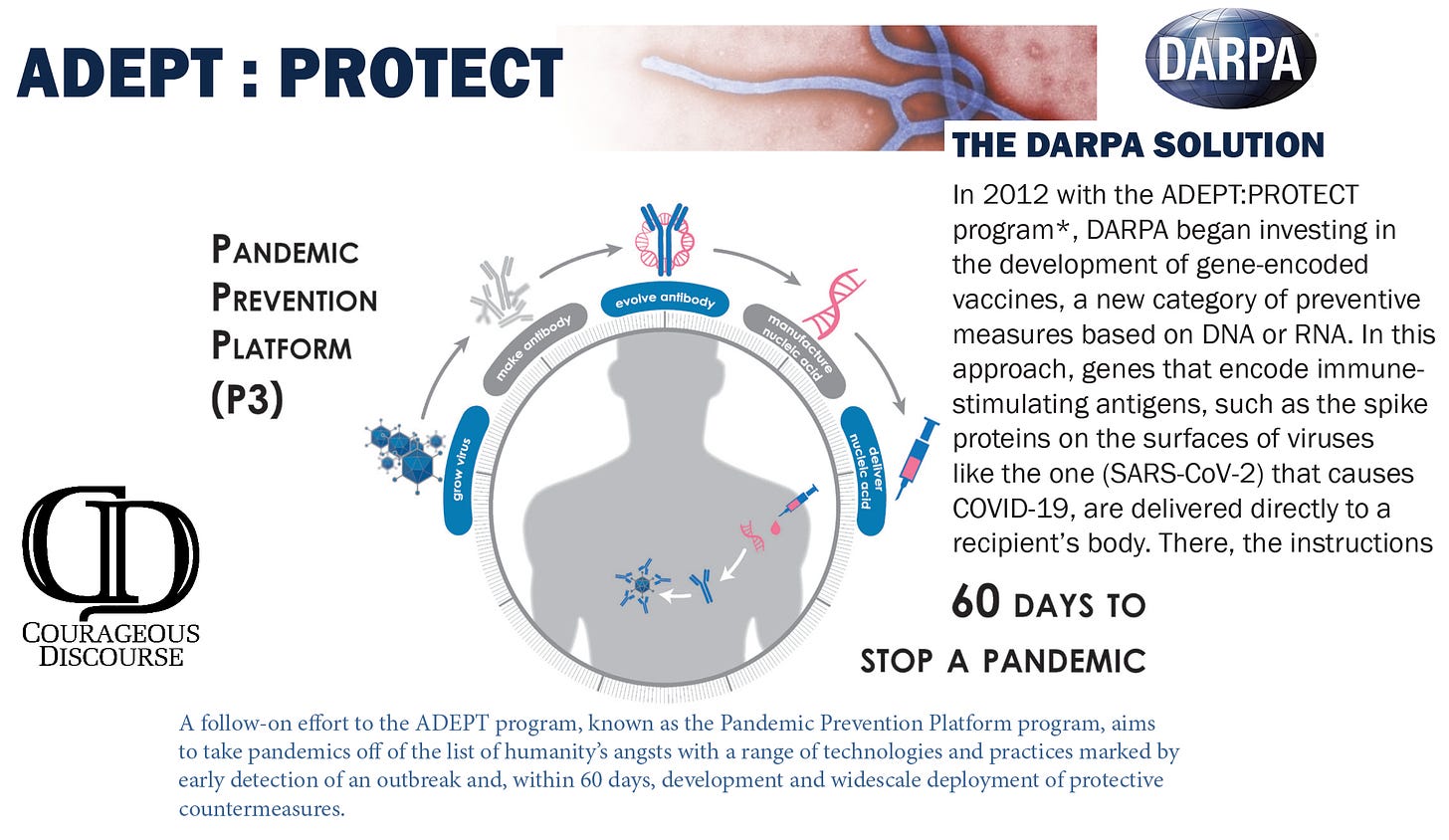
John Solomon on Real America’s Voice Just the News asked me why was mRNA chosen over traditional vaccines for the COVID-19 pandemic? My answer goes back many years to the US Department of Defense Biomedical Advanced Research and Development Authority (DARPA) ADEPT PROTECT P3 program which stated in 2012 the US will use mRNA vaccines to end pandemics in 60 days.
