Kerry teacher Karin O’Shea needs urgent treatment for chronic Lyme disease after being misdiagnosed for 12 years
By Aoife Breslin
Feb. 14, 2022
With only one option left, housebound Kerry woman Karin O’Shea must go to Germany in order to receive urgent treatment for Chronic Lyme disease after believing her diagnosis to be Fibromyalgia for 12 years
Kerry woman Karin O’Shea contracted Lyme disease from the bite of a tick when she was a teenager and went undiagnosed for 12 years.
Now, she needs urgent treatment.
When Karin became ill in her teens, she was misdiagnosed with Fibromyalgia. She was able to manage her symptoms through medication and lived a normal life.
In 2020, the 26-year-old saw a rapid deterioration in her health. After endless GP visits, countless consultants, MRI’s, X-rays and hospital admissions, there were no answers.
Speaking with RSVP Live, Karin shared her experience:
“Me and my GP extended every avenue but there were still no answers.
“So, I had to send my bloods to Germany myself to test for Lyme disease and the results came back positive, as well as showing chronic immune suppression.”
Karin was tested for Lyme disease under the Irish system when she was 14 years old, but her results came back negative.
This was due to her chronic immune suppression; her body wasn’t creating enough antibodies and the Irish system detects antibodies in order to get results. (See link for article and video)
__________________
**Comment**
Another heart-breaking story of misdiagnosis which has caused yet another case to fester and worsen.
SUMMARY:
O Shea finally obtained appropriate treatment which included 5 antibiotics a day.
Due to her late stage case, she had horrific side-effects, and her body rejected the treatment.
Patient is now housebound due to severe neurological symptoms.
Her remaining option is to travel to Germany for a month of intensive treatment followed by a 6 months of rehabilitation.
She’s been told she has a 70% chance of obtaining remission and should get quality of life back.
O Shea’s advice to others:
“I want people to know if you do get a tick bite, go straight to the doctor and demand two weeks antibiotics, regardless of if you have the bulls-eye rash or not.
I couldn’t agree more, but I’d demand a month’s worth.
She also states that she was untreated because she never got the EM rash. She then states that only 50% get the rash, but it can actually be far less than that, is highly variable, and should never be used to keep people from being diagnosed. While the EM rash IS DIAGNOSTIC for Lyme, not having it means nothing.
The article doesn’t mention co-infections which are almost always an issue with chronic patients and require other medications. They also make cases much more severe. My educated guess is she’s going to St. George Hospital where she will be treated with hypothermia and IV antibiotics, among other modalities. Here’s the story of a woman who got this treatment. I also write about the treatment in the comment section as well as questions I posed to Dr. Douwes, head of St. George Hospital, when he spoke at an ILADS convention.
If you want to support Karin on her journey to recovery click here.
True to form, the day after this information about ivermectin is disseminated, Medpage Today comes out with yetanother trash piece on ivermectin. Mainstream media is also guilty. Rather than discussing solid data, science, and the fact it has worked even on the most severe cases, the article focuses on a singular doctor on twitter who states FLCCC’s therapies for Long COVID is like “throwing spaghetti against the wall,” as well as, “Throwing 20 medications (9 are prescription) at a problem with minimal (or no) evidence is irresponsible. As we will see, this is both unethical & likely harmful.” ~Nick Mark, MD
Lyme/MSIDS patients and Lyme literate doctors take note of this attack because the same thing has been said about effective treatments for tick-borne illness due to the fact pathogens cause severe immune dysfunction and can affect every organ in the human body – similarly to COVID. FLCCC has figured this out and is addressing multiple issues the body is contending with when infected with COVID.
Ivermectin Beats Out 9 Other Meds for Treating Omicron, Study Confirms
Researchers used computational analyses to evaluate the performance of 10 medications against the Omicron variant, finding ivermectin outperformed all of them, including nirmatrelvir (Paxlovid), a new drug from Pfizer that has cost taxpayers $5.29 billion and costs $529 per course of treatment.
Researchers used computational analyses to evaluate the performance of 10 medications against the Omicron variant, finding that ivermectin outperformed all of them, including nirmatrelvir (Paxlovid) a new drug from Pfizer that has cost taxpayers $5.29 billion and costs $529 per course of treatment.
Ivermectin lowers the viral load by inhibiting replication, reduces infection by 86% when used preventively, speeds recovery, protects against organ damage, lowers the risk of hospitalization and death and costs between $48 and $95 for a course of treatment depending on your location.
Early treatment lowers your risk of long COVID, which includes physical and mental health conditions. According to cardiologist Dr. Peter McCullough, 50% of those sick enough to be hospitalized have symptoms of long COVID.
