Join us live on Monday 11 March to learn all about fasting with Christof Plothe, DO. As millions of people begin fasting around the world, let’s explore what the science says about this practice and the different ways to do it.
Animals and children refuse to eat when getting sick. What are the hidden secrets of fasting that science is just discovering with the insights on autophagy?
Christof is an osteopath and author as well as a member of the World Council for Health Steering Committee. He works in the field of integrative medicine, combining naturopathy, environmental medicine, and holistic dentistry with conventional medicine.
What the Science Says About Fasting: A Low Cost Approach to Health
Please note: Daylight Saving Time begins in the US, Canada, some parts of Mexico, etc. this weekend, making Monday’s show one hour later than previously.
Time zone guide: 11 am PDT, 1 pm CDT, 2 pm EDT, 6 pm UTC / GMT, 8 pm CAT, 3 am JST (12 March), 5 am AEDT (12 March), 7 am NZDT (12 March)
People who tested positive for COVID-19 and took ivermectin as a treatment recovered faster than a comparison group, a new study found.
The time to self-reported recovery was a median of two days faster among the ivermectin recipients, according to the large UK study.
The quicker recovery period was statistically significant.
People who received ivermectin were also less likely to be hospitalized or die, with 1.6 percent of ivermectin recipients being hospitalized or dying versus 4 percent of the comparison group, which received typical care, which in the UK is largely focused on managing symptoms.
Ivermectin recipients also enjoyed a reduction of severe symptoms and sustained recovery, according to the study.
Only in the topsy-turvy world of COVID do study authors rewrite positive findings into negative ones
The PRINCIPLE trial came up with an unneeded specified hazard ratio to make the findings appear insignificant. In the real world, if a HR is >1.0, and is statistically significant, it is a robust finding.
Further, the findings should be interpreted in the context of
recipients only receive ONE dose per day across three days
recipients received ivermectin a median of 5 days after symptom onset, a time some consider to be too late since the drug works best within 24 hours according to a meta-regression
There have been additional studies that found ivermectin works against COVID-19.
Dr. David Boulware who helped run the trial argued that faster recovery with ivermectin was similar to the open-trial findings of molnupiravir; however, according to James Lyons-Weiler, the FDA dropped the ball completely on this supposed ‘game changer’ which gave people higher live SARS-CoV-2 viral titers and more viral evolutiontwo weeks after start of treatment, but was still FDA approved.
Go here for a quick review of costs between FDA approved and FDA unapproved COVID treatments. This says it all.
Results from the Oxford-managed PRINCIPLE trial of ivermectin in out-patient Covid-19 were published in the Journal of Infection on 29 February 2024, over a year and half after the trial’s closure in July 2022, and over 2 years since the originally planned termination. The unexpected pause in January 2022 (said to be due to supply problems, denied by the supplier) remains unexplained. PRINCIPLE is funded by the NIHR, i.e. by the British taxpayer.
The trial design was criticised by FLCCC and BiRD International on 1 July 2021, because of enrollment up to 14 days of symptoms. The comprehensive summary of clinical evidence at c19ivm.org thus categorises this as a “Late Treatment” RCT. The protocol treatment, with weak dosing, short duration, fasting administration minimising serum concentrations, confined to a monotherapy with disregard of ubiquitous adjuncts, and of the concurrent corticosteroids indicated at later disease stages, did not correspond to any treatments adopted by clinicians using ivermectin with success. Overall the majority of patients were low-risk, after enrollment criteria were changed in July 2021 to accommodate all adults.
In spite of the low-risk population, under-dosing, and late treatment,statistically significant improvements in times to recovery on various metrics are found, Fig. S6(b) opposite, though not graphed in the main paper. The authors’ summary rejects these as not clinically significant, based on an arbitrary, pre-defined, metric: – “Ivermectin for COVID-19 is unlikely to provide clinically meaningful improvement in recovery, hospital admissions, or longer-term outcomes. Further trials of ivermectin for SARSCov-2 infection in vaccinated community populations appear unwarranted.” This does not follow from the evidence.A rational response to statistically significant improvement in recovery time, demonstrating a positive quantified effect, would be to seek to optimise the protocol. Also the alleviation of Post-Acute Sequelae of SARS-Cov-2 (PASC) i.e. “Long Covid”, as detailed here from data in the Supplementaries, is clear, and at variance with the negative conclusion on “longer term outcomes”.
