
Patents Prove COVID Fraud & Illegal Dealings
https://articles.mercola.com/sites/articles/archive/2021/10/03/david-martin-covid-fraud.aspx
Patents Prove COVID Fraud and Illegal Dealings
October 03, 2021
Story at-a-glance
- In the early 2000s, David Martin, Ph.D., founder of M-CAM International, started finding large numbers of patents that violate biological and chemical weapons laws
- In 1999, Dr. Anthony Fauci funded research to create “an infectious replication-defective recombinant coronavirus.” In 2002, Ralph Baric, Ph.D. and colleagues at the University of North Carolina, Chapel Hill, filed a patent on recombinant coronavirus, and within a year, we got the world’s first SARS outbreak
- Since 1999, at least 4,000 patents involving coronavirus have been filed, including patents detailing key features of the so-called “novel” SARS-CoV-2 virus
- The 2001 anthrax attack, which came out of medical and defense research, led to the passage of the PREP Act, which removed liability for manufacturers of emergency medical countermeasures
- The funds for entitlement programs and pensions will dry up by 2028, at which point the drug industry will go bankrupt as well. With a burgeoning population that is sick from the COVID jabs, we need to prepare new systems to care for each other
In this interview, we continue our coverage of the COVID “plandemic” by speaking to David Martin, Ph.D., who has done a phenomenal job uncovering the paper trail behind the virus now known as SARS-CoV-2. As it turns out, this is not a novel virus at all, as patents and government grants detailing key features of the virus go back two decades.
Martin finished his doctorate at the University of Virginia in 1995, after which he was hired on to the medical school faculty in radiology and orthopedic surgery. In 2006, he set up the first medical device clinical trials organization for the University of Virginia — a company called IDEAmed — which conducted medical device clinical trials for U.S. Food and Drug Administration submission. So, he has an extensive background working with FDA clinical trials.
Monitoring Biological Weapons Violations
In 1998, he founded another company called M-CAM International, which is focused on finding ways to bring intellectual property into conventional finance. M-CAM also started auditing the U.S. patent system at the request of the U.S. Congress.
In the early 2000s, M-CAM worked with the Senate Banking Committee and was a contractor for the United States Treasury to expose white collar criminal activity around intellectual property and tax fraud. In doing that work, Martin also discovered something else.
“Quite alarmingly, we found an enormous number of patents [detailing] biological and chemical weapon violations,” Martin says. “That was not something we were looking for. I let people know this was not something we set out to find. This is something that landed in our lap.
I developed a technology a decade earlier called linguistic genomics, which is a means by which you can look at unstructured text data and find the metaphoric meaning inside of what is being communicated. As you can imagine, if people of ill intent are trying to do something, they often hide what they’re doing in plain sight, but they use language that is not conventional.
So, when you find a patent, for example, on a blast-resistant pathogen from a rocket-propelled grenade — did you hear what I just said? ‘A blast-resistant pathogen from a rocket-propelled grenade.’ Does that sound like it’s a common way to inoculate a population or does that sound like [a bioweapon]?
And so, finding a number of bioweapons patents, we started taking into account some very serious things. I published once a year the literal global phonebook of every biological and chemical weapon violation that took place anywhere in the world.
[It tells you] the who, the where, the who funded it, what their addresses are. It was … used by U.S. law enforcement, intelligence communities and elsewhere around the world to track things that were being done inappropriately. And, it was in 1999 [that] we started detecting that there seemed to be an alarming event around coronavirus, which we’re going to get into.”
Coronavirus Identified as a Potential Vaccine Vector
As explained by Martin, in 1999, the National Institutes of Allergy and Infectious Diseases (NIAID), headed by Dr. Anthony Fauci, identified coronavirus as a possible vaccine vector.
At the time, the disclosed rationale was to try to come up with an HIV vaccine, and to that end, Fauci, in 1999, funded research to create “an infectious replication-defective recombinant coronavirus.”
In 2002, Ralph Baric, Ph.D. and colleagues at the University of North Carolina, Chapel Hill, filed a patent on recombinant coronavirus, and within a year, we got the world’s first SARS outbreak.
