One of the most egregious minor consent bills to ever surface in this country, B23-0171, became D.C. law on December 23, 2020. The measure, which received widespread opposition from advocates nationwide, makes it possible for 11 year olds to be vaccinated behind their parents’ backs. This dangerously misguided law includes provisions to ensure that parents never find out their child got vaccinated by requiring insurance companies, vaccine administrators and schools to conceal the vaccination(s) from parents. This effectively prevents parents from ever knowing their child’s complete medical history.
Medical and legal experts say the D.C. minor consent law is predatory, racist and destructive to children and families everywhere. That’s why we’re asking for your immediate help to overturn it! (Keep reading; helping is easy.)
Before the minor consent law goes into effect, it has to undergo a 30-day congressional review period per the District of Columbia Home Rule Act. The act makes it possible for Congress to overturn the law, although this has only been done successfully a handful of times in history. As such, we are urging all U.S. advocates to support a congressional resolution that’s been filed to strike down the D.C. minor consent law. If we don’t stop this bad law in our nation’s capital, it could easily become law in your state!
The D.C. minor consent law is a bad law. In addition to putting children in potential physical danger, it breaks multiple federal laws, instructs healthcare providers to engage in criminal misconduct by falsifying medical records, and targets disadvantaged inner-city minorities by paving the way for them to be “groomed” for medical interventions that their parents (and possibly even their own doctors) will never know about. Most of all, it erodes the parent-child relationship by interfering in a family’s personal matters and encouraging kids to keep secrets from their parents. This, experts say, lays the foundation for a relationship filled with fear, paranoia and mistrust. Allowing minor children to consent to vaccination is dangerous because children don’t have the emotional maturity or intellectual capacity to make important medical decisions. Additionally, by removing parents from their child’s healthcare decisions, it forces young pre-teens and teens to make complex choices without the advice or support of those who know and care for them best — their parents.
The pharmaceutical industry and medical lobbying groups are hard at work redefining the parent-child relationship and influencing lawmakers and public officials to give ultimate healthcare decision-making authority to the state. However, there is no justification for the state to eliminate a parent’s legal and moral right to make an informed decision about vaccination on behalf of their minor child, especially when doctors and other vaccine providers have no liability or accountability for what happens to the child after vaccination.
The D.C. minor consent law needs to be overturned immediately! We are asking people from all over the country to take action NOW so that this predatory law in our nation’s capitol is abolished and won’t set precedent for other states to follow! Taking action is easy. Simply click below to send a pre-drafted (and customizable) email and tweet to your federal officials urging them to support the congressional resolution to strike down the D.C. minor consent bill! Remember: No one knows children like their parents do, and coming between families will have devastating, long-lasting effects — both physical and psychological.
Your home address information is required from the legislative offices to ensure you are reaching out to your designated representatives. Your email and your phone number are used to establish connection with your designated representatives. Messages from non-constituents don’t have the same impact on a legislator as messages from verified constituents, who can vote for that officeholder. We do not share your name and contact information with any third parties unless legally required to do so.
This is important for children everywhere, but particularly for vulnerable children with Lyme/MSIDS.
Since vaccines are not without risks and have directly caused death and severe adverse reactions, children need direction from their parents who are the most vested in their lives and health. Not only that, but children being treated for tick-borne illness have complicated regimens that parents need to be completely privy to. Blocking them from this process will yield nothing fruitful.
While proponents of this bill will state childabuse as a viable reason for this harmful bill, there are already laws protecting children.
Children are only children for a small window of time. For those children desiring vaccination against their parents’ approval, they don’t have to wait long to be on their own to do what they want. In the meantime, let parents do what they feel is best for their children.
Right here in the U.S., the family of Justina Pelletier found that out the hard way in 2014 when the state of Massachusetts took Justina from them and placed her in the custody of Boston Children’s Hospital. Doctors there were free to enroll her in clinical trials (without parental consent) for the somatoform disorder diagnosis they had given her, rather than continuing the treatment for Mitochondrial disease that her parents and doctors at Tufts Medical Center had been following. After public outrage following her parents going public, Justina was finally returned to her parents 16 months later, in much worse condition than when she was taken away.Her story reemerged in 2016 as the family filed suit in federal court against the state and the hospital who so severely injured their daughter.
Isaiah Rider of Missouri was also taken by the state over a disagreement regarding his treatment. He was finally released by the state of Illinois who had been granted custody (though he was never a resident of the state until he went into foster care) when Lurie Children’s Hospital (Chicago)doctors decided they knew better than his mom. While in foster care, Rider suffered sexual assault. He was finally returned to the custody of his grandparents in his home state, but wasn’t fully released from Illinois care until June of 2016, months after his 18th birthday!