BiRD International and the World Council for Health agree however that further trials of ivermectin alone are unwarranted, the weight of evidence summarised at covid19.org being so overwhelming that the remaining issues concern dosage, adjuncts, and mechanism, rather than further empirical evidence of clinical effect. The paper’s opening statement “The evidence … is contested” does not survive scrutiny of all available evidence, even after this report.Multiple critiques of design and implementation remain unanswered, data sharing is only offered subject to contracts, and an undeclared conflict of interest is Prof Chris Butler’s parallel PANORAMIC trial of molnupiravir, a proprietary drug.
We find the results unsurprising in view of the poor trial design; they do little or nothing to refute the accumulated worldwide evidence on the efficacy of ivermectin in Covid-19.
_______________
**Comment**
And there you have it. Yet another manipulated study for a pre-determined outcome by an author with a vested interest in a treatment that competes with ivermectin.Case closed.
March 6, 2024 – Last week the CDC’s Advisory Committee on Immunization Practices (ACIP) gathered for their regularly scheduled February meeting. The ACIP traditionally meets three times per year in February, June, and October. COVID upended that, with 10 meetings in 2020, 17 in 2021, 11 in 2022, and seven in 2023.1 The ACIP started this year with a notable eight vacancies on the panel, so for this meeting, members of the federal government stepped in as voting members. Topics included the expected: shots for COVID, flu, polio, pneumococcal, and meningococcal, alongside discussions revisiting guidance for diphtheria, tetanus, and pertussis, and newly-licensed, fast-tracked chikungunya vaccines.
Four votes were taken; each passed easily. The first added another recommended 2023-2024 version of the COVID shot for those over 65. The committee spent over 30 minutes discussing whether the recommendation language would be more effective at getting shots in arms if the CDC says people “should” get the shot versus “may” get the shot. The difference is, if the CDC says people “may” get a shot, it sounds more like permission and would create discussion with providers about individual patient needs, while “should” more clearly supports their end goal of directing one-size-fits-all medicine. In the end, push came to shove and the crew decided “shared decision making” was too weak and confusing and went with “should.” Is it curious that the ACIP spent a hefty chunk of time debating the subtleties of persuasive language? Were there other topics that that went ignored?
The committee also voted to update Vaccines for Children (VFC) guidelines for combination vaccines containing tetanus, diphtheria, and pertussis. This is significant because VFC earmarks taxpayer money to supply free vaccines to poor children only if the vaccine is specifically added to the list. But these combo shots have been given to children since the 1970s. What changed? The stated reason for doing this was because an unnamed maker of the only DT vaccine (who happens to be Sanofi), discontinued manufacturing.2 The DT vaccine was recommended for children who had a reaction to the pertussis component of DTaP, or people who showed up in the ER for potential tetanus exposure. DT will be replaced with Td, also manufactured by Sanofi, and containing less diphtheria toxoid than DT. (For a review of the alphabet soup of this combo shot, check out our article “Shining a light on Pertussis, the vaccine that opened the courthouse doors.”)
Strangely, the group voted to add Td, manufactured by MassBiologics, to the VFC resolution to authorize taxpayer dollars for free vaccines despite acknowledging the company’s very recent decision to discontinue manufacture of the product. There was no discussion about why either product was being discontinued, but Sanofi cited “minimal demand” in a letter to customers,3 and the maker of TdVax revealed the FDA was investigating some of its lots in 2022.4 One member of the committee, Dr. Chan, did not vote because he disclosed an active collaboration with MassBiologics. What does this curious vote mean for Americans? Moving forward, children who have a reaction to DTaP may be able to access Td (with lower doses of diphtheria toxin than DT) as long as there are no supply shortages, however, people going to the ER with a wound will most likely not be able to access a shot that does not include pertussis. Our article “Shining a light on tetanus: The case of the rusty nail and the anti-fertility vaccine” explains why doctors push the Dtap shot when they see open wounds.