The Real Tony Fauci
For more background on Fauci, be sure to read Robert F. Kennedy Jr.’s book “The Real Tony Fauci,” which details how Fauci’s promotion of AZT during the 1980s ended up killing hundreds of thousands of people. And the pattern we’re seeing with coronavirus is basically a repeat of previous behavior. Martin says:
“It’s important to realize that at the time [in 1984 when Fauci became director of the NIAID] we were transitioning from an STD environment in which syphilis and gonorrhea and those types of STDs were the things that we were concerned about …
HIV became a political and social hot potato because it was associated in many respects with lifestyle branding, and as a result it became a political issue to essentially identify a class of the population that could be the basis for research without consideration.
The notion by Fauci was that people with HIV had already made decisions that somehow entitled them to less humanity. As a result, the clinical trials around developing both management techniques as well as potential treatments … were done in a very reckless fashion. Numerous people died in [those] clinical trials, and by the way, still are …
He has been obsessed about this HIV situation as a platform to, essentially, use humans that he determines to be some form of sub-human for clinical trials. It is a horrific blight on the United States’ medical establishment that we have been willing to allow this to go on in the name of science, in the name of health promotion, since 1984, without any significant disruption or check.”
The First SARS Outbreak
The first SARS outbreak occurred in late 2002 going into 2003 in China. Curiously, before Baric’s team invented and patented a recombinant infectious replication-defective coronavirus, no one had ever heard of SARS.
“I’m not drawing a causal relationship,” Martin says. “I’m making an observation that humans and what we call coronavirus seem to have cohabitated this earth for hundreds of thousands of years.
And then we manipulate that [virus] in 1999. We start playing around with putting it into different animals and different human cell line models, and then in 2003, we have SARS. Like a lot of other things, it’s an observation worth noting.
What makes the observation more problematic, obviously, is this was happening during the unfortunate results of the 2001 anthrax attack, which as you know came out of federal labs …
[It] became very clear that this was not [due to] a bad actor, per se. This was medical and defense research gone bad that got into the public and people died. But the real benefit, if you will, of the anthrax attack was the passage of the PREP Act.”
Anthrax Attack Provided Desired Liability Removal
Inside the PREP Act we now have the carte blanche removal of liability for manufacturers of medical countermeasures. As noted by Martin, the PREP Act has “made pharmaceutical companies much more capable of instilling terror in the population, coercing a population into taking an untested measure, and doing so with absolute impunity.”
Curiously, while Martin’s annual report on bioweapons patents was, with only a few exceptions, appreciated and used by agencies around the world, when it comes to the information he has amassed on coronavirus, not a single agency anywhere in the world has been willing to address it.
“No one … seems to be willing to look at the fact that beginning in 2016 we started seeing very alarming language being used, which was ‘coronavirus poised for human emergence.’ This was in patents, but also in scientific publications. And when you start referring to a coronavirus allegedly poised for human emergence, after the World Health Organization has declared SARS eradicated, there’s something desperately wrong with that picture.”
Racketeering and Organized Crime
The biggest alarm bell was published February 12, 2016, by EcoHealth Alliance president Peter Daszak1 who, according to Martin, has been “the money laundering agent” for gain-of-function research coronaviruses after the U.S. implemented a moratorium on that kind of research in 2014. Rather than close it down, this research was simply moved over to China instead. In 2015, Daszak stated:2
“To sustain the funding base beyond the crisis, we need to increase the public understanding of the need for medical countermeasures, such as a pan influenza or a pan coronavirus vaccine. A key driver is the media and the economics will follow the hype. We need to use that hype to our advantage to get to the real issues. Investors will respond if they see profit at the end of the process.”
That statement was made by Daszak in 2015, and was published in the spring of 2016. The statement “set off alarm bells very loudly within my organization,” Martin says, “because when you have somebody who is promoting gain-of-function research, and clearly blurring the line on what is even legal … saying we need ‘media to create the hype’ … and ‘investors will follow if they see profit’ … that doesn’t sound like public health.
To me, that sounds like organized crime. That sounds like racketeering, and we need to raise this issue.”
What the Coronavirus Patents Show
In all, since 2002, some 4,000 patents have been filed on the genome, vaccines and detection of coronavirus. According to Martin, this is alarming, “because you don’t file patents on something that you don’t intend to commercialize.” Evidence of intended commercialization can also be found by looking at the dates of certain patents by certain companies.
