
More CDC Shenanigans; Changes COVID Testing & Violates Federal Law to Inflate Cases – Investigation Petitions Sent To All U.S. Attorneys & DOJ
CDC Rewrites COVID Testing Measures for Post-Vaccine Breakthrough Infections
In a move to investigate COVID-19 breakthrough infections among persons vaccinated against the virus, the U.S. Centers for Disease Control and Prevention has announced new and revised testing measures just for vaccinated individuals.
Previously, the CDC had recommended something called a PCR threshold of 40, meaning that the test would be considered positive even if it took 40 testing cycles to find a tiny shed of virus. During the height of the pandemic, critics said that threshold was too high, as it was marking people positive when they actually had only genetic fragments or leftovers from an infection that posed no risk of contagion.
The New York Times likened those tests as “akin to finding a hair in a room long after a person has left.”
Criticisms aside, the high threshold testing procedure stayed in place — until now.
With more and more breakthrough cases being reported, the CDC quietly changed its PCR threshold for testing breakthrough infections to 28 or less.
This means that far fewer cases will be identified as positive than were they to stay at the 40 threshold.
“The entire epidemic would have looked very different if [28] had been used [for a regular infection],” Alex Berensen tweeted.
On its website, the CDC noted that it also would not test every breakthrough case, but instead would “focus on identifying and investigating only vaccine breakthrough infections that result in hospitalization or death” — a move that will also lower the total case counts among vaccinated individuals.
SOURCES:
CDC Vaccine Breakthrough Testing Measures
CDC Breakthrough Case Investigations April 16, 2021
The New York Times August 29, 2020
_______________________
**Comment**
Regarding the PCR testing the whole house of cards is built upon, please see the following quote from its creator:
This informative article also points out the complete hypocrisy when it comes to counting COVID deaths vs vaccine-related deaths. The CDC accepts ALL suspected cases and records them as COVID deaths, even false positives cases and cases with serious underlying health conditions. The corrupt CDC also conveniently stopped counting seasonal flu and funneled those numbers to increase COVID deaths as well.
Yet when a completely healthy person with no underlying condition dies within hours and days following the experimental, fast-tracked, dangerous COVID injections that don’t even fit the criteria of being vaccines, the CDC completely denies any connection.
The CDC has a long and sordid history of denying anything that doesn’t fit its accepted narrative, including the very real Lyme/MSIDS epidemic.
Anyone else smell a skunk?
__________________
CDC Violated Law to Inflate COVID Cases and Fatalities
STORY AT-A-GLANCE
- Dr. Henry Ealy and his team started looking at CDC data on COVID-19 cases and fatalities in mid-March 2020, quickly realizing the agency was vastly exaggerating fatalities
- Over-reporting of fatalities was enabledby a March 2020 change in how cause of death is reported on death certificates. Rather than listing COVID-19 as a contributing cause in cases where people died from other underlying conditions, it was to be listed as the primary cause
- As of August 23, 2020, the CDC reported 161,392 fatalities caused by COVID-19. Had the long-standing, original guidelines for death reporting been used, there would have only been 9,684 total fatalities due to COVID-19
- The CDC violated federal law, as the Paperwork Reduction Act requires data collection and publication to be overseen by the Office of Management and Budget. Proposed changes must be published in the Federal Register and be open to public comment. None of these transparency rules were followed
- We don’t yet know who was responsible for altering the reporting rules in violation of federal law. To identify the culprits, formal grand jury investigation petitions have been sent to all U.S. attorneys and the U.S. Department of Justice,requesting a thorough, independent and transparent investigation; a direct public effort to gather signatures also commenced on the one-year anniversary of the CDC reporting change
Dr. Mercola Interviews the Experts
This article is part of a weekly series in which Dr. Mercola interviews various experts on a variety of health issues. To see more expert interviews, click here.
In this interview, Dr. Henry Ealy, ND, BCHN, better known as Dr. Henele, a certified holistic nutritionist and founder/executive community director of the Energetic Health Institute,1 reviews how U.S. federal regulatory agencies have manipulated COVID-19 statistics to control the pandemic narrative.
