scientists witnessed a vaccine that was escorted to market, before academic and community doctors had a chance to read any published reports on the safety studies, and before the results of the big polio vaccine trial made it into any medical journal.
If these scientists had had more say, it is likely that the “Cutter” disaster and the “Wyeth problem,” both events that led to crippling or death of vaccine recipients just weeks following the hurried vaccine licensing – could have been averted.
“Previously it [the vaccine] had been distributed as an experimental product, not a licensed product…the committee was asked to come to a decision very quickly…there was discussion of the report that Dr Francis had given, but we were not in a position to discuss it very intensively because we had not seen the report prior to this morning and the report was distributed to us after the presentation…we were pressured in the sense that we were told that speed was essential, and when we came up toward the 5:00 time, some of us felt we would like to discuss this matter more. We were told that to discuss the matter further it would have to go into the following week, and we would have to go to Washington or Bethesda and most of the members were unwilling to do so. We were in effect pressured into an earlier decision than we ordinarily would have made. …It was part of the pressure of events, put it that way.[5]”
And that is only the beginning of the polio story, the likes of which currently serve as the foundation of modern belief in vaccination, even by those who may have doubts regarding current vaccine policy.
No vaccines are safe. Having “efficacy” means an antibody response is generated, not that they keep you from getting sick. There are many other ways to keep children healthy other than injecting them with disease matter, chemicals, animal DNA, animal proteins, detergents and surfactants that inflame and weaken the blood brain barrier, potentially causing inflammation and other problems.
Do you know how much doctors learn about vaccines in medical school? When we participate in pediatrics training, we learn that vaccines need to be given on schedule. We learn that smallpox and polio were eliminated by vaccines. We learn that there’s no need to know how to treat diphtheria, because we won’t see it again anyway. We are indoctrinated with the mantra that “vaccines are safe and effective” – neither of which is true.
Doctors today are given extensive training on how to talk to “hesitant” parents – how to frighten them by vastly inflating the risks during natural infection. They are trained on the necessity of twisting parents’ arms to conform, or fire them from their practices. Doctors are trained that NOTHING bad should be said about any vaccine, period.
Historically it has been commonplace, since the times of the deadly smallpox vaccines – to discourage or silence scholarly, thoughtful and cautious opposition to mass vaccination policies. This is politics, plain and simple, in the environment of cronyism and corporatism that has invaded the supposed health-care industry.
The opinions of learned anti-vaccinationist doctors are not permitted on CNN, Fox News, or in mainstream literature. Probably because if they were broadcast on such media outlets, the unsuspecting public would do an about-face. Instead, the publicity that mainstream media concedes, often involves a parent who is opposed to vaccination, after a child becomes vaccine-injured, matched up with a celebrity talking-head doctor. Dr. Stork had an all-out tantrum after JB Handley got some sense interjected (from the audience!) during Jenny McCarthy’s invite.
For now, let’s just ignore Dr. Sears’ utter delusion over the history of vaccination and the decline in infectious disease. Having JB Handley on the program with the audience clapping for him, without editing him, was an unusual event. The standard approach on commercial television is to pretend that there is no anti-vaccinationist doctor to match the celebrity doctor, or those of the Paul Offit genre.
Therefore, they can only invite and publicly defeat those whom they underestimate.
Cheers to JB for getting an edge in. This is simply how the game of vaccination has always been played; keep the opinions of thoughtful and informed doctors and scientists out of the way of the cameras and peer-reviewed journals, and only allow the anti-vaccine perspective limited representation.
If you have doubts on the safety and effectiveness of vaccination, please keep your curiosity up, since the lives of your children may depend on it. You will probably have much deprogramming to do, just like most of us had. Full article.
Dr. Humphries, along with Roman Bystrianyk, published a book called: Smoke, Mirrors, and the “Disappearance” of Polio.
She has made the chapter on polio available to the public for free, as a .pdf, and you can download it here. This is one of the best, if not THE best, presentations on the historical polio and polio vaccine scam.
She presented her research on polio in 2012 at the Association of Natural Health Conference. It is still on YouTube (we have it in this 2013 article), but the lighting is bad and it is over an hour long.