AS SAD AS IT SOUNDS, THOUGH, THE RIDERS AND THE PELLETIERS ARE THE LUCKY ONES.
Scientists Warn of Potential COVID Vaccine-Related ‘Ticking Time Bomb’
Studies suggest that COVID vaccines may trigger antibody-dependent enhancement in some people, a condition that could cause them to develop more severe symptoms when exposed to the wild virus than if they hadn’t been vaccinated.
Associate Professor of Health Sciences Adam MacNeil at Brock University, Canada and his Ph.D. student Jeremia Coish were among the earliest to warn, last June, of the dangers of not looking very carefully at the possibility that vaccines might trigger antibody-dependent enhancement(ADE) of disease. This could mean that people who are vaccinated might, paradoxically, suffer more severe disease when exposed to the wild virus than if they hadn’t been vaccinated.
In their aptly titled article, “Out of the frying pan and into the fire? Due diligence warranted for ADE in COVID-19,” published in the journal Microbes and Infection in June 2020, MacNeil and Coish argue that ADE is well known to be a risk for coronavirus-mediated infections, as well as dengue.
For those not already familiar with ADE, it is the paradoxical immune response that makes a person who was previously exposed to the disease, or a vaccine targeting it, more — not less — susceptible in the event that they’re subsequently infected.
Proceed with caution
Seemingly countering this view, in August 2020, was viral epidemiologist Leah Katzelnick Ph.D., a dengue and zika specialist now in the employ of the National Institute for Allergy and Infectious Diseases headed by Dr. Tony Fauci. Along with co-author Scott Halstead,. Katzelnick argued that ADE shouldn’t be something to be feared. Katzelnick and Halstead proposed that the fundamental differences between SARS-CoV-2 infection that can cause COVID-19 and other diseases, for which ADE has been shown, meant that ADE would be highly unlikely.
They supported their arguments with evidence from cases of classic, intrinsic ADE, notably infectious peritonitis, a coronavirus infection in cats, as well as from respiratory syncytial virus, dengue and SARS — suggesting significant differences in the pathology, epidemiology and immune responses involved in these diseases as compared with COVID and SARS-CoV-2 infection.
Careful readers of Halstead and Katzelnick’s paper will note that while the authors largely dismiss the ADE risk, they very clearly identify a risk of vaccine hypersensitivity (or VAH), a closely related immunological hyper-reaction that was first identified in the late 1960s when children developed atypical measles following measles vaccination.
Many who’ve used the paper to dismiss ADE risks may only have read the title and abstract and not picked up that Katzelnick and Halstead dismiss only intrinsic ADE or iADE (i.e. the risk of disease enhancement on re-infection in the absence of vaccination).
They also may not have read the sombre advisory in the paper’s last sentence:
“Given the magnitude of the repertoire of COVID-19 problems and the need for an effective vaccine, the full force of worldwide investigative resources should be directed at unravelling the pathogenesis of VAH.”
There is not much to suggest that this advisory has been heeded, other than the fact that thousands of volunteers have been put through Phase 3 trials and there has been no evidence of spikes in more severe reactions among those vaccinated with the real thing, as opposed to the placebo.
Herbert Virgin, Ann Arvin and colleagues, writing in Nature, one of the most influential journals in the world, made a not dissimilar call for caution back in July. These authors discuss the great difficulties in identifying the incidence and frequency of ADE (and VAH) and suggest that “… it will be essential to depend on careful analysis of safety in humans as immune interventions for COVID-19 move forward.”
Transparency is key
This requires full transparency of surveillance data so that cases of infection and reinfection post-vaccination can be correlated against severe reactions following infection or vaccination. It also requires time — much more time than we’ve had so far.
Presently, data released by VAERS (Vaccine Adverse Event Reporting System) in the U.S. and the MHRA (Medicines and Healthcare products Regulatory Agency) in the UK don’t come close to telling us anything about the ADE or VAH risk. In fact, there will have to be a lot more re-infection before we know conclusively one way or another. And will we be able to find out if there are genuine issues with ADE or VAH, or will the authorities manage to keep a lid on it by just not communicating them given many reactions will be substantially delayed following vaccination?
Timothy Cardozo from New York University and Ronald Veazy from Tulane University took it a step further in their article in the International Journal of Clinical Practice published in October, when Phase 3 trials for the COVID frontrunner vaccines were in full swing. They argued not only that vaccine-mediated ADE (i.e. VAH) risks were more than just theoretical, they also suggest that the risks may be greater following particular types of mutations in the circulating viruses.