He earned his doctorate in naturopathic medicine from SCNM. After graduating from UCLA with a bachelor of science in mechanical engineering, he worked for a major aerospace company as a primary database developer for the International Space Station program.
He holds over 20 years of teaching and clinical experience and was the first naturopathic doctor to regularly teach at a major university in the U.S., when he headed up a program at Arizona State University on bioanxiety management.
As he points out, he’s an avid data collector. In October 2020, Henele and a team of other investigators published a paper2 in Science, Public Health Policy and the Law, titled, “COVID-19 Data Collection, Comorbidity & Federal Law: A Historical Retrospective,” which details how the U.S. Centers for Disease Control and Prevention has enabled the corruption of case- and fatality-reporting data in violation of federal law.
Accuracy of Data Is Paramount for Public Health Policies
The team started looking at CDC data on COVID-19 cases and fatalities in mid-March 2020. He explains:
“What I started doing on March 12 was going through all the data we could find from the Italian Ministry of Health and South Korea. We couldn’t validate any of the data coming out of China. There was just no independent way to do it. What we were seeing out of Italy and South Korea was that we were going to be concerned about people who are over 60, over 70 years of age with preexisting conditions.
That was the main thing coming out of that data. So, we were expecting the same kind of trends here … I started tracking the data on a daily basis from each state health department, and then making sure that what the CDC was reporting was matching up.
What we started to see, very early on, were some significant anomalies between what the states were reporting and what the CDC was saying. It was concerning, because the variance was growing with each day. We have an old saying: ‘Garbage in equals garbage out.’ And that was the concern, because we knew public health policies are going to be based upon the data, so accuracy is of paramount importance.
Then we started delving in a little deeper into how the CDC was supposedly collecting their data. That’s where we saw the National Vital Statistics Systems (NVSS) March 24 guidelines, which were very concerning, and we saw the CDC adopt the Council for State and Territorial Epidemiologists paper on April 14.
What was incredibly concerning about this was that it was all done without any federal oversight, and it was all done without any public comment, especially scientific comment. That became increasingly problematic. We started to see discrepancies in the state of New York alone, in the thousands of fatalities.”
Special Rules for COVID-19 Fatalities Were Implemented
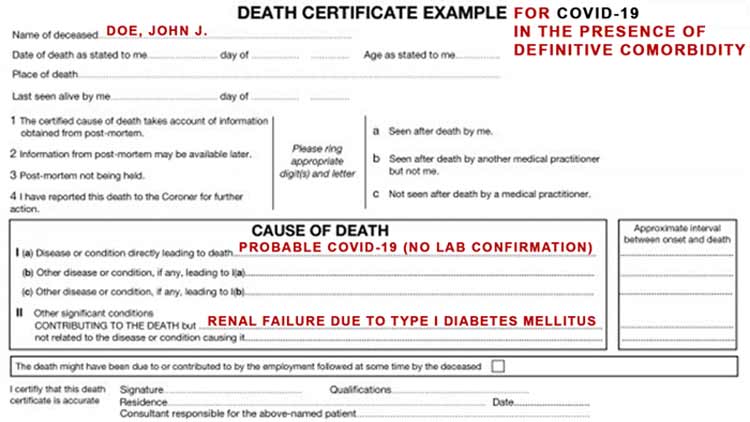
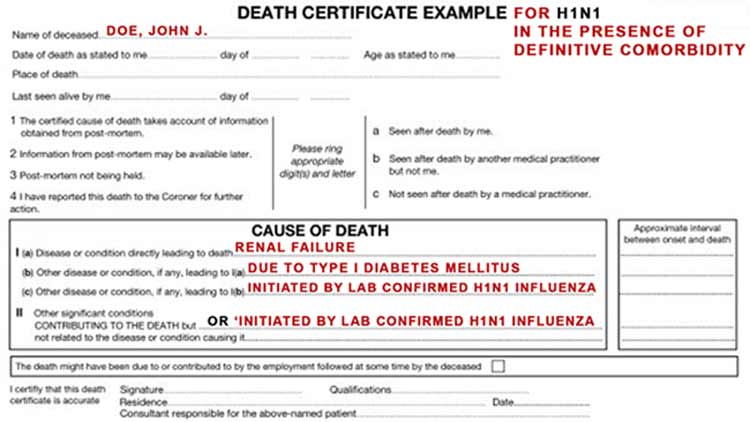
Importantly, in March 2020, there was a significant change made to the definition of what a COVID-19 fatality was. As explained by Henele, there’s a handbook on death reporting, which has been in use since 2003. There are two key sections on a death certificate. In the first part, the cause of death is detailed. In the second part, contributing factors are listed.