Brad Kaye edited it down to just 30 minutes and replaced most of the graphics on his YouTube channel, but because YouTube is now purging anything critical of vaccines from its platform, we have a copy on our Rumble and Bitchute channels as well.
There is one section in the longer version that I wish had been kept, and that is a major section on the wonders of breastfeeding, and how children who were breastfed as opposed to infant formula fed, did not get polio. So it is well worth your time to watch the longer version, and we have a copy on our Bitchute channel, as it is well worth watching!
Oh, and when people who believe polio was eliminated through vaccines tell you: “You don’t see any iron lungs around anymore, do you?” – you can tell them: “Yes, that’s true, because that was old technology. What has replaced iron lungs today are ventilators.”
Yes, the same ventilators that Congress and President Trump spent $BILLIONS on in 2020, many of which are still sitting in warehouses today unused. Yes, the same ventilators that hospitals today get huge financial kickbacks from the government every time they put a patient on it following “COVID-19 protocol”, and which few patients survive.
Those ventilators are what have replaced “iron lungs.”
This is a video you are absolutely going to love and learn much from if you have never seen it before.
It has all the ingredients to cook up a “virus” and full-blown “pandemic”: labeling a “virus,” huge controversies over being able to actually test for that virus and identify it, a huge outbreak near a laboratory that was apparently trying to weaponize the virus, silencing and discrediting doctors with opposing views, massive government spending on advertising to convince the public that this virus was going to wipe out humanity if people did not go out and get the vaccine they created for it, using celebrities to endorse it, and catastrophic injuries and deaths resulting from a rushed to market new experimental vaccine.
Sound familiar? The playbook doesn’t change much over the years.
Conclusion: Do NOT Get Any Polio Vaccines!
Child in Pakistan being given the oral polio vaccine at the border by force. Photo courtesy of Dawn.com.
There have never been any vaccines that have been proven to stop polio, and it is a well-known fact today that all cases of polio are from the polio vaccines.
Finding evidence of the “polio virus” in sewage systems of large international cities where people frequently fly into from countries where the OPV is still being used, has been happening pretty much every year for the past 2 decades or so.
So this is not new “news.”
Polio vaccines are the problem, NOT the solution.
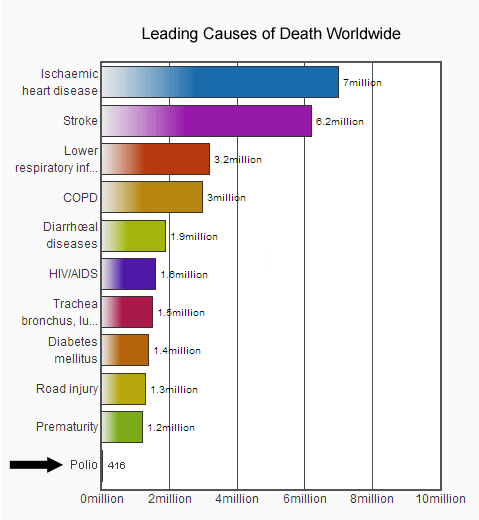
As to the polio “virus,” it is all hype and fear. Almost NOBODY is dying from polio worldwide.
This article is just a small sample of the coverage we have provided about the Polio Scam over the past 11 years. For further reading see:
Doctors who are critical of official positions on COVID policy are facing retaliation from their certification boards. The Association of American Physicians and Surgeons Education Foundation (AAPS) is suing three medical specialty boards for threatening doctors who speak publicly on these issues:
The American Board of Internal Medicine
The American Board of Obstetrics & Gynecology
The American Board of Family Medicine
AAPS has been around since 1943 and is an alternative to the American Medical Association. Its principles are to serve patients not the state, preserve medical freedom, and stand up for physicians.
We speak to AAPS lawyer Andy Schlafly.
_________________
**Comment**
The AMA and these other specialty boards need to go.Period. They are forcing doctors to follow a corrupt government’s dictates. This corrupt government has so many conflicts of interest it walks side ways.
Lyme literate doctors, including my own, continue to fight state medical boards due to the politicization of the disease. The COVID debacle has shown the world what has been going on in Lymeland for decades.