Two further votes sailed through for the first-ever chikungunya vaccine to be recommended for lab workers and anyone traveling to a country where there is an increased risk of the mosquito-borne illness. Chikungunya commonly causes fever and joint pain and, according to the WHO, most people fully recover and have lifelong immunity.5 Serious or long-term illness occurs typically only in the very old or very young and those with complications. Unfortunately, the FDA’s press release announcing licensure in November 2023 makes one wonder if the cure is worse than the illness itself for the healthy traveler or lab worker:
The FDA’s announcement further explains that the vaccine was granted “Accelerated Approval,” based on whether a product may be effective. There’s no mention of safety requirements, and the press release admits that adverse reactions did not happen in the placebo group, and that it is unknown whether the vaccine will cause adverse effects in newborns. The FDA is relying on the manufacturer to do postmarket surveillance to gather safety data. In other words, we’ll figure out how safe this is after we sell it and see what happens.
There’s no information on the safety or efficacy for mom or baby, because it’s general practice not to test vaccines on pregnant women. There’s also no “human data” on whether vaccine virus or antibodies are present in breast milk after vaccination. Two pregnant women who were inadvertently included in clinical trials both had miscarriages after the vaccine was administered (none in the placebo group did), and the miscarriages were not attributed to the shot.
Regardless, the ACIP did not exclude or add precautions to their recommendation for pregnant women.
AS YOU CAN SEE, THERE WAS A LOT MISSING FROM THE MEETING DISCUSSION. HERE ARE JUST A FEW OF THE THINGS LEFT UNSAID DURING THE COVID DISCUSSIONS:
Data about hospitalization for COVID in children wasn’t given, though there was a full presentation on adult hospitalization.
Public attitudes about the shot, and top concerns were presented in the context of addressing why people haven’t gotten all the shots, and notably absent was any discussion of people’s concerns, which included serious or mild side effects, and whether the shot worked at all.
COVID vaccine safety presentations still did not address the safety signal from VAERS data and deaths.
Efficacy data presented did not include inquiry into “negative efficacy,” meaning questions of whether those vaccinated are more likely to get COVID.
Why efficacy data was discontinued after a very short 119 days.
Economic analysis also didn’t include the possibility of breakthrough infections in estimating years of life and money saved.
“Available data” addressing the acknowledged signal for stroke associated with the shot was “inconsistent,” with the claim “most” results didn’t show an association…which leaves one wondering if there are studies that have shown those results which were not disclosed or discussed.
There was no discussion about why they recommend a 2nd 2023-2024 shot for those over 65 at four months rather than the typical 2 month wait between shots.
There were references to differences in opinion among Working Group members regarding the 2nd shot recommendation, but full disclosure of those differences was absent.
There were comments about returning to strain recommendations at least yearly, but no discussion on why we need new strains every year.
HERE ARE SOME THINGS THEY DID SAY ABOUT THE COVID SHOTS:
“I totally acknowledge that lots of people don’t want it…anything we can do to lower the barrier of getting a vaccine in someone’s arm is just wonderful.”
“We know efficacy wanes.”
“98% of people have natural or vaccine immunity.”
[There are] “lots of questions, probably unanswerable.”
What an absolute dog and pony show. Do not trust these people. At all.
The other little factoid not mentioned at the ACIP meeting was that they proclaimed all COVID gene therapy (40 in total) injections were 100% effective, but ZERO actually work.
In 2024, there is still no cure or proven “vaccine” for any respiratory disease.
Though this is totally redacted, it shows us 3 things:
1. The CDC has TOTAL contempt for members of the public
2. Its blank BECAUSE the findings show that the vaccine causes myocarditis. If it didn’t cause myocarditis then they would not be hiding the results.
3. When they say “follow the science” they mean follow it blindly.
**UPDATE**
There is now an obvious concern about receiving a blood transfusion using COVID ‘vaccinated’ blood.This article based on a Twitter post relays an important patient case of a COVID ‘vaxxed’ blood transfusion causing blood clotting and pericarditis. Another unfortunate example of this is the death of a baby who died of blood clots after the hospital gave him a blood transfusion using “vaccinated” blood against the parents’ wishes. The hospital somehow managed to “lose” the specially donated unvaccinated blood by a family friend, so have an advocate with you if you are in the hospital.
Similarly to the redacted pages and blind refusal to admit the injections are even causing widespread blood and heart problems, researchers are carefully toeing the narrative by stooping so low as to compare the potential for life-altering health issues to a historical example of denying blood based upon race (the old race card). There is quite a difference between the two when you consider the potential life-altering damage or even death from COVID ‘vaxxed’ blood. It’s simply easier to call it all ‘misinformation.’