Contributing factors are not necessarily statistically recorded. It’s the first part, the actual cause of death, that is most important for statistical accounting. March 24, 2020, the NVSS updated its guidelines on how to report and track COVID-19-related deaths.
“They were saying that COVID-19 should be listed in Part 1 for statistical tracking, but [only] in cases where it is proven to have caused death, or was assumed to have caused death,” Henele explains.
“What was really concerning about this document was that it specifically stated that any preexisting conditions should be moved from Part 1, where it has been put for 17 years, into Part 2.
So, it was basically taking this and saying, ‘We’re going to create exclusive rules for COVID-19 and we’re going to do a 180 for this single disease …’ The big problem with that is that now you remove the ability for a medical examiner, a coroner, a physician, to interpret [the cause of death] based upon the collective health history of that patient …
You remove their expertise, and you say, ‘You have to count this as COVID-19.’ That takes on an added measure when you incentivize it financially, and that’s what we saw with some of the Medicare and Medicaid payouts …”
Who’s Responsible?
Who has the authority to do this? The answer is “no one.” A federal agency has the ability to propose a data change, at which time it would be registered in the Federal Register. At that point, federal oversight by the Office of Management and Budget kicks in, and the proposed change is opened up for public comment.
Since they did not register the proposed change, there was no oversight and no possibility for the public to comment on the change. Basically, what happened is that these changes were simply implemented without following any of the prescribed rules. “They acted unilaterally, and that’s not how [it] is supposed to work,” Henele says.
As to who took it upon themselves to alter the reporting rules, we don’t know. To identify the culprits, Henele and his team have sent out formal grand jury investigation petitions to every U.S. attorney and the U.S. Department of Justice (DOJ), requesting a thorough, independent and transparent investigation.
“We did it at both state and federal levels. We have sent physical copies to every U.S. attorney and their aides. We sent out over 247 mailings in October [2020],” Henele explains. “We sent out an additional 20 to 30 to various people at the Department of Justice …
They would have the ability to call a grand jury, and that grand jury would have the ability to subpoena all those records to determine who were at fault … All we need is one U.S. attorney. All we need is one person at the Department of Justice to take up the cause.”
Dramatic Implications
The consequences of that change in the definition of the cause of death where COVID-19 is involved have been dramatic. For the full implications, I recommend reading through Henele’s peer-reviewed paper, “COVID-19: CDC Violates Federal Law to Enable Corruption of Fatality-Reporting Data.”3
“We’ve accumulated about 10,000 hours of collective team research into this [paper]. It’s been reviewed by nine attorneys and a judge for accuracy. It’s gone through the peer-review process before being published. We feel it’s tight.