Please learn how the Federation of State Medical Boards (FSMB), a private tax-exempt 501(c) (6) trade association, is staffed with members who presently or previously held positions with other medical governing bodies and is in conjunction with the U.S. government which spawned the International Association of Medical Regulatory Authorities (IAMRA). FSMB’s president and CEO is also secretary of the IAMRA demonstrating the incestuous relationship and conflicts of interest.
In addition to contracting with the U.S. government and IAMRA, the FSMB (similarly to the CDC) runs its own foundation that functions as a separate 501(c)(3) organization but is supported by a “generous seed endowment” from the FSMB.
Conveniently, the FSMB foundation’s website does not disclose its donors.
Where does the FSMB derive its authority to regulate United States medical boards and, through its apparent international partner, the IAMRA, direct medical councils around the world to discipline doctors?”
Amélie Champagne, 22, died by suicide this month after a battle with Lyme disease, her father said.
Lyme disease can infiltrate the joints, heart, and nervous system if left untreated.
Her father shared the news on LinkedIn.
Amélie Champagne, 22, struggled to find an explanation for her physical pain for years before she was finally diagnosed with Lyme disease in June 2021.
By then, the tick-borne bacteria had already taken a severe toll on her brain. On a Sunday this September — more than a year after her diagnosis — Champagne died by suicide.
Her father Alain, outgoing president of the Canadian drugstore chain Jean Coutu Group, recently shared the news in a poignant LinkedIn post. (See link for article)
___________________
SUMMARY:
Like so many, it took years before this woman got diagnosed with Lyme disease.
And like so many, this complex disease(s) “hijacked her.”
If you or someone you know is experiencing depression or has had thoughts of harming themself or taking their own life, get help. In the US, call or text 988 to reach the Suicide & Crisis Lifeline, which provides 24/7, free, confidential support for people in distress, as well as best practices for professionals and resources to aid in prevention and crisis situations. Help is also available through the Crisis Text Line — just text “HOME” to 741741.
An analysis of U.S. Morbidity and Mortality Weekly Report (MMWR) data suggests the CDC has been filtering and re-designating cancer deaths as COVID deaths since April, 2021 to eliminate the cancer signal. The signal is being hidden by swapping the underlying cause of death with the main cause of death. And before it was manipulated, data from the Defense Medical Epidemiology Database (DMED) showed cancer rates in military personal and in their families TRIPLED after the shot rollout. Cancer patients have also gotten younger with the largest increase among 30-50 year olds, with dramatically larger, and multiple tumors, occurring in multiple organs as well as recurrence and metastasis increasing.
Since 1990, the number of adults under the age of 50 developing cancer has increased dramatically around the world.
What’s concerning is that the increase in early-onset cancers doesn’t seem to be slowing down – and improvements in screening alone don’t seem to be able to fully explain the trend.
“We found that this risk is increasing with each generation,” says one of the researchers, Shuji Ogino, a pathologist and epidemiologist at Brigham and Women’s Hospital in Boston.
(See link for article)
__________________
SUMMARY:
The researchers looked at 14 cancer types: breast, colorectal (CRC), endometrial, esophageal, extrahepatic bile duct, gallbladder, head and neck, kidney, liver, bone marrow, pancreas, prostate, stomach, and thyroid cancer – all of which are on the rise according to global cancer data.
Then they reviewed any available studies that could shed light on possible risk factors for these cancers by looking for clues in the literature describing any unique clinical and biological characteristics of tumors of early-onset cancers.
They found that early-onset cancer is an emerging global epidemic.
They found the following issues contributed to the uptick:
increased screening, however even countries that don’t have screening programs have increased cancer rates.
Diet
lifestyle
weight (obesity)
environmental exposures
microbiome
sedentary lifestyle
alcohol consumption
type 2 diabetes
Among the types of cancers studied 14 are related to the digestive system.
Regarding children, they are getting a lot less sleep than in the past.
While the article doesn’t mention it specifically, radiation from wireless devices such as cell phones which have become prominent today may be adding to this cancer surge as well. It is commonly known that EMFs wreak havoc in the body and many Lyme/MSIDS are particularly vulnerable.
Another little discussed topic is glyphosate, the major ingredient in Bayer-Monsanto’s Roundup which is the most widely used pesticide in the U.S. WHO and CA scientists both agree it is linked to cancer, yet the EPA concluded it was “safe” and “not likely” to cause cancer. The EPA has been forced to review this due to a federal judge finding the agency ignored human health studies, expert advice, and the agency’s guidelines for determining cancer risk. Source
And a 2021 study links lung cancer with mask usage.