Africa has a lower number of cases, severity of disease, hospitalizations and deaths than other areas of the world, which may be due to using prophylactic medications for endemic infections that have successfully treated COVID.
At nearly no other time in history has there been this level of fear generated across the world as experienced thus far in 2020 and 2021. The depth and breadth of the strategies used to stoke those fears have been overwhelming.
Unfortunately, many of the early effective treatment strategies that can be used at home have also fallen victim to censorship.Ivermectin is one of those strategies. In a computational analysis of the Omicron variant against several therapeutic agents, data show that ivermectin had the best results.
Yet, as you look objectively at what’s been happening across the world, the fear being generated is not one-sided. The suppression of information by corporations, government agencies and the pharmaceutical industry is one indication of their concern and how far they’re willing to go to ensure the level of fear remains high enough to manipulate behavior.
Consider the statistics from the Centers for Disease Control and Prevention. In 2019, 4.6% of the U.S. population was diagnosed with heart disease. The population at the end of 2019 was 328,239,523.
This means there were 15,099,018 people with heart disease in the U.S. in 2019. There were 696,962 people who died that year from heart disease, which is a death rate of 4.6%.
This is 20 times greater than the death rate from COVID-19. Yet these same agencies were not lobbying for mandates against soda or sugar-laden foods — they weren’t banning smoking and they weren’t mandating exercise — all heart disease risk factors.
The censorship and suppression of information has hobbled early treatment of COVID-19 in many western nations. Through 2020, public healthexperts and the mainstreammedia warned against the use of hydroxychloroquine and ivermectin.
Both are on the World Health Organization’s list of essential drugs, but the benefits have been ignored by public health officials and buried by the media.
Newest ivermectin study showed best results against COVID
This study on Cornell University’s preprint website has not yet been peer-reviewed. Researchers used a computational analysis to look at the Omicron variant, which has demonstrated a lower clinical presentation and lower hospital admission rates.
After having retrieved the complete genome sequence and collecting 30 variants from the database, the researchers analyzed 10 drugs against the virus, including:
Binding energy of promising drugs against main protease of Omicron variant.
The researchers found that each of the drugs had some degree of effectiveness against the virus and most were currently in clinical trials. They used molecular docking to find that the mutations in the Omicron variant didn’t significantly affect the interaction between the drugs and the main protease.
An analysis of all 10 drugs found that ivermectin was the most effective drug candidate against the Omicron variant. The testing included Nirmatrelvir (Paxlovid), which is the new protease inhibitor for which the U.S. Food and Drug Administration (FDA) provided an emergency use authorization against COVID in December 2021.
In other words, Pfizer released a new drug which cost the U.S. taxpayers $5.29 billion or $529 per course of treatment and which received an EUA despite the availability of a similar drug that has proven to be more effective and is cheaper.
How ivermectin works
Ivermectin is best known for its antiparasitic properties. Yet, the drug also has antiviral and anti-inflammatory properties. Studies have shown that ivermectin helps to lower the viral load by inhibiting replication.
A single dose of ivermectin can kill 99.8% of the virus within 48 hours.
A meta-analysis in the American Journal of Therapeutics showed the drug reduced infection by an average of 86% when used preventively. An observational study in Bangladesh evaluated the effectiveness of ivermectin as a prophylaxis for COVID-19 in health care workers.
The data showed four of the 58 volunteers who took 12 mg of ivermectin once a month for four months developed mild COVID symptoms as compared to 44 of the 60 health care workers who declined the medication.
Ivermectin has also been shown to speed recovery, in part by inhibiting inflammation and protecting against organ damage. This pathway also lowers the risk of hospitalization and death. Meta analyses have shown an average reduction in mortality that ranges from 75%to83%.
Additionally, the drug also prevents transmission of SARS-CoV-2 when taken before or after exposure. Added together, these benefits make it clear that ivermectin could all but eliminate this pandemic.
Early intervention lowers long COVID and hospitalization
Some people who have had COVID-19 seem to be unable to fully recover and complain of lingering symptoms of chronic fatigue. Others struggle with mental health problems.
One study, in November 2020, found 18.1% of people who had COVID-19 received their first psychiatric diagnosis in the 14 to 90 days after recovery. Most commonly diagnosed conditions were anxiety disorders, insomnia and dementia.
These symptoms have come to be called long COVID, long-haul COVID, post-COVID syndrome, chronic COVID or long-haul syndrome. They all refer to symptoms that persist for four more weeks after an initial COVID-19 infection.
According to Dr. Peter McCullough (5:43), board-certified internist and cardiologist, 50% of those who have been sick enough to be hospitalized will have symptoms of long COVID:
“So, the sicker someone is, and the longer the duration of COVID, the more likely they are to have long COVID syndrome. That’s the reason why we like early treatment. We shorten the duration of symptoms and there’s less of a chance for long COVID syndrome.”