On page 20 of the paper, we have a big graphic showing what the estimated actual fatality count should have been as of August 23, 2020. What was reported on August 23 was 161,392 fatalities caused by COVID-19 …
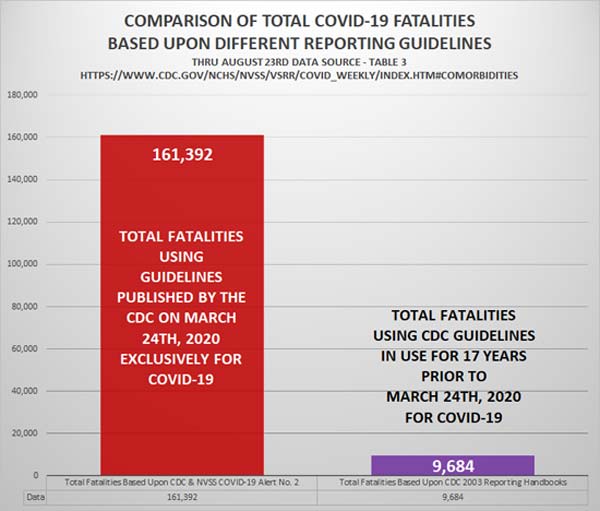
Had we used the 2003 guidelines, our estimates are that we would have roughly 9,684 total fatalities due to COVID-19. That’s a significant difference. That’s a difference on the scale of as much as 96%. The range that we calculated was 88.9% to 96% inflation.“
Indeed, this matches up with an admission by the CDC in late August 2020, at which time they admitted that only 6% of the total death count had COVID-19 listed as the sole cause of death. The remaining 94% had had an average of 2.6 comorbidities or preexisting health conditions that contributed to their deaths.4
“For absolute 100% accuracy, we’d have to do something like what we were just alerted to by a whistleblower in Florida, where they’ve actually gone in and reexamined every single death certificate and the medical records with them. What they found was that roughly 80% of the fatalities were wrongfully classified as COVID-19 fatalities,” Henele says.
Science Foundations Have Been Violated
Mainstream media have justified pandemic measures “based on the science,” yet the very foundation of science has been violated. The ramifications are enormous, from the destruction of local economies and skyrocketing suicide rates to people being forced to die alone, their family members being barred from being at their bedside during their last moments.
“I lost my mother in in 2002,” Henele says. “The grace of it all was that we were able to get her out of the hospital and fulfill her last request, which was to pass away in her bed with family around her. I grieve for every single person who’s lost someone [during this pandemic] who was not able to be there.
Americans should not have to die alone because we’re worried about some virus that they’re telling us is a problem, when the data, even the data that we know to be inflated and fraudulent, still doesn’t suggest the virility that they want us to believe.”
COVID-19 Timeline
In their paper, Henele and his team detail a timeline of the COVID-19 pandemic and federal laws that impact data handling. Here’s a summary:
|
In 1946, certain administrative procedures were implemented. The Administrative Procedures Act requires federal agents and agencies to follow certain rules to get things done. These rules are to ensure transparency in government.
In 1980, the Paperwork Reduction Act was written into law. In 1995, the Act was amended, designating the Office of Management and Budget (OMB) as the oversight body for all federal agencies’ data. In October 2002, the Information Quality Act was implemented, which doubles down even further on the accuracy and integrity and data gathering. This act requires federal agencies to meet explicit criteria in order for their data to be published and analyzed. |
|
In 2005, the Virology Journal published research demonstrating that hydroxychloroquine has strong antiviral effects against SARS-CoV (the virus responsible for SARS) primate cells. This finding was hailed by Dr. Anthony Fauci, Henele notes. In other words, 15 years ago, Fauci admitted that hydroxychloroquine works against coronaviruses. This is public record. As reported in “The Lancet Gets Lanced With Hydroxychloroquine Fraud” and “How a False Hydroxychloroquine Narrative Was Created,” the myth that this drug was useless at best and dangerous at worst was purposely created using falsified research and trials in which the drug was given in toxic doses. This fraudulent research was then used to discourage and in some cases block the use of hydroxychloroquine worldwide. As noted by Henele, “It’s not science. We’re in this very weird faith-based model of science, which isn’t science at that point.” |
|
In 2014, Fauci authorized $3.7 million to the Wuhan Institute of Virology (WIV). In 2019, WIV received another $3.7 million. In both instances, this funding was for gain-of-function research on bat coronaviruses. |
|
October 18, 2019, Johns Hopkins Center for Health Security hosted Event 201, in conjunction with the Bill & Melinda Gates Foundation, the World Economic Forum and a few other financial partners. November 17, 2019, China recorded the first known case of COVID-19.
