So thankful someone listened to the entire podcost and broke it down in this handy article. I try to do this but sometimes get overwhelmed with the length and amount of material, and neglected to break down Dr. McDonald’s latest work. I regret this as I consider McDonald an expert and a true help for Lyme patients. Every word that proceeds out of this man’s mouth is informative. Now we can all enjoy the information he presented in the podcast in the article which follows. Enjoy!
Pioneering researcher discusses Lyme links to Alzheimer’s and more
April 4, 2023
From the Tick Boot Camp Podcast:
In this eye-opening episode, Dr. Alan McDonald unveils his latest findings, revealing the connections between Lyme disease and an array of serious health issues, including Lewy body dementia, liver damage, leukemia, brain cancer, and even suicide.
This compelling conversation underscores the urgency of broadening our understanding of Lyme disease to better support and treat patients.
Dr. McDonald’s research has led to several groundbreaking discoveries, including:
Lyme Disease Triggers Lewy Body Dementia: Dr. McDonald has discovered a link between Lyme disease and Lewy body dementia, a neurodegenerative disorder that affects the brain. His research has shown that Lewy bodies contain Borrelia DNA, the bacteria responsible for Lyme disease, challenging previous assumptions about the nature of Lewy bodies.
Lyme Disease Causes Liver Damage: Dr. McDonald has found that nearly 20% of acute early Lyme patients suffer from liver issues related to the disease. Early treatment of Lyme disease can help prevent liver damage and its detrimental effects on the body’s detoxification process.
Lyme Disease Linked to Leukemia: Dr. McDonald’s research has also identified a connection between Lyme disease and chronic lymphocytic leukemia, opening up possibilities for improved diagnosis and treatment options for patients affected by both conditions.
Lyme Disease Initiated Brain Cancer: The podcast highlights Dr. McDonald’s ongoing research on glioblastomas, a form of brain cancer, and its association with Lyme disease. This research has the potential to lead to new treatment options and a better understanding of the disease’s impact on the brain.
Lyme Disease and Suicide: The podcast also addresses the crucial connection between Lyme disease and suicide, emphasizing the importance of understanding and supporting patients struggling with the psychological impact of Lyme disease.
Lyme Disease Intelligently Evades Tests: Dr. McDonald’s research illustrates the Lyme bacteria’s ability to sequester itself in the body, leading to false-negative test results and leaving many Lyme patients undiagnosed and untreated.
It’s also available on Apple podcasts, Google podcast, and Spotify.
______________
**Comment**
As I read this, I was again hit hard with the fact that this seriously incredible information isn’t even on the radar of mainstream research/medicine/public health. After 40 years we haven’t budged on understanding this complex illness which typically includes far more than just Lyme, which is why many call it MSIDS or multi systemic infectious disease syndrome or Lyme and company. Lyme alone is formidable, but add in a few coinfections just as nasty and you are one sick dog. McDonald and a few others are the rare scientists who aren’t led by the government narrative/paradigm and who do not have conflicts of interests that obviously make them biased. Further, they obviously look harder and don’t quit when they get the accepted result.
Hopefully the last few years have awakened many to the fact science has been hijacked; however, science has always been hijacked in many areas and Lyme/MSIDS is one of them. I would put vaccines, cancer, autism, MS, chronic fatigue, and many others in this camp as well. Currently, these diseases are huge money makers and the ‘powers that be’ are raking in royalties and other monies and don’t want their cash cows to stop. Public health is the last thing on their minds. If these diseases are in fact triggered or caused by hidden infections, they could be helped by cheap, already existing antimicrobials that could be repurposed. As we have clearly seen with COVID, those controlling the narrative simply can’t allow this to happen.
Advanced imaging shows Lyme-related brain fog is real
By Nancy Dougherty
Johns Hopkins Medicine Lyme Disease Research Center
There are approximately 476,000 people diagnosed with Lyme disease annually in the US. Of these, an estimated 10-20% suffer from impairing symptoms well beyond the acute phase of infection.
Persistent symptoms include severe fatigue, pain, and cognitive problems. Vexingly, these symptoms can be difficult to validate using current diagnostic tests.
Patients are often told by their health practitioners: “your tests are normal, it’s in your head” (aka psychosomatic).
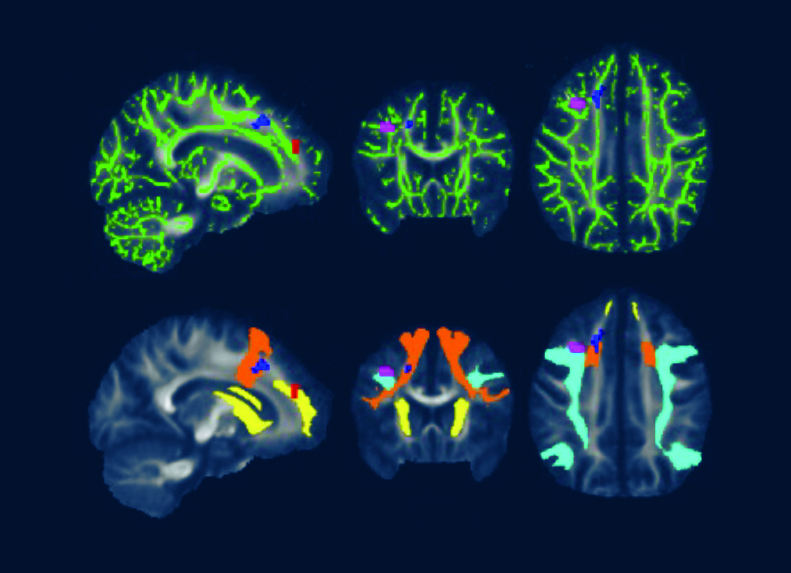
Researchers have discovered, however, that by using more advanced imaging modalities, brain changes can be objectively detected in Lyme disease patients.