Former president Trump and the White House Task Force should have done their homework with a phone calls to DARPA and a few clicks on the internet and told America that mRNA was the plan for many years. It was not developed during the few months of Operation Warp Speed. (See link for article and 2 Min video)
_________________
Summary:
There are 9,613 patents licensed to giants in biotech and the US government
A retrospective cohort study found the US government invested at least $31.9bn to develop, produce, and purchase mRNA covid-19 vaccines, including sizable investments in the three decades before the pandemic through March 2022.
While the study claims “millions of lives were saved,” the truth is the experimental, COVID gene therapy injections saved ZERO lives.
Dr Jayne Donegan practiced as a Medical Doctor for 40 years. In 1990 she began her studies in homeopathy and naturopathy and is now a registered Homeopathic and Naturopathic Practitioner. She is a member of the British Society of Ecological Medicine and a patron of the College of Naturopathic Medicine. In July 2023, after applying unsuccessfully for four years, she was eventually deregistered from the General Medical Council. She is now free to continue working as a holistic practitioner without having to adhere to NHS policies that she believes were not in the best interests of her patients.
In 2011, Dr Donegan wrote a comprehensive article, Measles Outbreaks: The Song Remains the Same, for The Informed Parent.Christoph Plothe DO, Health and Science Lead for the World Council For Health, asked Dr Donegan to share her insights regarding recent measles scares on Better Way Today on 25 March 2024.
In the UK we are told that the recent measles scare is due to lower rates of vaccine uptake. These low rates are not surprising: during the Covid event doctors’ surgeries were closed, reducing access to these services. We also saw during Covid that making people afraid is one of the best ways to ensure compliance – so now the health authorities are trying to increase vaccination rates by threatening that children are going to die of measles. Dr Donegan denies that there is a measles emergency, but notes that – just like during Covid – nobody is informing the public about effective ways of managing measles or other diseases that result in fevers.
Were vaccines really the cure?
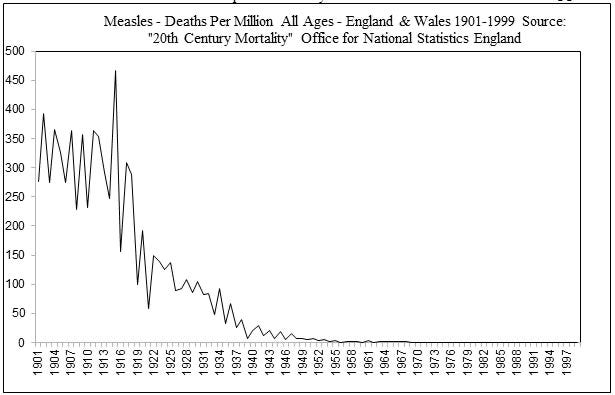
Dr Donegan points out that there is a lot more to immunity than antibodies generated by vaccines, and long before vaccines were developed, death rates from measles had been plummeting. This is not the story we have been told – or that doctors have been educated to believe. Instead we have learnt that the MMR vaccine is a lifesaving intervention that will protect us all from measles.
Measles deaths in England and Wales, 1940-1991. Source: Immunisation Against Infectious Diseases Handbook
In the Immunization Against Infectious Diseases Handbook, which provides guidance on vaccination to doctors, is a graph showing measles-related deaths in England and Wales. The graph starts in 1940, with the zigzag pattern reflecting the fact that measles epidemics normally occur about every two years. After introduction of the original measles vaccine in 1968 cases do appear to decline; and they continue to do so after introduction of the MMR vaccine.
Looking at this graph, it is clear why people believe that the measles vaccine was responsible for the decrease in measles-related deaths, but we need to look more deeply into the evidence. For instance, what the graph actually indicates is anassociation in time – not causality. Also, what is not stated is that, when the measles vaccine was first introduced, there was only a 30% uptake. Most parents didn’t see the point of the vaccine as measles was just a normal childhood disease, like chickenpox. Uptake of the vaccine only exceeded 50% in 1980, and it was only in the 1990s that uptake rates for all vaccines rose above 90%.