Some of the common symptoms of long COVID include shortness of breath, joint pain, memory, concentration or sleeping problems, muscle pain or headache and loss of smell or taste.
According to McCullough (6:05), a paper presented by Dr. Bruce Patterson at the International COVID Summit in Rome, Sept. 11 to 14, 2021:
“… showed that in individuals who’ve had significant COVID illness, 15 months later the s1 segment of the spike protein is recoverable from human monocytes. That means the body literally has been sprayed with the virus and it spends 15 months, in a sense, trying to clean out the spike protein from our tissues. No wonder people have long COVID syndrome.”
It should come as no surprise that studies have also confirmed that early intervention improves mortality and reduces hospitalizations. Perhaps one of the greatest crimes in this whole pandemic is the refusal by reigning health authorities to issue early treatment guidance.
Instead, they’ve done everything possible to suppress remedies shown to work. Patients were simply told to stay home and do nothing. Once the infection had worsened to the point of near-death, patients were told to go to the hospital, where most were routinely placed on mechanical ventilation — a practice that was quickly discovered to be lethal.
However, as the featured study and others have demonstrated, ivermectin is one of the successful treatment protocols that can be used against SARS-CoV-2.
Africa has lowest case and death rate, likely from ivermectin
Across the world, countries have taken different approaches to address the spread of the virus. The steps taken in Africa varied depending on the country, yet the infection and death rates were relatively stable and low across the continent.
In the last year there have been reports of small areas in the world where the number of infections, deaths or case-fatality rates have been significantly lower than the rest of the world. For example, India’s Uttar Pradesh State reported a recovery rate of 98.6% and no further infections.
However, the entire continent of Africa appears to have sidestepped the massive number of infections and deaths predicted for these poorly funded countries with overcrowded cities. Early estimations were that millions would die, but that scenario has not materialized.
The World Health Organization has called Africa “one of the least affected regions in the world.”
There are several factors that may influence the infection rate in Africa. A study from Japan (1.25) demonstrates that after just 12 days that doctors were allowed to legally prescribe ivermectin to their patients, the cases dropped dramatically.
The chairman of the Tokyo Medical Association had noticed the low number of infections and deaths in Africa, where many use ivermectin prophylactically and as the core strategy to treat onchocerciasis, a parasitic disease also known as river blindness.
More than 99% of people infected with river blindness live in 31 African countries.
In addition to ivermectin use in Africa, other medications are also commonly available, such as hydroxychloroquine and chloroquine, which have long been used in the treatment and prevention of malaria, also endemic in Africa.
Finally, Artemisia annua, also known as sweet wormwood, is an herb used in combination therapies to treat malaria. It was used in traditional Chinese medicine for more than 2,000 years to treat fever.
Today artemisinin, a metabolite of Artemisia, is the current therapeutic option for malaria. The plant has also been studied since the 2003 SARS outbreak for the treatment of coronaviruses, with good results.
In other words, whether by design or default, the medications that have proven to be successful against the virus are commonly used in Africa for other health conditions.
While Pfizer tests the short- and long-term effects of a genetic experiment on Israel’s population, it appears one continent has demonstrated administration of a 30-year-old, inexpensive drug with a known safety profile could reduce the cases, severity and mortality from this infection.
The question that must be asked and answered to get to the bottom of this plandemic is what is blinding mainstream media, government agencies, public health experts, medical associations, doctors, nurses and your next-door neighbor from recognizing and speaking out in support of science?
Dr. Robert Califf, head of FDA under the Obama administration, is back as head of the FDA. Under his watch, he helped Big Pharma reap in record profits and sales and shielded them from any liability due to the opioid crisis. An FDA exec was taped by Project Veritas proving that the FDA is utterly controlled by Big Pharma. The fraud, collusion, and conflicts of interests are all exposed, plain as day, yet the lawlessness continues.
It’s gotten so bad, state attorney generals have had to call out the FDA, CDC, Fauci, and the media for ‘fueling confusion and misinformation’ by interfering with the treatment of COVID patients. Both Nebraska and Oklahoma doctors are now free to prescribe off-label medications such as ivermectin and HCQ for COVID without fear of disciplinary action from corrupt groups like the AMA and state medical boards.
This legal action needs to happen in each and every state in the U.S.
What you are about to read will make perfect sense when you know that two high-level regulatory officials with the FDA involved in vaccine oversight accepted jobs at Moderna just months after signing off on the licensure of the company’s COVID-19 vaccine, according to a British Medical Journal (BMJ) investigation. This is not the first time issues have been raised with the FDA’s “revolving door”—a concept defined in an October 2005 paper by the Revolving Door Working Group (RDWG) as the “movement of individuals back and forth between the private sector and the public sector.”