|
|
January 29, 2020, the White House installed a coronavirus task force, which included Fauci and then-CDC director Dr. Robert Redfield, as well as Derek Kan, then-deputy director of the OMB.
|
|
March 9, 2020, the CDC alerted Americans over 60 with preexisting conditions that they might be in for a long lockdown out of safety concerns. March 24, the CDC changed how COVID-19 is recorded on death certificates, de-emphasizing preexisting conditions and comorbidities, and basically calling all deaths in which the patient had a positive SARS-CoV-2 test a COVID-19 death.
|
|
April 14, 2020, the CDC adopted a position paper from a nonprofit, the Council for State and Territorial Epidemiologists, which identifies every single methodology for how to report a probable COVID-19 case, a confirmed COVID-19 case, an epidemiologically-linked or contact-traced COVID case.
|
Transparency Rules Have Been Grossly Violated
So, what exactly is the connection between the Paperwork Reduction Act and the COVID-19 fatality data? Why is it so important?
“Well, the Paperwork Reduction Act is really about establishing oversight,” Henele explains. “It established the Office of Management and Budget, the OMB, which is under the executive branch. It established them as the key agency for oversight of all data in the entire federal government.
So, when you start seeing IHME [Institute for Health Metrics and Evaluation] out of the University of Washington — which is heavily funded by the Bill & Melinda Gates Foundation, to the tune of $384 million in two installments — when you see their data being used at federal levels, you go and look at the Federal Register and you say, ‘OK, where is the 30 to 60 days that we were supposed to have to comment on the use of that data?’
Public comment is part of the Paperwork Reduction Act. That’s what it’s all about. What we saw instead was just, ‘Hey, this is what the IHME is putting out there. We’re going to go with it.’ Well, you can’t do that if you’re a federal agency … IHME is … technically an independent organization, but they don’t have any governmental designation.
They’re not a 501(c)(3), they’re not a 501(c)(4), they’re not a 501(c)(6). They’re just this amorphous nongovernmental organization within our country, and it’s kind of concerning. We’re doing more research on that, but it’s very, very concerning because they don’t have anybody to account to.“
Test-Based Strategy Has Been an Egregious Fraud
In addition to the manipulation of fatality statistics, the statistics of “cases” were also manipulated. Traditionally, a “case” is a patient who is symptomatic; someone who is actually ill. When it comes to COVID-19, however, a “case” suddenly became anyone who tested positive for SARS-CoV-2 using a PCR test, or worse, assumed positive based on proximity to someone who tested positive.
I’ve detailed this fraud in many previous articles over the past year, including “Coronavirus Fraud Scandal — The Biggest Fight Has Just Begun” and “The Insanity of the PCR Testing Saga.” “Cases” were also counted multiple times, as explained above. Henele expounds on this issue, noting:
“The CDC specifically enacted what’s called a test-based strategy, which we’ve never done before in medicine for anything. What that test-based strategy means is if you test positive, you got [COVID-19]. But what they didn’t do for the PCR testing was they didn’t identify the agreed upon number of cycles across all states across all labs that are testing.
What most people don’t know is that the closer you get to zero in terms of cycle times, the more likely that the result is going to be negative. The closer you get to 60, the more likely that it’s going to be positive.
Well, we’ve never seen a document coming out of the FDA, coming out of the CDC, coming out of any of the state health departments, that says, ‘We need all labs to be at this specific cycle [threshold]. And if a person is not deemed positive with that number of cycles, then they are not positive.’ So, there’s just flaw after flaw after flaw.”
Data Manipulation Created COVID-19 Pandemic
Most labs used cycle thresholds above 40 — as recommended by the CDC and the World Health Organization — which exponentially increased the likelihood of a positive test, even among completely healthy and noninfectious individuals. The only justification for all of this is that it was done to perpetuate the narrative that we were in a raging pandemic, which was then used to justify the unprecedented destruction of personal freedom and the economy.