April 28, 2003, the U.S. Centers for Disease Control and Prevention filed a patent on the genome of the SARS coronavirus. Five days later, Sequoia Pharmaceuticals received a $935,000 grant and filed U.S. Patent 7151163 for a treatment for that same virus. How can you file a patent for the treatment of a virus that was only discovered five days earlier?
“That sounds like an inside job,” Martin says. “Because you cannot have a pathogen identified and a cure for it in five days, when all of the information was held from the public, because when the CDC filed its patent on the genome of coronavirus, it paid to keep that patent secret.
So, somebody somewhere knows that this thing was going to turn out to be a moneymaker … The proliferation of proprietary controls around SARS Coronavirus probably exceeds at least by two or three times most other pathogens …
Dana Farber had a monoclonal antibody patent system that came out of three NIH grants. Their patent 7750123 on the monoclonal antibody for SARS-Cov treatment took place in 2003.”
So, while we’ve been told that SARS-CoV-2 is something we’ve never seen before, there are 4,000 patents and patent applications that say otherwise. The same can be said for the testing and the COVID shots. For example, Pfizer filed the first S1 spike protein vaccine patent on coronavirus in 1990 — 30 years ago.
“Regardless of what part of the story we look at, the patent record is full of thousands of patents where commercial interests funded by NIAID and the National Institutes of Health have been building the economic cabal around coronavirus. This is not a new thing. It hasn’t been a new thing.
And regrettably, we’re being told continuously that somehow or another there’s something novel about this experience, despite the fact that every single part of what we are told is being detected with PCR … the injections, every single one of those things has been known and isolated for over 30 years.”
How Did We Get Here?
How did we get to a point where taxpayers are funding research on pathogens that are being designed to sicken and kill us, only to drive profits into the drug industry and all these various patent holders, which include the government itself?
In large part, it goes back to the implementation of the Bayh-Dole Act of 1980, which allows the beneficiaries of federal grants to file patents on work derived from federally funded research. The idea was that the economy would benefit by allowing scientists to be entrepreneurs first, rather than simply publishing their research.
This piece of legislation has undermined health care by bringing the patent office, the FDA and CDC into an unholy trinity that serves and promotes private pharmaceutical concerns. So, what we have now is an insidious funding loop. Martin explains:
“Corporations and pharma lobby to get people elected. Once they’re elected, the lobbyists flow an enormous amount of money into the various NIH programs. In the case of NIAID, since Fauci took over [in 1984], $191 billion have gone through his fingers. Now, is that because he’s successful?
No, as a matter of fact, under his watch, allergies and infectious diseases have increased over 60 times. Yet somehow or another, he’s still the director of a failed [agency] that’s gotten $191 billion to solve a problem that is getting worse every single year.
If it was a company, we would have fired him. The problem is, it’s not a company. It’s a money laundering agency. It moves public funds through the hands of a federal agency into the research laboratories, which ultimately are going to conduct research that is then licensed back to the benefactors, which are the pharmaceutical companies that paid to get people into office in the first place.
So, this is a revolving door problem, and the Bayh-Dole Act created an insidious incentive that said that the only research that was going to be conducted was going to be research that ultimately would flow back to the pharmaceutical industry and create juggernauts, where the risk of R&D was taken by the public and the benefit for that R&D was taken by the private. That’s a horrible thing, and that is exactly what Fauci has run.”
Why Did Fauci Pick Moderna as Vaccine Frontrunner?
Martin also points out that Fauci has also lied to Congress about the NIAID’s financial interests in drugs. During this pandemic, Congress and the Congressional Budget Office asked for an accounting of NIH-owned patents where they have potential commercial interest in the drugs being produced. Fauci did not disclose any of them. Instead he lied and said there are none.
“The evidence is stacked a mile long,” Martin says. “Moderna stands alone as the only recipient of NIAID funding that fails to comply with the law and fails to disclose the federal government’s interest in their intellectual property.
Despite the fact that everyone knew Moderna failed to disclose the federal government’s interest in its research, Fauci picked Moderna to be the frontrunner for an untested, commercially unsuccessful and entirely unproven mRNA vaccine technology in the spring of 2020.