For example, clinical researchers at Johns Hopkins University School of Medicine have used novel PET imaging, functional MRI (fMRI), and diffusion tensor imaging (DTI) to identify inflammatory, functional, and structural abnormalities in the brains of Lyme disease patients as compared to healthy controls.
Their findings indicate that Lyme-disease-associated brain alterations are biologic and measurable, not psychosomatic. These discoveries are significant but not yet well known by the physician community or broadly available to clinicians.
What does “brain fog” mean?
Brain fog is a term used to describe difficulties with cognitive functions such as working memory, focusing, concentrating, planning, organizing, word recall, processing speed, and mental fatigue.
Working memory enables one to do tasks quickly or easily solve a problem without looking up information. This includes quickly learning a new computer program or using names or numbers for a routine task.
Mental fatigue is akin to how one feels after taking a long test that requires remembering detailed information or doing a complicated mental task when short on sleep.
What are the limitations of current clinical tests for Lyme-associated brain fog?
Brain fog is commonly experienced by Lyme disease patients but difficult to detect because cognitive deficits can be too subtle for standard diagnostic tests to uncover.
Usual blood tests appear normal in Lyme encephalopathy or brain fog (CBC; CMP: kidney, liver, glucose, thyroid; ESR, CRP).
Serum blood testing for 2-tier IgG Borrelia burgdorferi antibody seropositivity may be negative in patients, such as those with past antibiotic treatment.
Clinically available MRI imaging is usually normal or shows nonspecific changes. Cerebrospinal fluid examination findings are usually normal as well. In some cases, the CSF fluid may show evidence of a mild form of encephalomyelitis, but this is rare.
Formal cognitive testing with a neuropsychologist to characterize the type and severity of cognitive problems can be a more helpful approach. Working memory and processing speed have been shown to be impacted in Lyme disease patients using standardized neuropsychological measures.[i] However, patient-reported cognitive complaints are subjective, and objective measures of cognitive decline are sought after by patients and clinicians.
What does more advanced neuroimaging reveal?
Non-standard research-grade neuroimaging technologies have discovered marked biologic abnormalities in patients with Lyme disease as compared to healthy controls.
A Columbia University brain PET imaging study (2009) found hypometabolism in Lyme-disease-associated encephalopathy.[ii]
A Johns Hopkins University School of Medicine brain PET imaging study (2018) revealed increased inflammation and glial activation in patients with Lyme-disease-associated persistent symptoms.[iii]
A 2022 Johns Hopkins University School of Medicine neuroimaging study utilized fMRI and DTI brain scans in conjunction with each other. These scans identified striking functional abnormalities as well as distinct structural changes in the white brain matter of Lyme disease patients.[iv]
What is the significance of these neuroimaging findings?
John Aucott, MD, Director of the Johns Hopkins Medicine Lyme Disease Research Center and Associate Professor of Medicine at Johns Hopkins University School of Medicine, explains, “The cause of Lyme-disease-associated persistent symptoms typically cannot be identified with regular MRIs, CT scans, or blood tests. However, in a research setting, more sophisticated PET, fMRI, and DTI imaging approaches have found significant objective abnormalities in the brains of Lyme disease patients compared with healthy controls.”
Cherie Marvel, PhD, lead author of the fMRI/DTI study and Associate Professor, Departments of Neurology & Psychiatry at Johns Hopkins University School of Medicine, describes fMRI as “a quantitative ‘brain stress test’ that measures brain function during cognitive tasks.”
Dr. Marvel explains that “the brain scans indicate Lyme disease patients’ brains work harder than normal and unexpectedly by activating white matter in the frontal lobe to try to maintain normal function.”
DTI, a measure of structural brain integrity, confirms abnormalities in the same white matter regions as observed in the fMRI scans.
These novel neuroimaging results provide new objective validation of a biologic basis for the brain fog reported by Lyme disease patients, including working memory impairment and slower processing speed.
The findings indicate Lyme-disease-associated brain fog is real and likely due to ongoing neuroinflammation driving brain dysfunction. More research is needed to better understand the diagnostic and therapeutic implications of these notable discoveries and to bring new insights and more advanced tools into the clinic to help patients.
Big picture
The Lyme-disease-associated advanced neuroimaging brain findings may be relevant to other infection-associated chronic illnesses where neuroinflammation is also significant, including Long COVID and ME/CFS. On June 29-30, 2023, a National Academies of Sciences, Engineering and Medicine workshop will “examine common biological and clinical factors associated with infection-associated chronic illnesses.” Infection-associated brain fog is one topic this workshop can hopefully shine additional light on to help accelerate knowledge and solutions for patients.