Dr Donegan herself had accepted without question graphs such as this in her medical textbooks. It was only once she started studying homeopathy and hearing that death rates had started to decline before the vaccines were introduced, that she started questioning her assumptions and researching the issue more deeply. Eventually, on an old CD-ROM from the Office for National Statistics (ONS), she found data that enabled her to produce a graph of measles mortality for the whole of the 20th Century.
Even before antibiotics became widely available, measles deaths were declining precipitously. By 1940 (the starting point of the graph in the medical textbook) – and certainly by the time the vaccine was introduced in 1968 – the number of deaths was almost negligible. Of course, sometimes people with underlying medical conditions, or those not properly treated (e.g. for fever) do die of measles and other infectious diseases. But they are the exceptions.
In developed regions, a great many diseases have declined not due to vaccines but due instead to the provision of clean water, removal and treatment of sewage, better nutrition, and improved indoor air quality. Indeed, in countries lacking these services, many children do still die of measles because these conditions undermine their general health and weaken their immune systems. Emeritus Professor Thomas McEwan, a past Chair of WHO’s Health Research Strategy Committee, stated that the radical decline in child mortality between the 1850s (approx. 1,000 per million) and 1960s (almost zero) in England and Wales was due not to physicians, but to surgeons and hygiene.
Making an informed decisions
As we know, governments use fear to pressurize parents to have their children vaccinated, even though graphs like the one above clearly show that the risk of death and the efficacy of vaccines have been exaggerated. Over the past 30 years it has become more difficult for parents to make the decision not to vaccinate their children but to allow them to contract a disease and develop strong, long-lasting natural antibody immunity. In the case of a future mother, natural immunity will also confer immunity onto her child for the first 18 months of life by means of transplacental antibodies! Insights such as these help parents make choices based on science rather than fear.
Something else that can help us decide whether or not to have ourselves or our children vaccinated is to research what is in the vaccines, and their adverse effects (which are generally highly underreported). In the UK, the Electronic Medicines Compendium provides access to information on drugs and vaccines used to treat various diseases. By typing into your search engine ‘EMC’ plus the name of a disease, you will find the patient information leaflet (PIL) and the summary of product characteristics (SmPC) for the relevant medication, for example MMRVAXPRO for measles.
Knowing how to manage a fever – which is what people did to protect their children before the measles vaccine was introduced – can also empower parents who would prefer not to vaccinate their children. This makes sense when you consider that the risks of a serious vaccine adverse effects may be underreported by a factor greater than 100, and that babies and young children are subjected to multiple vaccines and boosters, increasing their individual risks.
Unlike babies born to mothers who themselves had measles as children, and whose long-lasting immunity protects the infant until 18 months of age, vaccine-derivedantibodies are short-lived and not passed on from mother to baby. Prior to Covid, there was a measles scare in Europe; most of the children who died were actually babies below the age of 18 months born to MMR-vaccinated mothers.
It’s about more than antibodies
It is important to recognize that immunity depends upon more than antibodies, which (with the lymphocytes) are part of the adaptive immune system that protects against specific pathogens and changed body cells. The innate immune system is the body’s first line of defence operating at the skin and mucous membranes to protect against germs in general entering the body.
Something that few of us recognize is the importance of fever itself. In the 1950s, a General Practitioner, Dr Fry, reported that mothers were observing that their children did better after “a good dose of measles”. People at the time regarded diseases like measles and chickenpox as developmental steps. Ironically, going through these infections appropriately results in improvements, but avoiding them means that you miss out. Dr Donegan referred to an editorial in the British Medical Journal that stated that “autoimmunity is the price one pays for the eradication of infectious disease.” The author explained to Dr Donegan that the human immune system developed under the ‘insult’ of common childhood diseases; without having to deal with these challenges, the immune system doesn’t learn.