There was no rational justification for that, and there would have been less rational justification, given the fact that Moderna is on record as having violated the federal law, the Bayh-Dole Act, 141 times at the time they were picked to be the winner.
This is a known fact, but it was overlooked entirely, and not a single law enforcement agent anywhere in the United States has decided that having a criminal organization supply a product sounds like a bad idea.”
Violations of Law Everywhere
Since the beginning of this pandemic, the number of rules, laws and regulations that have been broken in the name of public health boggle the mind. Even laws that are absolutely clear and in no way ambiguous are being broken. For example, under Code of Federal Regulations Title 21, section 50, no one can be forced or coerced into a clinical trial of an experimental medical product, even if it’s a pandemic countermeasure.
“It’s black and white, and this clinical trial does not end until 2023 in the first best instance. So, there is no such thing as an approved or even authorized use of a [COVID ‘vaccine’] that can be compelled on the population,” Martin says.
And yet they’re bribing, threatening and coercing people everywhere. The drug companies also violated basic principles by eliminating all of the controls and giving the test vaccine to everyone in the trials, leaving us nothing against which to compare side effects. They also do not have an independent investigational review board, or the statutorily required approval processes for the protocol.
The companies themselves decided to modify their protocols midstream, which simply isn’t how it’s done. Basically, we do not have an actual clinical trial on these COVID shots, because so many of the basic principles of clinical medical research were violated.
Collapsed Judicial System Has Put Big Pharma in Charge
The federal government is also violating the False Claims Act by telling you the COVID shots are safe and effective, when the studies are still years from being completed, and have been undermined in all the ways just mentioned.
“What we have is a situation where the deaths are actually considered to be acceptable,” Martin says. “I don’t know what world you have to come from to find that term even remotely speakable. I think the utterance of that phrase is horrific … We are killing people willfully, and we are doing it with impunity in the name of what we call a love affair with science.
The only problem is we’ve desecrated science in the process because it turns out that when I did randomized double-blind, placebo-controlled trials, you know what I had to do? I had to keep the populations blinded. I had to keep it placebo-controlled for the whole clinical trial. And the reason I had to do that is because that’s what the statute requires.
This entire process has been willful acts of harm to humanity. And the only hope we have is a very small note in the Department of Justice opinion that took place under the Trump administration, which says that if this was based on felony acts, then the entire emergency use authorization and all its benefits would collapse.
In other words, if we can show that a felony has occurred — racketeering, lying to Congress, the public coercion … [and] in the Fauci dossier3 I outline dozens of felony violations — [it] would bring this entire thing to its knees, because the moment the PREP Act protection falls away from Pfizer, Moderna, Johnson & Johnson, AstraZeneca and others, I can guarantee you [Fauci] will not be promoting a vaccine.
If they are liable for a single injury or death, they’ll pull the plug on what they know to be unsafe. That requires law enforcement to do its job. And somewhere there has to be a prosecutor who’s willing to do their job … Right now, I genuinely do not think we have three tiers of government. I don’t think there is a Department of Justice.
The judiciary is functionally gone … When we allow the judiciary to be an arm of the executive [branch], then what happens is we’ve actually lost the three-tiered structure of government. And, as a result, the system collapses. The judiciary was the only thing that was explicitly independent. We don’t allow judges to get sponsorship in campaign finance. We don’t allow judges to be elected.
We appoint them, we go through an approval process. We do all sorts of things to try to make sure the judiciary is independent. So, the only risk to the pharmaceutical industry, the only risk to an executive out of control, was the judiciary.
By collapsing the judicial system in the United States, we have effectively made the government a servant of its benefactors — and that is the pharmaceutical industry.”
How Will It End?
With what appears to be a near-total collapse of the judicial system, it looks like we’re on a straight path to global tyranny, with no routes of escape. Martin, however, believes there may be a way out, but it will require action on behalf of rational individuals blessed with foresight. He explains:
“You have to have currency to buy off politicians. Back in 2008, when we had the global financial crisis… we instituted a policy that [will] functionally bankrupt our entitlement program (Social Security, Medicare and Medicaid) in 2028 [or 2033] …
The best math we have is that the annuities and pension programs of the United States functionally run out of their trust fund in 2028. What does that mean? Well, one of the things that people overlook is there’s an unholy alliance between the insurance companies and what we call health care.