FDA Exec on Camera Reveals Future COVID Policy “Biden Wants To Inoculate As Many People As Possible”
FDA Executive Officer, Christopher Cole:
“You’ll have to get an annual shot [COVID vaccine]. I mean, it hasn’t been formally announced yet ‘cause they don’t want to, like, rile everyone up.”
Cole on President Joe Biden: “Biden wants to inoculate as many people as possible.”
Cole on plans to approve vaccine for toddlers: “They’re not going to not approve [emergency use authorization for children five years old or less].”
Cole on pharmaceutical companies: “There’s a money incentive for Pfizer and the drug companies to promote additional vaccinations.”
Cole on the financial incentive for pharmaceutical companies: “It’ll be recurring fountain of revenue. It might not be that much initially, but it’ll be recurring — if they can — if they can get every person required at an annual vaccine, that is a recurring return of money going into their company.”
FDA Official Statement: “The person purportedly in the video does not work on vaccine matters and does not represent the views of the FDA.”
[WASHINGTON, D.C. – Feb. 15, 2022] Food and Drug Administration [FDA] Executive Officer, Christopher Cole, inadvertently revealed that his agency will eventually announce that annual COVID-19 vaccinations will become policy.
Cole is an Executive Officer heading up the agency’s Countermeasures Initiatives, which plays a critical role in ensuring that drugs, vaccines, and other measures to counter infectious diseases and viruses are safe. He made the revelations on a hidden camera to an undercover Project Veritas reporter.
Cole indicates that annual COVID-19 shots isn’t probable — but certain. When pushed on how he knows an annual shot will become policy, Cole states, “Just from everything I’ve heard, they [FDA] are not going to not approve it.”
The footage, which is part one of a two-part series on the FDA, also contains soundbites from Cole about the financial incentives pharmaceutical companies like Pfizer have to get the vaccine approved for annual usage. “It’ll be recurring fountain of revenue,” Cole said in the hidden camera footage. “It might not be that much initially, but it’ll recurring — if they can — if they can get every person required at an annual vaccine, that is a recurring return of money going into their company.”
Perhaps the most explosive part of the footage is the moment where Cole brazenly talks about the impact that an Emergency Use Authorization has on overcoming the regulatory concerns of mandating vaccines on children.
“They’re all approved under an emergency just because it’s not as impactful as some of the other approvals,” Cole said when asked if he thought there was “really an emergency for kids.”
Cole, who claims his role with the FDA is to ensure the agency uses a framework of safety, security, and effectiveness as a part of its preparedness and response protocol, specifically cited concerns over “long term effects, especially with someone younger.”
FDA Executive Officer Exposes Close Ties Between Agency and Pharmaceutical Companies:
‘Almost a Billion Dollars a Year Going into FDA’s Budget from the People we Regulate’
• FDA Executive Officer Chris Cole: “The drug companies, the food companies, the vaccine companies. So, they pay us hundreds of millions of dollars a year to hire and keep the reviewers to approve their products.”
• Cole on FDA fees: “Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers which will speed up the approval process. So, they [pharmaceutical companies] make more money.”
• Cole: “They [FDA] tone down the impact of the user fees on their operations because they know they’re dependent on the drug companies, and the vaccine companies, and these other companies for their agency to operate.”
• Cole on blowing the whistle: “There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it.”
• Cole on retaliation in government: “You’ll be marked from getting other jobs because another office is not going to want to hire you if you’ve spoken out about something, right or wrong. They don’t look at what you’ve spoken out about. They’re just not willing to- government’s about rocking the boat and they don’t want to- which is the problem I have with- one of the problems I have with government is, like, they don’t like people rocking the boat, for right or wrong, at all costs. They want to hire a safe person that can do the job but doesn’t necessarily- is a great hire.”
[WASHINGTON, D.C. – Feb. 16, 2022] Project Veritas published Part Two of its series on the FDA on Wednesday night which featured FDA Executive Officer, Christopher Cole, speaking about the inner workings of the agency including the FDA’s conflicts of interest, overspending, and why it’s hard for those within the agency to speak out on such abuses.
In the footage, Cole talks about the impact that pharmaceutical companies have on the agency including the process for approving drugs.
“A long time ago, Congress approved user fees for [the] FDA. Basically, we charge the industry millions of dollars in order to hire more drug reviewers and vaccine reviewers, which will speed up the approval process, so they make more money,” Cole says in the hidden camera footage.
He then reveals that the FDA tones down the impact that these user fees have on the agency’s operations because, “they’re dependent on the drug companies, and the vaccine companies and these other companies for their agency to operate.”