In their discussion on SARS-CoV-2, they discuss how very tiny changes, such as changes in the conformity (shape) of its spike protein both before and after fusion with host cells, via ACE2 receptors might impact those who’ve been vaccinated. Several months on with emerging evidence that some variants are able to evade the immune response that has been trained to offer protection against the original Wuhan variants, there is cause for even greater concern. This risk also can’t be dismissed on the basis of the results of the Phase 3 trials
What Cardozo and Veazy also suggest is another point we’ve long been concerned about. That relates to the fact that trial subjects — let alone members of the public who’re now lining up for COVID vaccines — are just not being informed of these potential risks, and the delayed nature of possible ADE/VAH reactions.
What about vaccinees who become ill several months after being vaccinated, suffering the classic range of symptoms associated with many respiratory diseases (including COVID), such as fever, chills, cough, shortness of breath, headache, fatigue, and so on? Will they know that these symptoms might be related to enhanced COVID disease mediated by the vaccination given to them months before, something that didn’t occur to them because they thought the vaccine gave them protection from COVID?
Cardozo and Veazy then show how informed consent forms for volunteer subjects in vaccine trials fail to meet the required ethical standards for informed consent. While ADE is mentioned, it is generally added at the end of the list of possible risks and its implications and identification are unlikely to be adequately understood by the lay public.
With a tick in the box and a sense from regulators and vaccine makers that they’ve successfully negotiated the hurdle of ADE/VAH risks, there’s been no further discussion of the issue. The vast majority of pre-vaccinees lining up as part of the global mass vaccination roll out simply have no idea of the risk — because they’re not being told.
Could ADE be a ticking time bomb?
Does non-disclosure as part of the informed consent process constitute not only a breach of medical ethics, but also a breach of law? In our view, that’s highly likely and should evidence accrue in the future, this will be something the courts will need to grapple with.
Presently there is no evidence of any significant ADE/VAH signal — but it is too early to tell and many cases could have gone undetected.
Is it possible that some instances of ‘long COVID’ could be a form of ADE? This is a possibility we have been considering. Typically people who get long COVID don’t test as positive from nasopharyngeal swab tests. But in deep seated systemic infections the mucosa may not show evidence of viral multiplication, whereas the infection may become systemic in certain tissues and be enhanced. This possibility cannot easily be dismissed.
Could the problem increase with new variants of SARS-CoV-2? Yes, as explained above.
What you can do:
Anyone who is deciding to have the vaccine should inform themselves of the ADE and VAH risk, where there could be a considerable delay between vaccination and the experience of disease symptoms that may be more severe than those that would occur without the vaccine.
Consistent and effective use of personal prevention methods for tickborne diseases, including Lyme disease (LD), is dependent on risk awareness. To improve our understanding of the general U.S. population’s experiences with tick exposure and use of personal prevention methods, we used data from ConsumerStyles, a web-based, nationally representative questionnaire on health-related topics. Questions addressed tick bites and LD diagnosis in the last year, use of personal prevention methods to prevent tick bites, and willingness to receive a theoretical LD vaccine. Of 10,551 participants surveyed over three years:
12.3 % reported a tick bite for themselves or a household member in the last year, including 15.4 % of participants in high LD incidence (LDI) states, 16.3 % in states neighboring high LDI states, and 9.4 % in low LDI states.
Participants in high LDI states and neighboring states were most likely to use personal prevention methods, though 46.6 % of participants in high LDI states and 53.9 % in neighboring states reported not using any method. Participants in low LDI states, adults ≥ 75 years of age, those with higher incomes, and those living in urban housing tended to be less likely to practice personal prevention methods.
Likeliness to receive a theoretical LD vaccine was high in high LDI (64.5 %), neighboring (52.5 %), and low LDI (49.7 %) states.
Targeted educational efforts are needed to ensure those in high LDI and neighboring states, particularly older adults, are aware of their risk of LD and recommended personal prevention methods.
__________________
**Comment**
Well, well, it’s not hard to see through the veneer of this study. Under the guise of “educational efforts,” this is nothing more than phishing to see if people will take the jab. Our public ‘authorities’ are only concerned about Lyme disease when it suits them and typically it only suits them when there’s a lucrative vaccine in the works.