[i] Touradji P, Aucott JN, Yang T, Rebman AW, Bechtold KT. Cognitive Decline in Post-treatment Lyme Disease Syndrome. Arch Clin Neuropsychol. 2019 Jun 1;34(4):455-465. doi: 10.1093/arclin/acy051. PMID: 29945190. https://pubmed.ncbi.nlm.nih.gov/29945190/
[ii] Fallon BA, Lipkin RB, Corbera KM, Yu S, Nobler MS, Keilp JG, Petkova E, Lisanby SH, Moeller JR, Slavov I, Van Heertum R, Mensh BD, Sackeim HA. Regional cerebral blood flow and metabolic rate in persistent Lyme encephalopathy. Arch Gen Psychiatry. 2009 May;66(5):554-63. doi: 10.1001/archgenpsychiatry.2009.29. PMID: 19414715. https://pubmed.ncbi.nlm.nih.gov/19414715/
[iii] Coughlin JM, Yang T, Rebman AW, Bechtold KT, Du Y, Mathews WB, Lesniak WG, Mihm EA, Frey SM, Marshall ES, Rosenthal HB, Reekie TA, Kassiou M, Dannals RF, Soloski MJ, Aucott JN, Pomper MG. Imaging glial activation in patients with post-treatment Lyme disease symptoms: a pilot study using [11C]DPA-713 PET. J Neuroinflammation. 2018 Dec 19;15(1):346. doi: 10.1186/s12974-018-1381-4. PMID: 30567544; PMCID: PMC6299943. https://pubmed.ncbi.nlm.nih.gov/30567544/
[iv] Marvel CL, Alm KH, Bhattacharya D, Rebman AW, Bakker A, Morgan OP, et al. (2022) A multimodal neuroimaging study of brain abnormalities and clinical correlates in post treatment Lyme disease. PLoS ONE 17(10): e0271425. https://doi.org/10.1371/journal.pone.0271425
Caption for featured photo: DTI brain images from a 2022 Johns Hopkins University School of Medicine study show white matter changes associated with post treatment Lyme disease.
_________________
**Comment**
What’s important is what will they do with this information and what will they attribute the brain changes to. For instance, currently, and for the entire history of Lyme/MSIDS, these issues have been blamed upon PTLDS – an autoimmune/inflammatory type of condition that will be treated with things like steroids when the very real underlying problem could be persistent infection(s). This has become highly politicalized, causing polarity in research and medicine.
Unfortunately, this article, like so many others before it emphasizes and pushes the accepted narrative about the consequences or supposed failure of prolonged antibiotics for Lyme/MSIDS. Everyone understands that prolonged antibiotic use is not without risks; however, nobody seems to care when it’s for acne, salmonella, endocarditis, sickle cell, or rheumatic fever. Further, this report states there is significant information that supports the safety of prolonged antibiotic use regarding penicillin and its derivatives.
Again it’s about benefit vs risk.
When you are faced with death or a life of misery, all of a sudden the risk of prolonged antibiotics falls on the priority list. Further, many, including myself and my husband have achieved our health back after this therapy.
Of course antibiotics aren’t the only tool in the tool kit needed for treating Lyme/MSIDS. It truly is a complicated illness and one must learn all they can about diet, supplements, herbs, immune modulators, etc., but that doesn’t mean antimicrobials don’t have a very important role.
Lastly, there are good reasons why extended antibiotics haven’t appeared successful in many NIH funded studies. This is because:
typically a monotherapy is utilized, which frankly often isn’t enough with Lyme/MSIDS, plus there’s the concern of antibiotic resistance with this myopic approach
often the wrong antibiotic is used
often the wrong dosage of antibiotic is used
often, individual differences are not taken into account for example, symptoms must be monitored carefully and antibiotics changed when patients hit a plateau. This approach doesn’t fit into the current research paradigm.
many other research design flaws such as only accepting those who test positive on 2-tiered CDC testing which is known to miss more than 70% of all cases, as well accepting patients that have the EM rash which is highly variable
Treat long enough (Bb is slow-growing and persistent)
Make sure blood levels of antibiotics are high enough as people vary. He discusses amoxicillin and how they found that increasingthe dosage to 1,000mg 3X/day and adding probenecid to increase the antibiotic in the blood, people did even better. He goes on to tell of an unpublished study with Stoneybook where there was a failure rate of100% of patients taking 300mg of doxycycline a day for 21 days. Yet, how many people are given this exact treatment?
Cycle treatment. This means, once you are symptom-free for 2-4 months, stop treatment. If symptoms return, treat again. Burrascano has found that it typically takes 3-4 Cycles before a person remains symptom-free. The 3rd cycle often yields the worst herx in his experience.
From the very beginning, treatment failures were seen in virtually every antibiotic study done. The longer the patient follow up, the higher the incidence of treatment failure. The medical community blamed early treatment failures on the older antibiotics erythromycin, tetracycline, and penicillin, and determined that these antibiotics were not very effective at curing Lyme disease. Ignored was the fact that the newer antibiotics were also consistently failing to prevent relapses of active infection. Since these early treatment studies, the concept that two weeks of antibiotic therapy is adequate treatment for Lyme disease has remained ingrained in the medical community’s collective consciousness. [The Long-Term Follow-up of Lyme Disease: A Population-Based Retrospective Cohort Study. Authors: Shadick NA; Phillips CB; Sangha O et al. Ann Intern Med 1999 Dec 21;131(12):919-26]
*Data presented by Dr. Nancy Shadick at an International Lyme Symposia showed that patients in the Nantucket Island study followed for up to 5.2 years after initial antibiotic treatment had ever-climbing relapse rates. Relapse rates in patients receiving two weeks of IV Rocephin (ceftriaxone) could expect a relapse rate to exceed 50% after five years.
There is a smart way to treat this, yet few are nuanced in this skill. We desperately need post-mortem studies to determine what is keeping people ill. We need current transmission studies. We need doctor education on the polymicrobial aspect of this disease. And, we need the stigma & polarization to go away so insurance companies will cover Lyme/MSIDS medical expenses, patients will be believed and supported and the bullying will end.