The incendiary footage, which features Cole talking about how the additional money the FDA brings in “gets banked” to be spent on “whatever you can, whether it’s right or wrong,’’ also features Cole discussing reasons why it’s difficult for anyone in government to speak out about practices he sees as “probably excessive.”
“I don’t think there’s enough people saying — they’re, like, ‘Look, that’s fine, but that’s not right. So, we’re not going to charge that.’ You don’t want to be that person. You’re not going to have a long shelf life in the agency if you’re always that person,” Cole said.
“There’s not an incentive to speak out in government, surprisingly. You would think there would be, but there’s not. It’s better just to just not say anything and just ignore it. The whistleblower, well, it’s high-profile whistleblower statutes and everything, that’s kind of ridiculous,” Cole said before adding “it’s better to just stay quiet and accept.”
Cole’s LinkedIn page lists him as an Executive Officer within the agency’s Countermeasures Initiatives, which plays a critical role in ensuring that drugs, vaccines, and other measures to counter infectious diseases and viruses are safe. He made these revelations on a hidden camera to an undercover Project Veritas reporter.
A spokesperson for FDA issued a statement yesterday saying, “The person purportedly in the video does not work on vaccine matters and does not represent the views of the FDA.”
This statement appears to contradict a phone call released Wednesday afternoon by Project Veritas wherein Cole reiterated, during the conversation with Project Veritas Founder and CEO, James O’Keefe, that he is “a manager in the office that helps oversee the approval of the COVID vaccines for emergency approval.”
Please see below in the link that indeed, Dr. Robert Califf was voted in to head the FDA. We can only expect the corruption to continue under his reign.
Apparently Robert Califf did such a good job of helping Big Pharma shield themselves from any liabilities due to the opioid crisis that destroyed the lives of so many Americans while he was head of the FDA under President Obama, that he is being brought back to lead the FDA again to help Big Pharma continue growing in record profits and sales as they get ready to expand the market for the COVID-19 gene-altering shots by having Americans get vaccinated every year, along with the already profitable flu shots.
While he was approved to lead the FDA by the Senate in an overwhelming vote of support with an 89-4 Senate vote on his confirmation in 2016, this time around he barely survived the confirmation vote which was 50-46, facing bi-partisan opposition to his confirmation.
Senators Joe Manchin and Republican Senator Mike Braun from Indiana paired up to write an op-ed piece published at USA Today to voice their opposition to Califf’s confirmation as head of the FDA.
Since OxyContin was approved by the Food and Drug Administration in 1995, more than 500,000 Americans have died from overdoses related to opioids and synthetic opioids.
Nearly three decades later, more than 101,000 Americans – over 1,500 West Virginians and nearly 2,500 Hoosiers – died between June 2020 and June 2021. It’s clear that not much has changed in the way the FDA approves and manages these highly addictive, destructive drugs killing Americans at an astonishing rate.
In fact, it has become increasingly clear that the FDA has stood by, and even enabled, the pharmaceutical industry’s decision to choose profits over American lives.
High overdose rates, not enough treatment facilities
Many families across the United States have been impacted by the drug epidemic that continues to ravage our nation. In our beloved states of West Virginia and Indiana, our communities continue to face disproportionately high overdose rates, with not nearly enough treatment facilities to care for our neighbors in need.
However, instead of reining in opioid prescribing, the agency in charge of regulating these substances continues to approve even more deadly opioids. It is crystal clear that the FDA has not done enough to address the drug epidemic ravaging our nation.
Given the dire situation facing our communities, it makes absolutely no sense to install a candidate who has already led the FDA in its most senior position but failed to address this crisis in any meaningful way.
A poor record on opioids
The current FDA commissioner nominee, Dr. Robert Califf, has significant ties to the pharmaceutical industry, and his leadership of the FDA would take us backward, not forward. His nomination is an insult to the many families and individuals who have had their lives changed forever as a result of addiction.
During Dr. Califf’s previous tenure as FDA commissioner, drug-related overdoses went up, a clear indicator the FDA hadn’t made any necessary, meaningful changes to address the crisis facing our country. In 2016, then-Commissioner Califf announced the FDA’s plan to overhaul its opioid policies.
Reports have also indicated that Dr. Califf intends to keep Dr. Janet Woodcock on board as a senior adviser if confirmed to lead the FDA. During her tenure at the FDA, Dr. Woodcock has directly overseen the approval of numerous highly addictive drugs to market.
She also decided to ignore the advice of an FDA advisory committee when she chose to approve Zohydro, a questionable pure hydrocodone drug with strong risk of overdose and death.
The pharmaceutical industry has benefitted from the status quo at the FDA under the leadership of Dr. Califf and Dr. Woodcock, and the American people have suffered for it. (Full article.)