“The thing I have to give the folks that have been involved in this credit for is the incredible number of sleights of hands,” Henele says. “It’s a little bit here, a little bit here, a little bit here, a little bit here.
And when that happens, it leads to something that is very dangerous scientifically, and very dangerous for public health policy, which is control of data — the ability to manipulate data … and if you can control the data, you get to control the narrative …
If we’re not going to have an absolute, transparent and verifiable data collection process that is based upon accuracy and integrity of that data, then you can turn that [pandemic emergency] dial up and down at your whim. My hope is that the objective scientist within all of us understands that this is bigger than politics. This is beyond it. This is a severely broken system that we have to fix, and we better do it.”
As discussed in many other articles, it appears the COVID-19 pandemic has in fact been a preplanned justification for the implementation of a global technocrat-led control system, which includes a brand-new financial system to replace the central bank-manufactured fiat economy that is now at the end of its functional life. Fiat currency is manufactured through the creation of debt with interest attached, and the whole world is now so laden with debt it can never be repaid.
If people understood how the central banks of the world have pulled the wool over our eyes, we would simply demand an end to the central banks. Currency ought to be created and managed nationally.
The central banks, of course, do not want this reality to become common knowledge, because then they will no longer be able to manipulate all the countries of the world, so they need the economic breakdown to appear natural. For that, they need a global catastrophe, such as a major war, or a fearsome pandemic necessitating the shutdown of economies.
Through this willful manipulation of case- and fatality statistics, the CDC has been complicit in willful misconduct by generating needless fear that has then been used against you to rob you of your personal freedoms and liberties and help usher in this massive transfer of wealth and global tyranny. As noted by Henele:
“People are going to be complicit in their own slavery. People are complicit in putting digital shackles around themselves and really restricting their civil liberties.”
Hopefully, people will begin to understand how pandemic statistics have been, and still are, manipulated to control the narrative and generate unjustified fear for no other reason than to get you to comply with tyrannical measures designed to enslave you, not just temporarily but permanently.
More Information
To understand how we got to this point, please consider reading Henele’s paper, “COVID-19: CDC Violates Federal Law to Enable Corruption of Fatality-Reporting Data.” As noted by Henele:
“I’m looking forward to the day when we look back on this, and go, ‘Oh, we almost fell for one, but we woke up in time and we figured this out. And now we have a good balance of technology, but technology that doesn’t have the right to censor us, technology that doesn’t have the right to control us; we have figured out that having too much control in the hands of too few is not a good recipe for us as a species on this planet.’
We know it doesn’t pass the smell test, so it’s important to get informed and educated and it’s papers like this — and this isn’t the only one out there — that have done the homework. If we’re going to trust someone, it’s important to me that we trust people who’ve done the homework and have no vested interest in the outcome.
My team is a team of volunteers. We all do this in our spare time.We’re not making any money. We’re not going to seek to make any money off of this. We’re doing this because we believe in this country. We love this country and we love the people of this country. When I see people suffering, I have to help. I got to get in and help.
So, if you are an American that wants to help, we are setting up resources for you to be able to get engaged and help us push this forward, maybe grease some of these wheels of justice, so we can get an independent grand jury investigation.”
For additional information, or if you want to help, you can email Henele and his team at COVIDResearchTeam@protonmail.com. You can also use your voice and actions to support an investigation into the CDC’s actions.
Two Easy Ways You Can Take Action
- Add your signature to this petition to help mount public pressure to convene a formal grand jury to investigate allegations of willful misconduct by federal agencies during COVID-19 through Stand For Health Freedom, a nonprofit advocacy organization that Henele and his team have collaborated with
- Send a predrafted, customizable letter through Stand For Health Freedom urging key members of Congress to thoroughly investigate alleged violations of federal law by the CDC that compromised COVID-19 data
__________________________
**Comment**
Excellent, excellent paper which delineates the scam. And, it is a scam.