Prophetic last words: “The stuff I’ve been going through in my brain–ugh”
By Dorothy Kupcha Leland
March 24, 2023
Popular San Francisco radio host Jeffrey “JV” Vandergrift often spoke on the air about his struggles with Lyme disease. On February 23, on what turned out to be his last appearance on his WILD 94.9 radio show, he gave the following alarming update:
“The stuff I’ve been going through in my brain that they’re trying to figure out. Ugh,” he said. He added that doctors told him they believed something might have “reignited old infections.” Then he added, “The body and the pain and all that stuff, I can handle. What it’s doing to my brain I could never describe to you.”
The next day, JV was reported missing from his San Francisco home. Shortly thereafter, his wife Natasha–also a WILD 94.9 radio host–posted the following on social media: “The amount of compassion for the physical torture J has been going through for the past 2 years has been overwhelming. I have been in so much pain and fear and I know all of you have been so scared and concerned for JV as well.” At that time, she said the family had reason to believe that “he will not be coming back.”
Sadly, on March 22, a month after JV disappeared, his body was found in the water near San Francisco’s Pier 39. Here is how his heartbroken colleagues at the WILD 94.9 broke the news to their listeners.
This Sunday, March 26, a screening of the Lyme documentary The Quiet Epidemic will be held at San Francisco’s Roxie Theater. While JV was still missing, the filmmakers had already planned to dedicate this event to JV. At that time, they posted the following on social media:
“JV was a supporter of The Quiet Epidemic and was in touch with our team. It’s incredibly sad that we won’t have a chance to meet him. We hold him and his loved ones in our hearts as we continue pushing our story and cause out into the world. This screening is dedicated to JV, his family, friends, 94.9 family, and listeners.”
I never knew JV and never listened to his show. But I hear elements of his story from countless people throughout the US–in fact throughout the world–who are being held hostage by an insidious disease that has invaded their bodies and brains.
To make matters worse, the medical establishment and government health officials have failed to act on this serious threat to physical and mental health.
In memory of JV and every other person suffering like he did, we must do our best to change this. The time is now.
How to lift brain fog and boost your immune system
2/9/23
By Lonnie Marcum
Both viruses and bacteria can invade the brain. All too frequently, patients with lingering symptoms following infection complain of “brain fog.”
Brain fog describes the feeling of mental confusion, forgetfulness, memory loss, lack of motivation, inability to focus, and/or difficulty concentrating.
A simple technique known as lymphatic drainage massage may help to clear the fog and boost your immune system at the same time.
Patients with brain fog often report “drawing a blank” when trying to remember the name of a friend, family member or pet; forgetting what they were going to do; or getting lost on the way home or to a familiar location. Brain fog can also be associated with symptoms of anxiety and/or depression.
Prolonged brain fog can be caused by a variety of factors, including sleep disturbance, certain medications, head injury, environmental toxins, inflammation and infection—which is the case in many individuals with “Lyme brain.”
Borrelia burgdorferi (Bb), the bacteria that causes Lyme disease, can infect the brain and nervous system. Neurological symptoms of Lyme disease are a late-stage manifestation of Bb infection called neuroborreliosis.
Neuroborreliosis and Lyme Brain
In 2011, researchers at the University of California, Davis were able to show how Bb invades the lymph nodes within 24 hours after infection. They later discovered how it causes abnormalities in the lymph tissues and impairs the immune system.
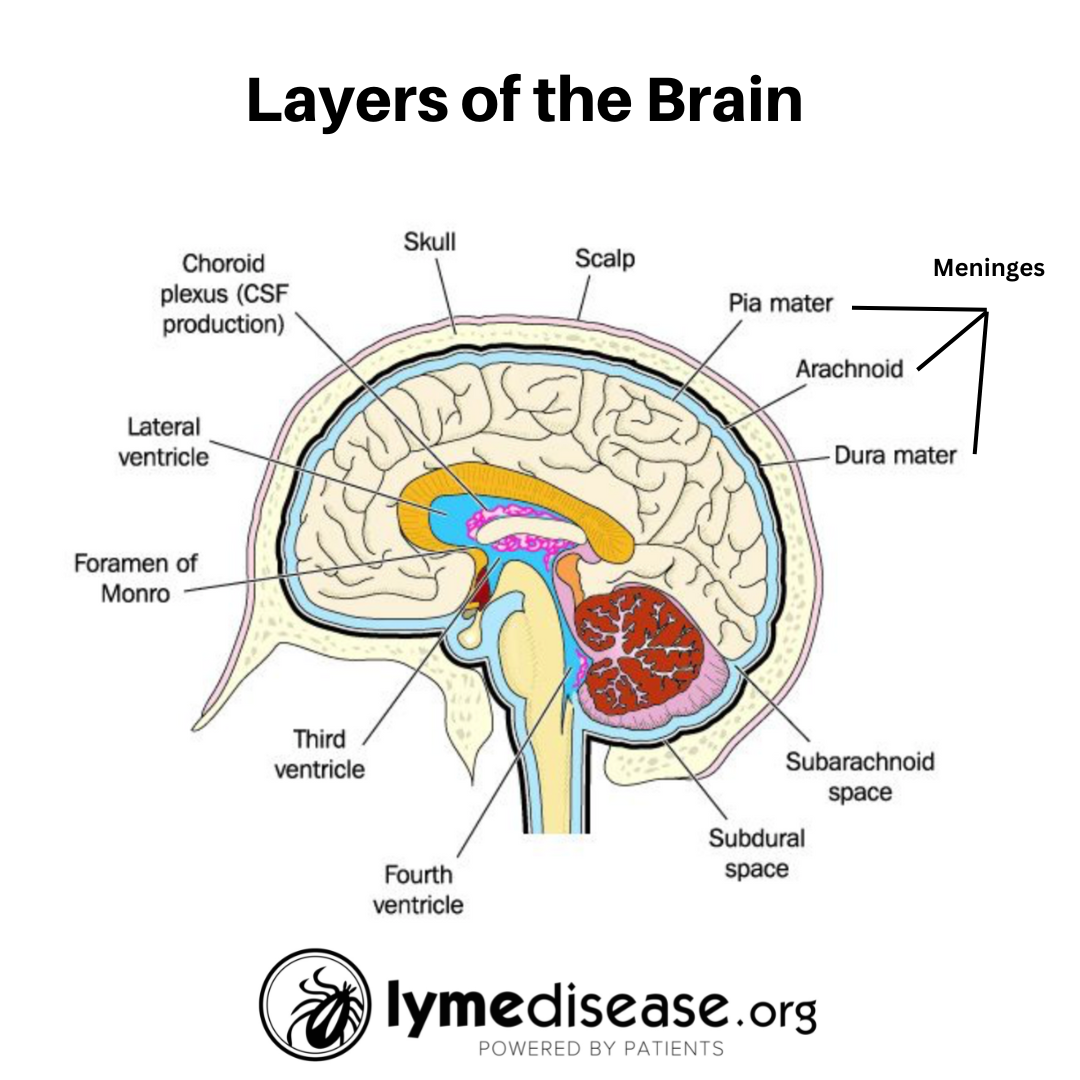
A more recent study suggests that the choroid plexus may play a role in how Borrelia infections affect the nervous system. The choroid plexus is found within the ventricles near the center of the brain. It produces and filters cerebrospinal fluid (CSF), the clear fluid that circulates around the brain and spinal cord.