Dr Donegan feels that we should let children have their normal childhood diseases and manage them properly – and this means not bringing down all their fevers with paracetamol or ibuprofen. According to a WHO bulletin from 2000, “fever is an ancient adaptive response for which there are a few, if any, good reasons to suppress.” As long as the patient remains alert, can communicate clearly, and sleep peacefully, the fever should be allowed to run its course. Indeed, the rise in body temperature increases the rate of detoxification by the liver, filtration of blood by the kidneys, and the immune response. And while the patient must drink enough during a fever, the natural tendency not to eat is a logical response, as it allows the gut to prioritize production of immune cells rather than focus on digestion.
This article is a taste of a fascinating discussion. We hope you will visit the World Council for Health’s Video Library to watch the whole episode … including Health Coach Linda Rae’s short video on how to boost your immunity!
______________
**Comment**
The CDC obfuscates vaccine data is by classifying 95% of measles cases as ‘unvaccinated or unknown’– two fundamentally different categories. Truth be told, measles cases with unknown vaccination status may in fact be vaccinated.
The CDC purposely merges unknown cases with unvaccinated ones maximizing the association between measles cases and non-vaccination while obscuring uncertainty in the data. It purposely does not apply the same logic in reverse – merging ‘unknown cases with vaccinated cases maximizing the association between measles cases and vaccination, which very well could be true.
This allows them to smugly reinforce a predetermined narrative which the media regurgitates.
The MMR vaccine contains a live measles virus that was created through a laboratory process U.S. military biodefense experts state “could be considered, by current definitions, gain-of-function research.”
Peer-reviewed studies further document vaccine-strain replication and shedding, measles-like illness following vaccination, and frequent inability to distinguish vaccine-strain illness from wild measles in symptomatic cases.
Please share this information with those around you. We desperately need to return to sanity and wisdom. The past four years have attempted to change everything previously known about disease.
Go here to listen to doctor after doctor discussing the very real problems surrounding vaccinations. Vaccine information is being censored from nearly every platform. ‘Authorities’ simply don’t want you to know the following truths about vaccines:
They contain toxic ingredients
The CDC has been lying about vaccine injuries and deaths for decades
The vaccine given in trials are often not what is given to the public
Vaccines are used in lieu of a true placebo making them appear safer than they are
Trials often do not have a true control group
Infant deaths due to vaccines are NEVER listed on death certificates but are listed as SIDS due to a lack of ICD code
Vaccines can reactivate latent infections
Vaccines have contained retroviruses and other cancer and disease causing viruses
Corrupt ‘public health’ has never done a study comparing the vaccinated to the unvaccinated
Corrupt ‘public health’ has never done a study looking at the cumulative effect of vaccines – particularly looking at metal accumulation
Corrupt ‘public health’ never admits vaccines can cause the very disease they are supposed to cure
Doctors get kickbacks for pushing vaccines on their patients
According to Dr. Ehrenfeld’s bio that is posted on the AMA website, he has a distinguished career in anesthesiology. His bio also states:
Upon his inauguration, Dr. Ehrenfeld made AMA history as the first openly gay president of the organization. For the past two decades, he has been a nationally recognized advocate for lesbian, gay, bisexual, transgender and queer (LGBTQ+) individuals. In 2018, in recognition of his outstanding research contributions, he received the inaugural Sexual and Gender Minority Research Investigator Award from the director of the NIH.
I’m immediately struck by the combination of anesthesiologist and gay rights activist, as both endeavors have been matters of great controversy since the mid 19th century.
Imagine if—following Friedrich Sertürner’s discovery of morphine in 1805—medical boards in the United States (affiliated with the British East India Company) insisted that ONLY opioid-based analgesics could be used, and that no one could use ether to anesthetize patients. To understand just how much disagreement, discussion, and debate there was around the use of ether, take a look at this history of the Ether Controversy.
Imagine if a medical board in Boston established a censorship apparatus to prevent anyone from challenging the supremacy of morphine as an analgesic, so that William Morton, Crawford Long, and Oliver Wendell Holmes, Sr. couldn’t publish about the value of ether for surgical anesthesiology.