Insurance companies are long-dated asset holders. These are the people who have to have money today to cover issues in the future. That’s what a long-dated asset holder is. The problem is that the Federal Reserve and the European Central Bank and other central banks have suppressed the value of the return on funds, so the funds are running out of money faster than expected …
You know as well as anybody else that for a politician to stand up and say, ‘I’m going to abolish or significantly alter Social Security’ is the death knell to any political aspiration. Tiny problem. But whether they say it or not, the trust fund runs out of money in 2028.
Now, here comes the kicker: So does the pharmaceutical industry because it turns out that the money that’s going into that system is actually paying for the drug dependency of this country.
And if we go all the way back to 1604 — to the establishment of the British East India Company and the establishment of the Virginia Company — we’ll realize that the 400-plus-year tradition that we have, where we have built nation states on the back of the drug trade, is coming to its end.
The good news for all of us is it’s going to end around 2028, because we have a convergence that they didn’t figure out how to cover up. The convergence is that the people with the money, the big pharmaceutical players, are the beneficiaries of a system that is going to bankrupt itself by virtue of their actions.
This is the brontosaurus that ate too much because it was the biggest dinosaur. And the great news is they have the brain the size of a pea, just like the brontosaurus. They are not smart. And the best thing we have going for us furry humans is that we actually are nimble.
Now, does that mean that we are not going to have an ounce of pain through the process? Absolutely not. There is social disruption that we can’t even imagine on the horizon in 2026, 2027 and 2028, because 86 million people will lose what they thought was going to be their retirement funds.
When we see that number now go to 100 million people, and the 100 million people are sicker because of what we’ve injected today … those people who are going to require greater health care then are going to be faced with a bankrupt system incapable of supporting their life and their livelihood. And that is the death knell of this story.
The best news about this is we have time if people of good conscience get together and say, ‘We’re not going to let that apocalypse arrive because we have time to start building communities that actually care for each other. We have time to start building accountability structures.
We have time to start doing things that bring our social fabric together so that when that system collapses, we can come back to a rational view of what life and liberty and the pursuit of happiness is’ because, until we can reclaim the sovereignty of our health, we cannot celebrate the sovereignty of our life.”
What About the 2030 Agenda?
By now, you’ve probably heard of the World Economic Forum’s Great Reset agenda, which includes the transition to a Central Bank Digital Currency. With that, they can abolish the dollar and “reset” the entire global economy that is now tottering on its last leg. However, even here there may be kink in the plan that can save us.
“Like a good [James] Bond villain, he’s actually ignorant of history,” Martin says. The reason Martin remains optimistic that the Great Reset doesn’t have a chance at all to succeed is because there’s no way the global public will embrace an all-digital system that can be annihilated by an electromagnetic pulse or electromagnetic disruption.
This year alone, we’ve seen internet failures, power outages and digital finance hacks that would leave people stranded without a single penny were they reliant on an all-digital financial system.
“The digital currency illusion is the most bizarre and pathetic Dr. Evil plan anybody’s ever concocted,” Martin says. “The fact of the matter is the digital currency craze is one of those fantastical illusions that unfortunately has a single-point failure.
We live in a world where actors of both anarchist intent, and very, very laudable privateers and pirates are more than happy to make sure that digital currency never sees the light of day because they will, in fact, hack, crack and disrupt every system out there.
And so, I look at the whole Great Reset as great theater … But the entire illusion is being run because they’re out of ideas. And … when the incumbency is out of bad ideas, they try desperately to force you into a behavior that you would not otherwise accept. All you have to do is just say no. Just don’t play along.”
The Financial Incentive for Depopulation
Is it possible that the COVID jabs might cause premature death and be an intentional form of depopulation? Well, since we’re following the money, there’s certainly a financial incentive for such a scenario. As noted by Martin, if you’ve made financial promises to people who are closing in on retirement, the fewer there are of them the better.