Another important study from Tulane University found spirochetes that cause Lyme disease in the autopsied brain tissue of a patient who had been aggressively treated with antibiotics. This demonstrated that infection can persist despite antibiotic treatment.
Even if the Borrelia spirochetes don’t completely penetrate the brain, they are frequently present in the meninges. These are three protective layers surrounding the brain and spinal cord. Infection of the meninges is associated with increases in inflammatory cytokines, and meningitis, a swelling of the meninges.
Lyme disease is the most common vector-borne disease in the U.S. and Europe. The spread of Bb to the central nervous system causing Lyme neuroborreliosis occurs in approximately 10–15% of all cases of Lyme disease. In the U.S., one of the most frequent manifestations of Lyme neuroborreliosis is lymphocytic meningitis.
Lyme lymphocytic meningitis is swelling of the meninges with the infiltration of lymphocytes (a type of white blood cell) into the CSF. Symptoms may include fever, headache, neck pain/stiffness, sensitivity to light and cognitive impairment.
Two Circulatory Systems
There are two circulatory systems in our bodies: the cardiovascular system and the lymphatic system.
The cardiovascular system consists of the heart and blood vessels (arteries, veins, capillaries). Basically, arteries carry oxygenated blood and nutrients away from the heart to every tissue in the body, while veins carry used blood back to the heart and lungs in a continuous loop. Capillaries are the small vessels where the arteries and veins connect.
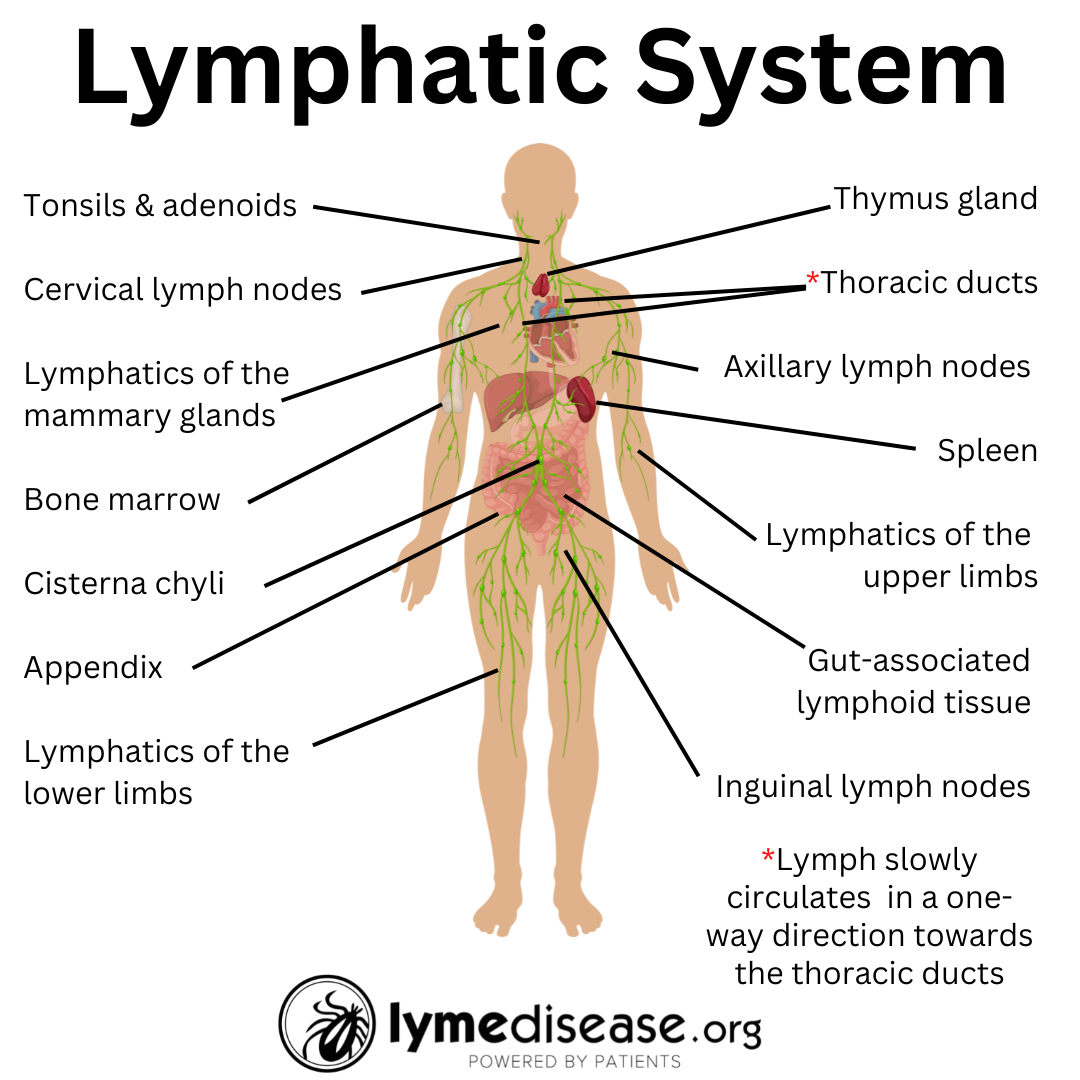
The lymphatic system is a secondary circulatory system. It works separately but in conjunction with the cardiovascular system. When working properly, lymphatics only move in one direction—towards the heart. Included in the lymphatic system are small bean-shaped structures called lymph nodes. Depending on one’s age and sex, there are 400-700 lymph nodes throughout the body with main clusters found in the neck, armpits, chest, abdomen and groin.