Lyme and Babesia–a potent combination that’s frequently missed
By Wendy Adams, Bay Area Lyme Foundation
Unless you’ve been living under a rock for the last few years, you’ll have learned that tick-borne diseases are on the rise across the United States.
Many theories exist as to why this is the case. However, most scientists that study ticks and their habitats agree that a combination of reasons—including climate change and human encroachment into tick habitats—are at least partially to blame.
Although Lyme disease (caused by the bacterium Borrelia burgdorferi) is the most common disease that humans acquire from tick bites, ticks can unfortunately transmit several other bacteria, viruses, and parasites to humans.
Multiple infections can even be transmitted during the same bite. The confusing and overlapping disease symptoms caused by multiple infections makes it extremely difficult for doctors to recognize, diagnose and treat the different infections.
Borrelia burgdorferi and Babesia
The most commonly reported tick-borne disease after Lyme disease is babesiosis, caused by infection with the parasite Babesia. This parasite, just like its cousin, Plasmodium falciparum (malaria), infects red blood cells and can cause anemia, thrombocytopenia (low platelets) and other serious, sometimes life-threatening symptoms.
Babesia microti, the most common infectious parasite in the US, is typically found where Lyme disease is found—the Northeast, Mid-Atlantic, and Midwest, although most reported cases come from the Northeast.
But why the overlap in this geography with Lyme disease? It turns out that the presence of B. burgdorferi in an ecosystem facilitates the establishment of B. microti in ticks.
Co-infections likely
This means that ticks in locations infected with Babesia are also more likely to be co-infected with B. burgdorferi. At least one study in mice co-infected with Babesia and Borrelia showed that Babesia hindered the acquired immune response, including B and T cell production, such that Borrelia (Lyme) symptoms were enhanced.
Notably, Borrelia can affect the innate immune system—meaning that a co-infected individual might not be able to mount a sufficient immune response at either stage to fight either pathogen optimally.
Babesia is of special concern to doctors and scientists for a few reasons. Like Borrelia, the parasite can be transmitted by an infected mother across the placenta to an unborn child. The resulting infection can be dangerous in a newborn and has been documented in a case where the pregnant mother was not tested for babesiosis despite a Lyme diagnosis.
Another reason Babesia is concerning is its invasion of the blood supply. Babesia can survive blood banking conditions and hundreds of cases have been documented through blood transfusions.
Infected organ transplantation has also led to Babesia transmission and infection by this route is especially problematic. Transplant patients must take immunosuppressants in order not to reject the new organ, leaving them even more susceptible to opportunistic infections.
Babesia duncani—“Left Coast” Babesia?
As noted earlier, Babesia is a specific family or “genus” of pathogens and there are different species within the genus in different regions of North America.
The West Coast of the US has at least one species which infects humans: Babesia duncani (Babesia divergens has also been found in Washington state).
B. duncani doesn’t seem to be closely related to B. microti. Rather, it is more closely related to Babesia gibsoni, a species found in canines, and a parasite called Theileria.
Although there are very few reported cases of B. duncani, some research suggests that it has been found in human infections in other North American locales as well and there are transfusion-associated cases in the literature.
Interestingly, the strains from California—while looking the same under the microscope—differ in genetic sequence from other known Babesia strains (notably, a strain called WA1) on the West Coast. Therefore, there is significant genetic diversity even within the same B. duncani species.
Seroprevalence studies (which measure antibodies from a large population of blood serum samples) done in the 1990s showed that 3% of people in a Lyme-endemic community in Mendocino county had antibodies, and 16% of soldiers stationed at Fort Ord in Monterey county had antibodies to B. duncani.
Yet, strangely, despite the overlap in regionality of B. duncani and Lyme Borrelia in California, Oregon and Washington, B. duncani has not been found in Ixodes pacificus (western blacklegged) ticks. These are the ticks that harbor and transmit B. burgdorferi in the western US.