Quotes from the patients affected by the LYMErix VACCINE:
“…..Smithkline should not be able to destroy people’s lives as they have destroyed mine …”
“… As of May 8, 2000 there were 467 adverse reactions reported to VAERS, and of them 144 had complained of some sort of joint pain. Please do not let this vaccine hurt anymore people. I know SmithKline is trying to get it approved for children, PLEASE DO NOT LET THEM HURT ANYMORE KIDS…”
“….. The FDA let them put this on the market without fully testing it. The longer that this is left on the market, the more people are going to get hurt. Please stop this madness and take it off the market…”
“….. No one else should ever suffer such profound life changes through the administration of a “safe” vaccine. He would have been far better off to get Lyme Disease than to be incapacitated by something we counted on to protect his health!…”
“….Please stop this vaccine from wrecking more lives! !Respectfully submitted…”
https://madisonarealymesupportgroup.com/2016/08/04/vaccine-injuries-and-the-lyme-connection/ According to the founder of May12.org, “The LYMEerix vaccine was manufactured with ‘outer surface protein A’ (OspA). OspA is fungal and therefore has an immunosuppressive effect – causing post-sepsis syndrome. People injected with this vaccine were effected similarly to those bitten by a tick -which injects spirochetes (toxic fungi). Ironically, this vaccine was making people sick with the exact thing it was supposed to prevent!”
One thing is for certain: the Lyme vaccine has caused the very symptoms it is supposed to prohibit.
The quality and quantity of the science being used to buttress public health policy and law in the 21st century, particularly vaccine policy and law, has been debated since the mid-20th century when serious adverse reactions to whole-cell pertussis (DPT) vaccine were acknowledged in the medical literature and publicized in Europe and the U.S. This 2020 conference, like the four previous public conferences on vaccination sponsored by NVIC between 1997 and 2009, features presentations by scientists, physicians and health professionals examining vaccine science policy, law, and ethics.
Multidisciplinary Approach. During Session 1 of this conference, scientific information is provided by speakers with expertise in biology and bioinorganic chemistry; pediatrics, immunology and molecular genetics, physics, health research methods, pharmaceutical policy, family practice, internal medicine, pathology and molecular diagnostics, molecular and cellular physiology, pharmacology, immunotoxicology and microbiology.
Speakers discuss vaccine ingredients, monitoring vaccine side effects, epidemiology of SARS-Cov-2, development of COVID-9 vaccines, flaws in clinical trial designs, pharmaceutical product marketing, HPV vaccine risk factors, use of human fetal cell lines to produce and test vaccines, research into the reported association between inflammation, epigenetics and autism, and how human health is affected by the microbiome.
Before Session 1 begins, NVIC co-founder and president Barbara Loe Fisher opens the conference with a Welcome to attendees. She gives an overview of the conference and offers perspective on the need to defend autonomy and the legal right to exercise informed consent to vaccination.
Session 2
U.S. and International Vaccine Choice Advocacy
Over the past four decades but, especially, during the 21st century, the pharmaceutical, medical trade and public health industries in partnerships with Big Tech companies and global communications corporations have stepped up lobbying efforts to eliminate flexible medical, religious and conscientious belief vaccine exemptions in public health laws. The debate about the science and ethics of mandatory vaccination has become more intense in the past decade as citizens of many countries push back against one-size-fits-all vaccine policies that apply increasingly more severe societal sanctions to individuals, who maintain that use of vaccines should be voluntary.
Vaccine Laws Reviewed. Session 2 at this conference reviews vaccine laws in the U.S., Canada and Europe and how inflexible vaccine mandates impact the lives of people. Speakers discuss the ways in which grassroots vaccine safety and informed consent movements are responding to threats to autonomy and freedom of thought, speech, and conscience with educational, legislative and civil court initiatives to defend the legal right to exercise voluntary, informed consent to vaccine risk taking.
Session 3
The Paradigm Shift To Health & Liberty
The vaccine safety and informed consent movements in the U.S. and other countries have developed alongside other grassroots movements that began in the middle of the 20th century, such as social reform, environmental and holistic health movements that focused on civil and human rights, protection of the environment from industrial toxins and non-pharmaceutical options for healing and staying well. As the education level of populations is increasing in the U.S. and throughout the world, so is easier access to scientific, medical, legal and other types of information that consumers can use to make informed choices. Recent public opinion polls demonstrate that more people are asking more questions about the quality and quantity of the science being used to buttress medical policies, which rely almost exclusively on use of prescription drugs and vaccines.
Challenging the Status Quo: Medical and holistic health professionals are challenging the vaccine and drug dependent medical model as the sole option for preventing and treating illness. Attorneys are challenging the pharmaceutical industry and educational and law enforcement systems. Spiritual leaders and human rights activists are holding institutions accountable for eroding cultural values and beliefs and for violating freedom of religion and other civil liberties.