I have lived in New Paltz, New York, my whole life and throughout that time, have grown accustomed to many of the seemingly odd local rituals that our town performs.
One of these oddities is that in elementary school, New Paltz students learn to tuck their jeans into their socks, stuffing them full until their feet look like weird upside down sock puppets before departing on a field trip.
This is all part of the general awareness for ticks that the Hudson Valley strongly promotes to its residents. Students learn to buddy up and do tick checks and their noses often become normalized to the scent of DEET as parents worryingly spray down their clothes. (See link for article)
______________
**Comment**
Bredberg admits that he became infected when tick awareness was nowhere near what it is today. Similarly to others in Lymeland, despite severe hallmark symptoms all tests returned ‘negative.’
If it wasn’t for a relentless mother, he probably never would have gotten help.
Unfortunately he uses the wrong statistic that up to 20% go on to suffer long-term symptoms when in reality it’s somewhere between 40-60%. I also must disagree that ‘research, treatment, and awareness has come a long way from where it was 10 years ago.’
Despite climbing numbers, we are no further along in understanding why some develop chronic Lyme/MSIDS and others don’t, and how to effectively treat it.
While awareness efforts have increased, this is entirely due to sick people who have done what they can in their sphere of influence.
Many are unaware that the climate narrative is part and parcel of this global endgame and that drastic and irreversible climate engineering worries real scientists who state the endeavor should be relegated to the fantasy realm and science fiction.
Disgusted Climate Scientist, Judith Curry, PhD, once one of the strongest scientific voices in the race to fight global warming, has now been labeled a “climate contrarian”.
Hear the data behind this marked reversal and why she believes the “climate change crisis” is politically motivated.
POSTED: March 1, 2024
I started criticizing scientists for not making their data publicly available, for not being transparent about their method and they quickly started labeling us a denier and tried to discredit me.
Anybody who speaks up in opposition to this established UN narrative gets ignored, marginalized, cancelled, insulted, and so on. ~ Judith Curry, PhD
At about 13:00, Curry explains that in 2009, hacked ‘Climategate’ emails exposed that Intergovernmental Panel on Climate Change (IPCC) authors were trying to avoid FOIA requests and rig the peer-review process.
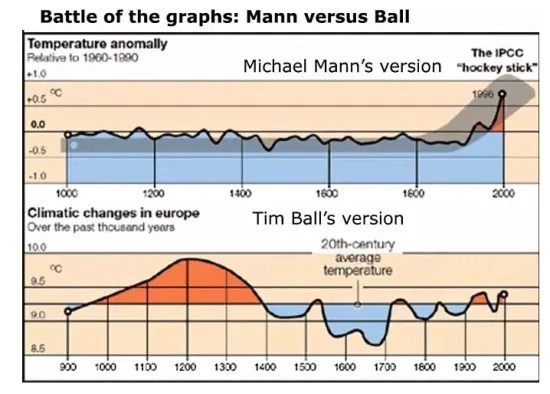
Previously to this, IPCC canonized and heavily promoted the infamously fraudulent hockey stick graph which relies on junk science and the proxy evidence from the tree rings of a single Yamal larch! The graph was discredited in 2003.
Dr. Ball spent over eight years of his life defeating in a court of law not one top IPCC climate scientist, but two. It is more than mere coincidence that Dr Ball, a world-leading skeptical climatologist, was systematically targeted for legal retribution time and again by political groups such as the unscrupulous Climate Science Legal Defense Fund. As a retired scientist in his 80’s, he was a easy picking, and the stress of these lawsuits put an enormous toll on his health. He managed to write a damning book of the 30-year back story of the great climate fraud titled ‘The Deliberate Corruption of Climate Science.’
Please note Ball’s fraudulent hockey stick graph vs factual data used by Dr. Ball.


 Please note: Daylight Saving Time begins in the US, Canada, some parts of Mexico, etc. this weekend, making Monday’s show one hour later than previously.
Please note: Daylight Saving Time begins in the US, Canada, some parts of Mexico, etc. this weekend, making Monday’s show one hour later than previously.