Found in a different tick
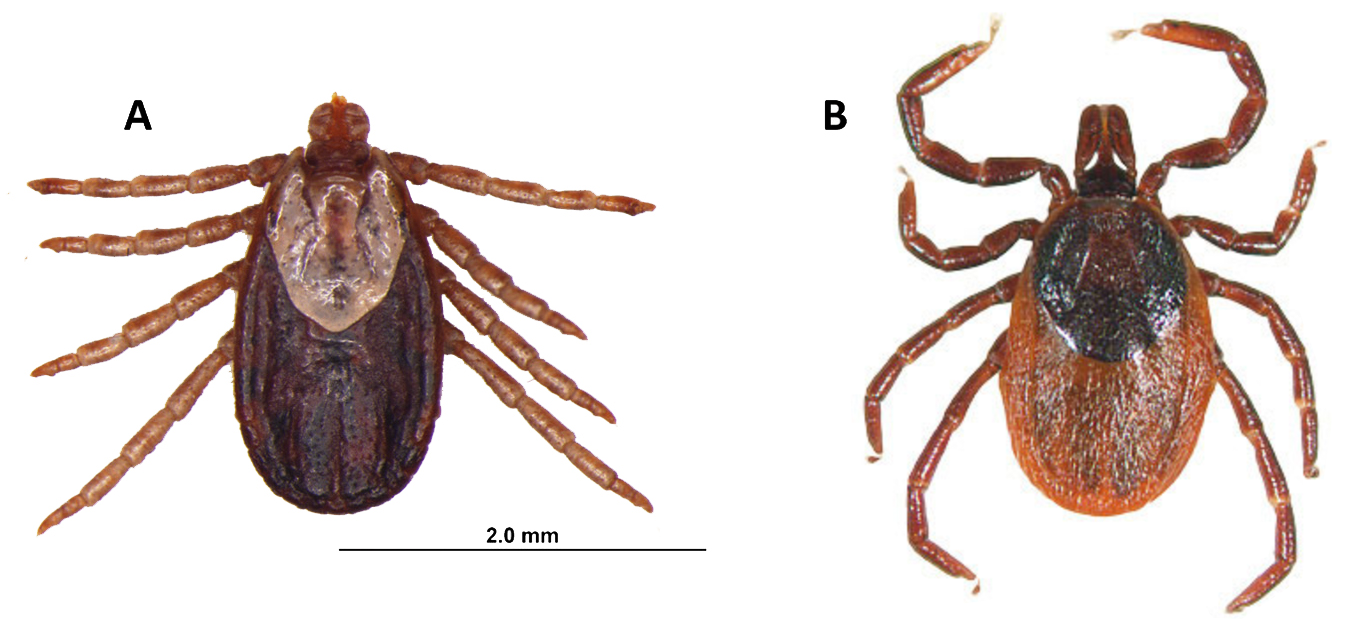
Scientists have found one tick, Dermacentor albipictus, the winter tick, that harbors B. duncani. D. albipictus is not known to bite humans often, instead spending almost their whole life on large mammals like deer or moose. These ticks also have been found to parasitize horses, cats and dogs in different parts of the country.
(A) Adult female Dermacentor albipictus. (B) Adult female Ixodes pacificus, image courtesy of TickEncounter, University of Rhode Island.
Clinically in humans, B. duncani can be very serious. It has been difficult to even study this species because the parasite could not be grown in a lab setting until very recently, and lab-infected mice and hamsters die within a few weeks of being infected.
The first human cases included two patients who died of the infection. Yet most doctors on the West Coast have never heard of it.
New studies show that B. duncani has acquired resistance to regular antiparasitic drugs including atovaquone, azithromycin, clindamycin, and quinine.
But recent in vitro studies sponsored by Bay Area Lyme Foundation have shown that an herbal compound studied and used in Africa against malaria (cryptolepis sanguinolenta) has shown positive treatment effects against both B. duncani and B. burgdorferi in in vitro studies.
Some physicians are already using this herbal medicine in their patients in the US. (Please note: this herb has shown some toxicity and should not be taken without physician supervision)
Doctors need to suspect additional tick-borne infections—many do not
While Babesia has only been a CDC-reportable disease for a decade, we do know it is the most commonly reported tick-borne infection after Lyme disease.
Despite that knowledge, babesiosis is typically not discovered until later, if at all. Obviously when a patient is infected with both a bacterium and a parasite, multiple drugs are usually required for effective treatment.
Research from the MyLymeData patient registry confirms the finding that Babesia is the most common co-infection among chronically ill patients.
Prompt and complete diagnosis of patients with tick-borne infections—bacteria, viruses and parasites, is paramount to giving patients the best chance at full recovery.
While Lyme disease is the most common tick-borne infection, there are others that can also cause congenital infections, severe disease and even death.
Testing for babesiosis is somewhat better than for Lyme, since a pathologist can actually see a Babesia parasite in red blood cells on a blood smear. However, it requires the doctor to suspect an additional tick-borne infection and order the blood smear analysis by the pathologist, which many do not.
Until we have more sensitive testing, (preferably unbiased, direct pathogen testing which detects ALL tick-borne infections), and more targeted, effective therapeutics, thousands of cases of Lyme and co-infections, including Babesia, will be misdiagnosed yearly, with sometimes fatal consequences.
Wendy Adams is Research Grant Director for the Bay Area Lyme Foundation and on its Advisory Board. She has served as a member of the federal Tick-Borne Disease Working Group and is a member of the Lyme Disease Advisory Committee of the California Department of Health.