Fast forward to the end of the 20th century. Imagine if no one was allowed to publish any criticism of the promotion and marketing of OxyContin by Purdue Pharma. (See link for article)
Dr. Reiner Füllmich has continued to analyze evidence of the crimes against humanity from prison. that he and the Corona Committee had been working to expose since 2020. The corruption is being increasingly seen worldwide and “Their house of cards is collapsing” according to Reiner, “and we as international attorneys will do our best to speed up that process and make sure that Justice is done.” He adds ‘The windows of truth that are opening worldwide and the light that shines through these windows is in the process of identifying all of those who are responsible, no one will escape Justice.‘
Reiner Füllmich made this statement in a a break from the his trial due to the Easter holidays which has followed eight days in court. He has now been able to summarize the criminal proceedings against him and concludes that Hoffman and Antonia Fischer were only interested in ‘getting their hands on the Corona Committees donation. He claims that ‘through ‘fraud and extortion’, they had gotten their hands on roughly 1.5 million euros of his and his client’s money.’
Viviane Fischer, however, has confirmed in court that they both took loans in order to secure the Corona Committee’s donations which were at risk from “government attack, but they were both able to pay the monies back.
What this means is accusations that Reiner had embezzled committee funds are unfounded. In fact, there seems to be no reason for the man to have been kept in jail at all, and he believes, as many others do, that the criminal proceedings are an effort to shut him up and put him in jail and can see that the ‘DA’s case, is dead in the water.’
Reiner therefore, seems to be more positive for the future, which can be heard in his statement which you can listen to in full in the video of the audio below. However, I have also transcribed the audio recording verbatim and have added it underneath the video for those unable to play videos. (See link for article and 10 Min video)
WEF Planning to ‘Relaunch’ Covid Pandemic, Insider Warns
Hunter Fielding,
A bioweapons industry insider has blown the whistle to warn the public that the World Economic Forum (WEF) is planning to “relaunch” the Covid pandemic in order to finalize its “Great Reset” agenda.
According to Dr. Harvey Risch, a bioweapons expert and Yale University professor and epidemiologist, the “next pandemic” is about to erupt “seemingly out of nowhere.”
Risch warns that globalist elites are not finished with Covid yet, despite the appearance that the pandemic is “over.”
While the last pandemic may have failed to fully usher in the WEF’s “Great Reset,” another, more deadly Covid outbreak would surely complete the transition.
Both the “virus,” so-called, and the “vaccine,” so-called, were the perfect excuse for America’s bioweapons industry to boost itself as something the nation requires in order to serve the public good by protecting We the People against disease – or so it claims.
Dr. Risch is now alerting top trusted lawmakers in the hope of blocking the plans. (See link for article and video)
_______________
**Comment**
Risch is not alone. Seems it came stright from the horses mouth and Benzinga reported that WHO Director-General Tedros Ghebreyesus sounded the alarm that its a “matter of when not if” a new pandemic, infamously called ‘Disease X,’ will strike. This sounds similar to billionaire Bill Gates’s recent public concerns that “we’re making the same mistakes again” by failing to adequately prepare.
But researchers are preparing by using breakthroughs in artificial intelligence (AI) to further speed up future vaccine development against Disease X. The Coalition for Epidemic Preparedness Innovations is providing up to $4.98 million to the Houston Methodist Research Institute to use AI to do just that. They aim to use AI to analyze the structures of potential viruses that may be the eventual Disease X and then identify specific parts of their proteins that cause an immune response. For now, their efforts focus on viruses such as Nipah and Lassa, but their goal is to get the time to develop a vaccine against a pandemic down to just 100 days.
Gee, what could go wrong?
Meanwhile, Politico reported that a growing dependence on artificial intelligence could pose a danger to the U.S. financial system, and regulators need to rethink their siloed approach to rule-making to minimize the risk, Securities and Exchange Commission Chair Gary Gensler said.
I’m sure trusting AI to create a ‘vaccine’ in 100 days to be put in human bodies is much safer, right?
MIT immunoengineer Michal “Mikki” Tal remembers the exact moment she had an insight that would change the trajectory of her research, getting her hooked on studying a long-neglected disease that leaves millions of Americans suffering without treatment.