T-cells (T-lymphocytes) – play a crucial role in cell-mediated immunity;
B-cells (B-lymphocytes) – produce antibodies that help fight pathogens;
Dendritic cells – present antigens to T-cells, activating the immune system;
Macrophages – engulf and digest foreign matter, cellular debris, and pathogens;
Natural killer cells – attack abnormal (cancerous) or infected cells;
Plasma cells – produce and secrete antibodies.
As bacteria and viruses enter the lymph nodes, the immune cells work to identify and remove them. The more fluid that moves through the lymph nodes, the more immune cells will be produced. From there, the waste is filtered out through the liver and kidneys and the lymph is returned to the blood stream in a continuous cycle.
Unlike the cardiovascular system, which is powered by the heart, the lymphatic system lacks a central pump. Thus, it relies on muscle contractions to circulate lymph. To keep lymph moving through the system, you must drink plenty of water and be active enough to move the fluids through the body.
However, many patients with persistent symptoms of Lyme suffer from chronic fatigue, making activity and traditional exercise nearly impossible—which was the case with my daughter.
When my daughter was immobile due to chronic illness, I used three things to help with lymph drainage: passive range of motion exercises, medical grade compression stockings, and manual lymph drainage massage. These were all things I’d been taught as a physical therapist (PT).
Later we worked with a PT who specialized in chronic fatigue syndrome. She helped my daughter design a full body lymph drainage massage technique she continues to use to this day.
[Note: While you can learn to do all these things on your own, I highly recommend scheduling an appointment with a licensed physical therapist to learn the proper technique for each. PT is covered by most insurance.]
Whether an infection is active, persistent, dormant, or the dead remnants of previous illness, it can produce inflammatory waste products that the body must try to clear through the circulatory system.
Lymphatic drainage massage is a therapeutic technique that uses gentle, rhythmic strokes to stimulate the flow of lymph fluids in a specific direction through the body.
Whole body lymph drainage massage helps reduce inflammation and remove waste products. It also helps stimulate the immune system and allows the movement of basic hormones needed for rest and healing.
Lymphatic drainage massage is similar to deep cleaning your home. It’s like clearing the cobwebs out of the corners and the dust bunnies out from under the bed. When the lymph nodes are plugged, they slow the flow of lymphatic fluid. Leaving those nodes clogged and swollen impairs the healing process.
Never underestimate the value of keeping the lymphatic system functioning.
The Glymphatic System
In the brain, the lymphatic clearance pathway is called the glymphatic system—a pathway that was only recently discovered.
Maiken Nedergaard is a Danish neuroscientist who works at the University of Rochester Medical Center in New York. In 2012, she first identified the existence of the network of lymphatic vessels in the brain that eliminate toxins via cerebrospinal fluid. Prior to this, no one knew how the brain cleared waste and infections. Nedergaard created the word “glymphatic” to represent the relationship between the glial cells and the lymphatic system of the brain.
Nedergaard discovered that the glymphatic system is responsible for removing byproducts of infection, including amyloid beta. It’s a protein that can build up in the brain and is associated with the onset of Alzheimer’s disease.
The glymphatic system is most active during uninterrupted deep sleep. This is one reason why sleep is so important for overall brain health and why sleep deprivation can exacerbate neurodegenerative diseases.
Head/Neck Lymphatic Self-Massage
[Note: If you have any contraindications listed below, please speak to your doctor before performing this procedure.]
When doing lymphatic drainage massage, you always want to start by opening the lymph valves closest to the heart first, work your way outwards, then back in towards the heart. The first time you do this type of massage I recommend going low and slow — maybe 10 – 20 motions of each of the following steps. Later, if no adverse reactions, you can increase to 50 repetitions of each step.
Step 1. From a comfortable seated position, begin by gently pulsing the lymphatic nodes at the base of your neck, the soft space just above the collarbones. These nodes need to be opened before anything can move down from the head/neck.