Notice how the CDC uses testing for COVID in an opposite manner as for Lyme/MSIDS. With tick-borne illness they have rigged testing which purposely took out the most specific band for Lyme, and force patients to meet an incredibly high, yet completely arbitrary testing standard which nearly nobody meets – despite having every symptom in the book!
Similarly with COVID-19, they’ve used these tests to control the narrative, educating doctors that patients must get a positive test to be infected with Lyme/MSIDS and if they don’t – well, they just aren’t infected. Worse yet, many doctors tell patients they have a “false” positive when they do manage to miraculously test positive!
It’s a damned if you do, damned if you don’t scenario we’ve been in for over 40 years, which continues unabated.
And then there’s the issue that most patients are infected with far more than Lyme disease. This fact isn’t even on the radar of most doctors and testing for these infections is as bad if not worse than Lyme disease.
For more on Lyme testing:
- https://madisonarealymesupportgroup.com/2020/03/01/study-cdcs-2-tier-lyme-testing-inaccurate-in-more-than-70-of-cases/
- https://madisonarealymesupportgroup.com/2018/01/16/2-tier-lyme-testing-missed-85-7-of-patients-milford-hospital/
- https://madisonarealymesupportgroup.com/2021/04/02/current-serology-no-better-than-a-coin-toss/
- https://madisonarealymesupportgroup.com/2018/04/03/cdc-deliberately-avoids-direct-detection-testing-methods-for-ld/
- https://madisonarealymesupportgroup.com/2020/11/05/your-lyme-disease-test-results-are-negative-but-your-symptoms-say-otherwise/
There has been a concerted effort against direct testing:
- https://madisonarealymesupportgroup.com/2017/12/13/suppression-of-microscopy-for-lyme-diagnostics-professor-laane/
- There is a current lawsuit due to this suppression: https://madisonarealymesupportgroup.com/2018/05/15/news-release-on-57-1-million-lyme-disease-lawsuit-filed-against-cdc/
- This article also reveals how Lida Mattman’s Gold Standard Culture Method has disappeared thanks to this concerted suppression: https://madisonarealymesupportgroup.com/2019/04/02/transmission-of-lyme-disease-lida-mattman-phd/
- There is NO foolproof diagnostic device or test for Lyme/MSIDS, but there IS a validated questionnaire that doctors should be utilizing: https://madisonarealymesupportgroup.com/2017/09/05/empirical-validation-of-the-horowitz-questionnaire-for-suspected-lyme-disease/
The simple reason for this is our public health ‘authorities’ have patents on tests, vaccines, and treatment guidelines. The same is true for COVID-19 as well.
They also want everyone to take their controversial Lyme (and COVID) injections which would only work if Lyme disease does not cause chronic illness – hence the continual denial of persistent infection.
THE CDC IS NOT TO BE TRUSTED AT ALL and should be disbanded.
We need to stop working with these agencies and raising money for their flawed, biased science that continues to abuse and neglect sick patients.
More on the corrupt CDC:
- https://madisonarealymesupportgroup.com/2021/04/01/cdc-foundation-is-not-a-government-entity-has-many-conflicts-of-interest/
- https://madisonarealymesupportgroup.com/2016/11/29/spider-attacks-cdc/
- https://madisonarealymesupportgroup.com/2021/03/31/stand-for-health-freedoms-peer-reviewed-position-paper-petition-to-investigate-the-cdc/
- https://madisonarealymesupportgroup.com/2020/02/11/how-the-cdc-combats-health-freedom-through-front-groups/
- https://www.change.org/p/the-us-senate-calling-for-a-congressional-investigation-of-the-cdc-idsa-and-aldf
- https://madisonarealymesupportgroup.com/2020/04/03/cdc-centers-for-damaged-credibility/
- https://madisonarealymesupportgroup.com/2020/03/27/cdcs-deadly-testing-fiasco-centralization-of-public-health-authority-a-threat-to-national-security/
.png)