Similarly to research regarding tick-borne illnesses, Alzheimer’s and cancer research have been controlled by a Cabal and researchers are currently accused of doctoring images, plagiarism, and faking data.
RENOWNED PHYSICIAN DOCUMENTS AGGRESSIVE CANCER POST COVID VACCINES
Belgian immunologist and medical research icon, Michel Goldman, had his values challenged when a Covid booster shot appeared to rapidly accelerate his cancer. He decided to go public with his story and tell the world.
Sept. 24, 2022
Excerpts:On September 22 of last year, Michel Goldman, a Belgian immunologist and one of Europe’s best-known champions of medical research, walked into a clinic near his house, rolled up his sleeve, and had a booster shot delivered to his arm.
Just a few weeks earlier, Michel, 67, had been to see his younger brother, Serge, the head of nuclear medicine at the hospital of the Université Libre de Bruxelles, where both men are professors. Michel was having night sweats, and he could feel swollen lymph nodes in his neck, so his brother brought him in for a full-body CT scan. When the images came through to Serge’s computer they revealed a smattering of inky spots, bunched near Michel’s left armpit and running up along his neck. It was cancer of the immune system—lymphoma.
Given his own area of expertise, Michel understood this meant he’d soon be immunocompromised by chemotherapy. With another winter on the way—and perhaps another wave of SARS-CoV-2 infections—that meant he had just a narrow window of opportunity in which his body would respond in full to COVID vaccination. Having received two doses of Pfizer the prior spring, Michel quickly went to get his third. If he was about to spend months absorbing poison as he tried to beat a deadly cancer, at least he’d have the most protection possible from the pandemic.
Within a few days, though, Michel was somehow feeling even worse. His night sweats got much more intense, and he found himself—quite out of character—taking afternoon naps. Most worryingly, his lymph nodes were even more swollen than before. He conferred with Serge again, and they set up another body scan for September 30, six days before Michel was scheduled to start his cancer treatment. Once again he sat in the radiology waiting room while his brother waited for the pictures to appear on his computer.
Serge’s bushy eyebrows furrowed when he spoke with Michel after having seen the scans. (“I will always remember his face, it was just incredible,” Michel told me.) The pictures showed a brand-new barrage of cancer lesions—so many spots that it looked like someone had set off fireworks inside Michel’s body. More than that, the lesions were now prominent on both sides of the body, with new clusters blooming in Michel’s right armpit in particular, and along the right side of his neck. (See link for article)
___________________
SUMMARY:
It is unusual to see such a swift progression in just 3 weeks
He hand his brother had a gnawing feeling the booster made him sicker
The article erroneously states this is a very rare life-threatening side effect. Doctors have been reporting this finding all over the world but are ignored.
An avid proponent of the shots, going to far as to reassure others about their safety, he’s definitely having a red pill experience.
Unfortunately he bought and propagated the lie that any chance of serious complications from the shots pale in comparison to the chance of complications from COVID.
Michael threw him into researching the mechanisms of action of the COVID shots and did find clues suggesting the the mRNA shots might be risky for a subset of the population as they are effective at generating a message and spurring its passage through helper T cells, which could give such a jolt to helper T cells that they go berserk. Overstimulation on those prone to forming tumors in those already with cancer, overstimulation could make it worse.
He learned that body scans of some of those who get vaccines, including cancer patients, haveshown heightened activity in the lymph nodes near the armpit on the side where the shot was received.
A mouse study also corroborated his experience.
Michael wrote a paper, about his experience titled “Rapid Progression of Angioimmunoblastic T Cell Lymphoma Following BNT162b2 mRNA Vaccine Booster Shot”
Worried his study would fuel vaccine skepticism he labored over every word, yet his paper follows earlier reports also suggesting a possible link between the COVID shot and lymphoma
Another doctor also worried that writing about five patients who had a relapse of kidney disease and eight patients who were newly diagnosed after getting the shot would also fuel vaccine skepticism.
Michael’s immunologist stated that the vaccine appeared to be related to the cancer’s behavior and then reneged by stating it’s just a case report – one patient.