Step 2. Move your fingers higher up the neck to the groove just behind your ears. With palms flat, pull the skin gently towards the front and all the way down to the center of your neck where it meets the “V” between the collarbones. (P.S. If your sinuses and/or ears pop and you feel like swallowing, you are doing it right.)
Step 3. Make the “Spock” hand sign. Place your middle and index finger behind the ears and the ring and pinky finger in front of the ears and gently pull downwards.
Step 4. Move your hands around the back of the head/neck to the base of the skull and gently pull forward.
Step 5, 6, and 7 is the first three steps in reverse: Perform steps 3, 2 and 1, pulling all the fluid down towards the collarbones.
This is the video I most frequently use to teach people this simple beginner’s self-drainage massage technique.
Watch:
Other Treatments
Ananti-inflammatory diet, full of high quality proteins, fresh fruits/veggies and fiber, and low in processed foods, sugar, gluten and dairy.
Vitamin B, vitamin C andvitamin D are also vital to immune health,
Epsom salt baths or foot soak. The magnesium helps to calm the nerves
Saunas and dry brushing also help with lymphatic drainage,
Movement based upon your tolerance: simple range of motion (moving arms & legs while lying or seated), walking, yoga, swimming, or biking.
Vagus nerve stimulation regulates the immune system through its connections with immune cells in the spleen, thymus and gut-associated lymphoid tissue (GALT),
I always recommend speaking to your treating clinician before beginning a new treatment method. Contraindications to lymphatic massage include acute infection, cardiac edema, cancer, blood clots (DVT), bleeding conditions, kidney failure, bronchitis, uncontrolled high blood pressure.
Resources
Find a Lymphology Certified Specialist through LANA.
Self-help: The Concise Perrin Technique: A Handbook for Patients. By Dr. Raymond Perrin. (A practical companion to The Perrin Technique 2E: How to diagnose and treat CFS/ME and fibromyalgia via the lymphatic drainage of the brain.)
LymeSci is written by Lonnie Marcum, a Licensed Physical Therapist and mother of a daughter with Lyme. She served two terms on a subcommittee of the federal Tick-Borne Disease Working Group. Follow her on Twitter: @LonnieRhea Email her at: lmarcum@lymedisease.org.
References
Adams Y, Clausen AS, Jensen PØ, Lager M, Wilhelmsson P, Henningson AJ, Lindgren PE, Faurholt-Jepsen D, Mens H, Kraiczy P, Kragh KN, Bjarnsholt T, Kjaer A, Lebech AM, Jensen AR. 3D blood-brain barrier-organoids as a model for Lyme neuroborreliosis highlighting genospecies dependent organotropism. iScience. 2022 Dec 19;26(1):105838. doi: 10.1016/j.isci.2022.105838. PMID: 36686395; PMCID: PMC9851883.
Bacyinski A, Xu M, Wang W, Hu J. The Paravascular Pathway for Brain Waste Clearance: Current Understanding, Significance and Controversy. Front Neuroanat. 2017 Nov 7;11:101. doi: 10.3389/fnana.2017.00101. PMID: 29163074; PMCID: PMC5681909.
Bohr T, Hjorth PG, Holst SC, Hrabětová S, Kiviniemi V, Lilius T, Lundgaard I, Mardal KA, Martens EA, Mori Y, Nägerl UV, Nicholson C, Tannenbaum A, Thomas JH, Tithof J, Benveniste H, Iliff JJ, Kelley DH, Nedergaard M. The glymphatic system: Current understanding and modeling. iScience. 2022 Aug 20;25(9):104987. doi: 10.1016/j.isci.2022.104987. PMID: 36093063; PMCID: PMC9460186.
Chikly, Bruno (2004). Silent Waves: Theory and Practice of Lymph Drainage Therapy: An Osteopathic Lympathic Technique. I.H.H. Pub. ISBN978-0-9700-5302-2.
Chikly BJ. Manual techniques addressing the lymphatic system: origins and development. J Am Osteopath Assoc. 2005 Oct;105(10):457-64. PMID: 16314678.
Elsner RA, Hastey CJ, Olsen KJ, Baumgarth N (2015) Suppression of Long-Lived Humoral Immunity Following Borrelia burgdorferi Infection. PLoS Pathog 11(7): e1004976. doi:10.1371/ journal.ppat.1004976
H Heald A, Perrin R, Walther A, Stedman M, Hann M, Mukherjee A, Riste L. Reducing fatigue-related symptoms in Long COVID-19: a preliminary report of a lymphatic drainage intervention. Cardiovasc Endocrinol Metab. 2022 Apr 12;11(2):e0261. doi: 10.1097/XCE.0000000000000261. PMID: 35441129; PMCID: PMC9010124.
Lotz SK, Blackhurst BM, Reagin KL, Funk KE. Microbial Infections Are a Risk Factor for Neurodegenerative Diseases. Front Cell Neurosci. 2021 Jul 7;15:691136. doi: 10.3389/fncel.2021.691136. PMID: 34305533; PMCID: PMC8292681.
Parthasarathy G, Pattison MB, Midkiff CC. The FGF/FGFR system in the microglial neuroinflammation with Borrelia burgdorferi: likely intersectionality with other neurological conditions. J Neuroinflammation. 2023 Jan 17;20(1):10. doi: 10.1186/s12974-022-02681-x. PMID: 36650549; PMCID: PMC9847051.