“The financial interest for depopulation is a thoroughly compelling argument,” Martin says. He recently reviewed this argument in a lecture given at the Church of Glad Tidings in Yuba City, which you can view above.
In short, having people live long enough to tap into their Social Security benefits and live to the full maturity of their life insurance policies is problematic with respect to the financial collapse that is looming.
Based on these financial realities — which certainly are not advertised or publicly discussed — there’s clearly an economic incentive to shrink the population and get rid of as many people as possible before 2028. Unfortunately, based on previous lipid nanoparticle and mRNA trials, the chance of a mass casualty event is high.
“There is no question … they jumped over animal trials for a very important reason,” Martin says. “We’ve been told it was to save time, but it wasn’t to save time.
It was to put this particular pathogen into humanity, so that a lot of people suffer and ultimately die of effects that we could have picked up if we had done it the traditional way, which is seven to eight years of safety studies, before we decide to put it in the arms of humans.
That’s not what we did. And if we look at the safety data from animal studies on mRNA, and on the lipid nanoparticle, there is no question that there is going to be a fatality increase because of this …
But the concern I have, [which may be] more egregious [than] the death … is the malingering morbidity, people who will require around the clock medical care is going to be a drain that will infect our economy so deeply that we may not recover.
Because if we have people who have to stay at home with children who are sick, if we have people who have to care for elderly parents who are sick, if we have people who are caring for a spouse or a family member who are sick, that means we do not have the ability to enjoy life and liberty. And the fact is that I think we’re going to have a bigger morbidity than mortality event.”
Now, as if all of that weren’t enough, Martin has also discovered CRISPR patents that describe how they can “clip” the effects of mRNA/DNA-based vaccines from people. He believes they may be building a pathogen set that is then introduced into the population so that they can later introduce a more expensive technology that can fix what was broken. This, unfortunately, could mean survival may be based on your ability to pay.
Were There Excess Deaths Due to COVID-19?
To backtrack for a moment, while we’ve been told COVID-19 caused excess deaths in 2020, one way to double-check that is to look at the number of life insurance policies paid. And in 2020, there were actually fewer life insurance policies paid out than normal, according to Martin.
“Whose numbers are you going to believe? Are you going to believe the CDC who’s trying to pump and dump this terror campaign of people dying, and therefore you need to have your mask on, you need to socially distance, you need to vaccinate?
Or are you going to believe the numbers from the people who actually pay claims when real human life ends? It turns out that if you look at the audited financial statements of the world’s largest life insurance companies, we can find no excess death evidence. Is COVID so smart that it only kills the uninsured? Is that what we’re supposed to believe?”
Live Consciously, Aligned With Health
In closing, I, like Martin, believe we can survive this and keep our freedom. But we must act. Individually, every single person needs to take actions that are in line with pro-life and liberty morals and ethics. As suggested by Martin, spend your money on certified organic foods and locally grown foods to help build a healthier food system.
Spend time with friends and family and share information. Start building a sense of community again, in whatever way makes sense to you. When you make a purchasing decision, analyze whether you’re supporting the evil being perpetrated, or choking its money supply. We need to start building micro-economies that can later grow into alternative economies. We need to start building support structures for when the financial and health care systems break.
“The fact is we are in a very unique moment in human history, and it probably is as close to the story of Joseph in Egypt as you can get. You know the seven fat years and then the seven skinny years? Well, guess what? We have a couple of fat years left. You know what we should be doing?
We should be investing in our networks of relationship. We should be investing in our networks of community. We should be building those resilient fibers that hold us together because we know that there is a famine coming. And we are in a unique position right now to actually do something about it.
So, start with yourself. Make sure that what you put into your body is aligned to your health. Make sure that what you do with your body is aligned to your health. And then as you do that, invite other people into living a life that in fact models that behavior, so that we start building communities of consciousness. And as we build those communities, we will start building currencies of consciousness …
There are a bunch of ways that we can solve these problems, and we can do it using the market. We can do it using our consciousness, but we need our consciousness, we need our community, and we need our currency to be organically aligned to humanity again.”
How to Break the Propaganda Cycle
Doing the things mentioned above will also further another task at hand, which is to break the propaganda cycle. The key, really, is to simply live your life as healthily and joyously as possible, so that people around you can see there are others out there who aren’t living in fear. Eventually, they’ll start seeing they actually have a choice.