References
Abraham, Amanah, et al. “Establishment of a Continuous in Vitro Culture of Babesia Duncani in Human Erythrocytes Reveals Unusually High Tolerance to Recommended Therapies.” Journal of Biological Chemistry, vol. 293, no. 52, 2018, pp. 19974–19981., https://doi.org/10.1074/jbc.ac118.005771.
Djokic, Vitomir, et al. “Protozoan Parasite Babesia Microti Subverts Adaptive Immunity and Enhances Lyme Disease Severity.” Frontiers in Microbiology, vol. 10, 2019, https://doi.org/10.3389/fmicb.2019.01596.
Duncan, Kathryn T., et al. “Recent Reports of Winter Tick, Dermacentor Albipictus, from Dogs and Cats in North America.” Veterinary Parasitology: Regional Studies and Reports, vol. 22, 2020, p. 100490., https://doi.org/10.1016/j.vprsr.2020.100490.
Handel AS;Krugman J;Hymes S;Inkeles S;Beneri C; “A Case of Relapsed Vertically Transmitted Babesiosis.” Journal of the Pediatric Infectious Diseases Society, U.S. National Library of Medicine, https://pubmed.ncbi.nlm.nih.gov/32964924/.
Persing, David H., et al. “Infection with a Babesia-like Organism in Northern California.” New England Journal of Medicine, vol. 332, no. 5, 1995, pp. 298–303., https://doi.org/10.1056/nejm199502023320504.
Renard, Isaline, and Choukri Ben Mamoun. “Treatment of Human Babesiosis: Then and Now.” Pathogens, vol. 10, no. 9, 2021, p. 1120., https://doi.org/10.3390/pathogens10091120.
Swei A; O’Connor KE; Couper LI; Thekkiniath J; Conrad PA; Padgett KA; Burns J; Yoshimizu MH; Gonzales B; Munk B; Shirkey N; Konde L; Ben Mamoun C; Lane RS; Kjemtrup A; “Evidence for Transmission of the Zoonotic Apicomplexan Parasite Babesia Duncani by the Tick Dermacentor Albipictus.” International Journal for Parasitology, U.S. National Library of Medicine, https://pubmed.ncbi.nlm.nih.gov/30367862/.
Zhang, Yumin, et al. “Botanical Medicines Cryptolepis Sanguinolenta, Artemisia Annua, Scutellaria Baicalensis, Polygonum Cuspidatum, and Alchornea Cordifolia Demonstrate Inhibitory Activity against Babesia Duncani.” Frontiers in Cellular and Infection Microbiology, vol. 11, 2021, https://doi.org/10.3389/fcimb.2021.624745.
Harry E. Prince, et al. “Comparison of the Babesia Duncani (WA1) IGG Detection Rates among Clinical Sera Submitted to a Reference Laboratory for WA1 IGG Testing and Blood Donor Specimens from Diverse Geographic Areas of the United States.” Clinical and Vaccine Immunology, 1 Nov. 2010, https://journals.asm.org/doi/10.1128/CVI.00256-10.
VA’s Delegate Reid Introduces Lyme Prevention & Education Bill
VA Del. David Reid
Delegate David A. Reid (D-House District 32) introduced Virginia HB 850, a Lyme disease bill, in House referral committee pending as of January 12, 2022. The bill pertains to Lyme disease; signage; instructional resources; and materials. It requires the Virginia Department of Conservation and Recreation to develop and post signage in each state park and interstate park that addressees appropriate steps that park visitors can take to prevent tick bites, how to identify Lyme disease, and where to seek treatment for Lyme and other tick-borne diseases. The bill requires the Department to install signage in areas in the Commonwealth that have been identified as most susceptible to Lyme disease first. Signage installation is to be completed in all state parks and interstate parks by January 1, 2028.
In addition, the bill requires the Secretary of Education, in collaboration with the Secretary of Health and Human Resources and the Secretary of Natural Resources, to develop instructional resources and materials to assist school boards and local and regional public libraries in establishing an education and awareness program to protect children from Lyme disease and other tick-borne infections.
Instructional resources and materials are required to be appropriate for school aged children; to provide information on the identification of ticks, recommended procedures for safe tick removal, and best practices to protect from ticks. These resources may include video productions, pamphlets, and demonstration programs to illustrate the sizes of various ticks, including sizes before and after each variety of tick has become engorged, to assist with the identification of a tick and the reaction on the skin that may result from a tick bite; and will be available to school boards and local and regional public libraries at no charge.
LDA NOTE: The Lyme Disease Association Inc. (LDA) was contacted by Virginia Delegate Reid almost a year ago to share his concerns about the spread of Lyme disease in the region and asked LDA to provide input into possible ideas for legislation to help stop the spread of Lyme disease. In a subsequent zoom meeting with LDA President Pat Smith, the LDA provided to him a number of possible ideas related to prevention and education, especially in parks.