Sachdeva S, Persaud S, Patel M, Popard P, Colverson A, Doré S. Effects of Sound Interventions on the Permeability of the Blood–Brain Barrier and Meningeal Lymphatic Clearance. Brain Sciences. 2022; 12(6):742. https://doi.org/10.3390/brainsci12060742
Thompson D, Brissette CA, Watt JA. The choroid plexus and its role in the pathogenesis of neurological infections. Fluids Barriers CNS. 2022 Sep 10;19(1):75. doi: 10.1186/s12987-022-00372-6. PMID: 36088417; PMCID: PMC9463972.
Tunev SS, Hastey CJ, Hodzic E, Feng S, Barthold SW, Baumgarth N. Lymphoadenopathy during lyme borreliosis is caused by spirochete migration-induced specific B cell activation. PLoS Pathog. 2011 May;7(5):e1002066. doi: 10.1371/journal.ppat.1002066. Epub 2011 May 26. PMID: 21637808; PMCID: PMC3102705.
Unvaccinated patients have mentioned half-jokingly that COVID-19 vaccination in friends and family makes some of them “crazy.” While I have always brushed this off as fear driven vaccine ideology taking over common sense in some zealots, the building literature on neuropsychiatric symptoms is alarming. There are now ~10 papers describing headache, fever, and a range of acute neuropsychiatric symptoms after both mRNA and adenoviral COVID-19 vaccination. The strong bias among editors and publishers has kept countless papers out of the mainstream medical media, hence one has to look far and wide to find information on the topic of vaccine safety. Borovina et al, from Croatia described three cases of acute headache followed by psychosis. (See link for article and study)
_______________
Important excerpt:
One of the cases progressed to attempted suicide with a knife stabbing to the abdomen requiring emergency abdominal surgery.
As a doctor I am disturbed by medical evidence demonstrating gene coded SARS-CoV-2 Wuhan Institute of Virology Spike protein in the human brain after vaccination. I wonderhow many subtle changes go clinically unrecognized.
McCullough rightly states that every suicide after Dec. 2020 should be investigated and the brand, doses, and dates of “vaccination” should be recorded and noted. Unfortunately, none of this will happen. It’s all #ABV (anything but the vaccine).
Moderna Booster Vaccine Singled Out for Chronic Hives
— Chronic spontaneous urticaria more frequent when compared with Pfizer’s mRNA vaccine
by Elizabeth Short, Staff Writer, MedPage Today February 1, 2023
The monovalent Moderna COVID-19 booster vaccine may be associated with an elevated risk for new-onset chronic spontaneous urticaria (CSU), or hives lasting more than 6 weeks, according to a Swiss study.
Among people who got an mRNA COVID vaccine booster and had new-onset hives reported to local allergists, 90% had vaccination precede CSU in the canton of Vaud during the study period, as did 81% of patients in the nationwide cohort, reported Yannick Daniel Muller, MD, PhD, of the University of Lausanne in Switzerland, and coauthors. (See link for article)
_______________
**Comment**
Predictably, the authors still want everyone to get “vaccinated,” and take the safe route by stating more research is needed. They state that Moderna shots contain higher doses of mRNA and are more immunogenic than Pfizer shots, although both are clearly linked to a multitude of adverse events and death. The Vaccine advisory committee unanimously endorsed the FDA’s plan to harmonize the primary and booster shots to contain a bivalent composition with components targeting BA.4/5 and the original SARS-CoV-2 strain, eliminating the original monovalent products. Both are deplorable and useless.
The study points out the risk of trying to alter the pathogen’s genetic code
The study found that the medication molnupiravir (Lagevrio) is giving rise to new mutations in some patients which has some researchers worried the drug may create more contagious or dangerous variations of COVID
One author of the study states the drug should be discontinued due to the risks
No Testing Required to Get Paxlovid & Molnupiravir/Lagevrio, Even Though They Are Dangerous
But in a slick move, the FDA has removed COVID testing requirements to make it even easier to obtain Pfizer (Paxlovid) and Merck (Molnupiravir/Lagevrio) COVID treatments. Now, exposed individuals with signs and symptoms (that look like any other flu-bug), can simply waltz into their doctor’s office and be diagnosed with COVID, even if they have a negative test result: however, they stillcan not obtain cheap, safe, effective drugs like ivermectin, HCQ, or even vitamin C.
And low and behold, a new study finds that ivermectin is a promising cancer drug.
Ivermectin is a widely used antiparasitic drug and shows promising anticancer activity in various cancer types. Although multiple signaling pathways modulated by ivermectin have been identified in tumor cells, few studies have focused on the exact target of ivermectin. Herein, we report the pharmacological effects and targets of ivermectin in prostate cancer. Ivermectin caused G0/G1 cell cycle arrest, induced cell apoptosis and DNA damage, and decreased androgen receptor (AR) signaling in prostate cancer cells. Further in vivo analysis showed ivermectin could suppress 22RV1 xenograft progression. Using integrated omics profiling, including RNA-seq and thermal proteome profiling, the forkhead box protein A1 (FOXA1) and non-homologous end joining (NHEJ) repair executer Ku70/Ku80 were strongly suggested as direct targets of ivermectin in prostate cancer. The interaction of ivermectin and FOXA1 reduced the chromatin accessibility of AR signaling and the G0/G1 cell cycle regulator E2F1, leading to cell proliferation inhibition. The interaction of ivermectin and Ku70/Ku80 impaired the NHEJ repair ability. Cooperating with the downregulation of homologous recombination repair ability after AR signaling inhibition, ivermectin increased intracellular DNA double-strand breaks and finally triggered cell death. Our findings demonstrate the anticancer effect of ivermectin in prostate cancer, indicating that its use may be a new therapeutic approach for prostate cancer.
Well now, ‘the powers that be’ simply can not have this.
Better censor and ban it off the face of the earth.