It was 2017, and she was a Stanford postdoc exploring connections between her immune regulation research and immuno-oncology, which harnesses the body’s immune system to combat cancer. Her work focused on how healthy cells broadcast “Don’t eat me” messages while cells that are cancerous or infected with a pathogen send self-sacrificing “Eat me” messages. Immune cells, in turn, receive these missives in pocket-like receptors. The receptor that receives the healthy cells’ signal, Tal read as she was poring over the literature that day, is the third most diverse protein in the human population, meaning that it varies a lot from one person to the next. It was a fact that struck her as “very odd.”
Tal, who has been obsessed with infectious disease since losing an uncle to HIV/AIDS and a cousin to meningococcal meningitis, wondered what this striking diversity could reveal about our immune response to infection. According to one hypothesis, the wide array of these receptors is the result of an evolutionary arms race between disease-causing microbes and the immune system. Think of the receptor as a lock, and the “Nothing to see here” message as a key. Pathogens might evolve to produce their own chemical mimics of this key, effectively hiding from the immune system in plain sight. In response, the human population has developed a wide range of locks to frustrate any given impostor key.
Wanting to test this hypothesis, Tal found herself walking the halls of Stanford, asking colleagues, “Who’s got a cool bug?” Someone gave her Borrelia burgdorferi, the bacterium that causes Lyme disease. Previous research from Tal’s collaborator Jenifer Coburn, a microbiologist now at the Medical College of Wisconsin, had established that Lyme bacteria sport a special protein crucial for establishing a lasting infection. Knock this protein out, and the immune system swiftly overwhelms the bugs. The big question, however, was what made this protein so essential. So Tal used what’s known as a high-affinity probe as bait—and caught the Borrelia’s mimic of our “Don’t eat me” signal binding to it. In other words, she confirmed that the bacteria’s sneaky protein was, as predicted, a close match for a healthy cell’s signal. (See link for article)
“Long covid looks exactly, and I mean exactly, like chronic Lyme.” ~ Michal “Mikki” Tal, MIT immunoengineer
_______________
**Comment**
Yet, despite knowing of this ‘sneaky protein’ that establishes a lasting infection, ‘the powers that be’ deny chronic/persistent illness with Lyme/MSIDS.
While the article factually states there’s no objective way to diagnose chronic Lyme and no medically ‘accepted’ therapy, it regurgitates the ‘same o, same o’ myth that only 10% suffer chronic symptoms.
It also correctly points out that short-term doxycycline, the widely ‘accepted’ treatment for Lyme, only prevents the bacteria from replicating which relies upon the immune system to kill off invaders which often doesn’t work due to the fact Lyme effectively gives patients immune system dysfunction – rendering it virtually useless. The article states that lengthy antibiotics can “ease” symptoms. I would disagree with this. For a subset of patients, it makes them completely well.
The author is far more into gender differences, which is the buzz word of the day, matters little, and won’t matter a tittle in helping patients get better. This ‘flavor of the day’ approach to research is the new norm and is unfortunately now required to get coveted government grants. All researchers know this little factoid, but the public remains in the dark.
Complaint aside, I did find the mouse experiment extremely interesting as it showed how Lyme ‘completely disfigured’ the uterus, which would explain why so many infected women have difficulties with pregnancies. Only ONE other study in the history of Lyme documented uterine infection.
This does show the extremely limited and biased approach to all things Lyme/MSIDS and it always amazes me that researchers literally have to stumble into this knowledge.
Blaming men is not the answer regarding the problems in research. The problem stems from conflicts of interestand corruption – with females just as culpable as males.
The article then switches gears into Long COVID, a contested term that has yet to be proven conclusively, yet accepted at face value by many. The first thing that crosses my mind when I hear that “Long COVID” and Lyme have identical symptoms is, who’s to say it isn’t Lyme?
the immune system remains in a faulty state – driving symptoms
Tal’s project uses AI which she hopes will allow her to predict who will go on to have persistent symptoms. She has already learned that current Lyme tests only look at IgG and IgM – not IgE, which she describes as an immune system ‘air strike’ and that those with this type of immune reaction have been ignored in research. She received $2 million to further test this hypothesis and she expects to publish findings as early as 2025.
And hold the press! – Tal states that at a conference the keynote speaker actually apologized for what he had written in the past about chronic Lyme after he got ‘Long COVID.’