“Listen, propaganda cannot stand against the truth of a life well lived,” Martin says. “It can never stand against that truth. What we’re trying to do is the wrong energy. We’re trying to confront irrationality with rationality. But what we need to be doing is being persistent in showing up and living in a way that people look at it and say, ‘I’ll have what she’s having.’
This is your ‘Harry Met Sally’ moment. This is that restaurant scene. This is your moment to be a person who outlasts the half-life of the propaganda reflex. And I’ve seen way too many people try to engage energetically in the debate where they enter into conflict and it destroys their well-being.
Don’t be the miserable angry one. Be the one at the table who is the one worth looking at and going, ‘I’ll have what he’s having. I’ll have what she’s having.’ Live a life that is desirable, and you’ll see propaganda become emasculated instantaneously …
All the time while Gov. [Ralph] Northam here in Virginia was telling us that we could not have gatherings, we continued our workshops. We had our table full of 15, 20, 25 people, and our official policy was that if you signed up for our workshop, for the time you were in our home we adopted you as family, because the legal exemption in Virginia was that family didn’t count.
So, we adopted everybody for the week. We had every kind of cousin, uncle, aunt, brother, sister, child, granny. It was all family. We went through the entire shutdown having a table full of fellowship. And you know what? Everybody in the neighborhood said, ‘I’d love to have what they’re having.’”
_________________
For more:
- https://madisonarealymesupportgroup.com/2021/08/10/pfizer-whistleblower-confirms-covid-injection-is-a-bioweapon/
- https://madisonarealymesupportgroup.com/2021/09/24/wuhan-scientists-planned-to-release-chimeria-covid-spike-proteins-into-bat-populations-using-skin-penetrating-nanoparticles/
- https://madisonarealymesupportgroup.com/2020/09/19/whistleblower-states-covid-19-made-in-a-lab/
- https://madisonarealymesupportgroup.com/2021/09/09/new-docs-show-fauci-lied/
- https://madisonarealymesupportgroup.com/2021/09/20/fauci-up-to-his-neck-funding-coronavirus-research-in-wuhan-documentary-tonight-8-p-m/
- https://madisonarealymesupportgroup.com/2021/10/01/beyond-doubt-there-was-an-incident-at-the-wuhan-institute-of-virology/
- https://madisonarealymesupportgroup.com/2021/06/16/world-exclusive-footage-proves-bats-where-kept-in-wuhan-lab/
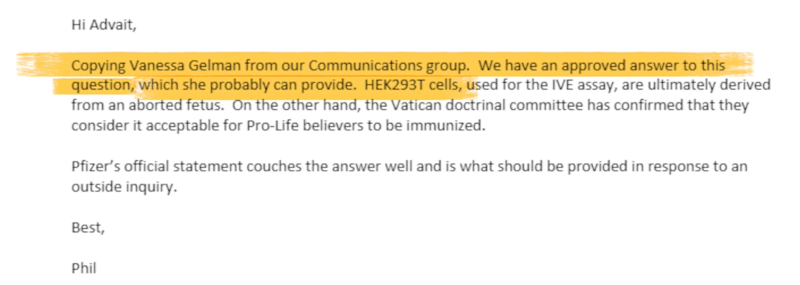
 Vanessa Gelman, who serves as Pfizer’s Senior Director of Worldwide Research, encouraged staff to be careful when talking about human fetal cells in the company’s vaccine program.
Vanessa Gelman, who serves as Pfizer’s Senior Director of Worldwide Research, encouraged staff to be careful when talking about human fetal cells in the company’s vaccine program.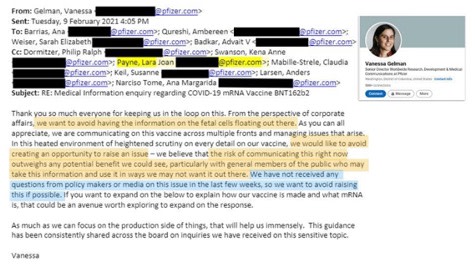 In another email thread, Gelman doubled down on being secretive about this information.
In another email thread, Gelman doubled down on being secretive about this information.