Presentations, Achievement Awards, Guest Appearance, Movie. Session 3 of this conference “The Paradigm Shift to Health & Liberty” features physicians who defend informed consent rights and have been sanctioned for exercising professional judgment and conscience; representatives of different faiths; holistic health leaders; a best selling author and an environmental protection activist; constitutional law and product liability attorneys; and a keynote presentation on “Defending Life and Liberty in the Vaccine Culture War.”
Session 3 ends with presentations of two NVIC Lifetime Achievement Awards to holistic health pioneer Dr. Joseph Mercola and posthumously to Jeanne Ohm, D.C., of the International Chiropractic Pediatric Association; a guest appearance by actor and civil rights activist Rob Schneider; and a showing of the award winning 2011 documentary The Greater Good, a character-driven movie that features interviews with families with vaccine injured children, doctors, scientists and vaccine safety and health freedom activists.
Session 4
Growing Our Grassroots Advocacy
A continuation of the scientific, medical, legal, ethical and holistic health themes that were explored in the previous three sessions, Session 4 of this conference features speakers discussing issues that inform grassroots vaccine safety and choice advocacy.
From Animal Vaccines, Medical Privacy and Adult Vaccine Mandates to Propaganda, Vaccine Liability Shields and Medical Atrocities. Topics covered in this session include animal vaccines; how to access and interpret information contained in the federal vaccine adverse event reporting system; the threat to medical privacy and informed consent rights posed by electronic health care records and vaccine tracking systems; the expansion of vaccine mandates to include adults; strategies used by mandatory vaccination proponents in state legislatures; COVID-19 vaccines; propaganda and psychological warfare; urban community education and organizing; historical examples of medical atrocities; vaccine product liability shields and the untold story of why and how the 1986 National Childhood Vaccine Injury Act was passed and then systematically dismantled.
Session 4 ends with a plea by the mother of an adult vaccine injured son for public recognition of the suffering of vaccine injured children and their families, and a brief Close by NVIC’s co-founder and president.
_____________________
**Comment**
Understanding vaccines is crucial – especially now that an unproven gene-therapy called a COVID “vaccine” is being thrust upon an unsuspecting public for a supposed virus that the CDC owns the entire genetic sequence to.
Important excerpt:
According to Martin, Fauci, Baric and the CDC “are at the hub” of the whole COVID-19 story. “In 2002, coronaviruses were recognized as an exploitable mechanism for both good and ill,” Martin says, and “Between 2003 and 2017, they [Fauci, Baric and CDC] controlled 100% of the cash flow to build the empire around the industrial complex of coronavirus.”
HOW THE CDC BROKE THE LAW
The key take-home message Martin delivers in “Plandemic” is that there’s a distinct problem with the CDC’s patent on SARS-CoV isolated from humans, because, by law, naturally occurring DNA segments are prohibited from being patented.
The law clearly states that such segments are “not patent eligible merely because it has been isolated.” So, either SARS-CoV was manmade, which would render the patent legal, or it’s natural, thus rendering the patent on it illegal.
However, if the virus was manufactured, then it was created in violation of biological weapons treaties and laws. This includes the Biological Weapons Anti-Terrorism Act of 1989, passed unanimously by both houses of Congress and signed into law by George Bush Sr. (Source)
More damage continues rolings out daily like a barrel full of monkeys, and many are warning these injections are a “ticking time bomb.”
By referring to COVID-19 vaccines as “vaccines” rather than gene therapies, the U.S. government is violating its 15 U.S. Code Section 41, which regulates deceptive practices in medical claims
The mRNA injections are gene therapies that do not fulfill a single criteria or definition of a vaccine
COVID-19 “vaccines” do not impart immunity or inhibit transmissibility of the disease. They only are designed to lessen your infection symptoms if or when you get infected. As such, these products do not meet the legal or medical definition of a vaccine
Since a vast majority of people who test positive for SARS-CoV-2 have no symptoms at all, they’ve not even been able to establish a causal link between the virus and the clinical disease
By calling this experimental gene therapy technology a “vaccine,” they are circumventing liability for damages that would otherwise apply
Did you know that mRNA COVID-19 vaccines aren’t vaccines in the medical and legal definition of a vaccine? They do not prevent you from getting the infection, nor do they prevent its spread. They’re really experimental gene therapies.
I discussed this troubling fact in a recent interview with molecular biologist Judy Mikovits, Ph.D. While the Moderna and Pfizer mRNA shots are labeled as “vaccines,” and news agencies and health policy leaders call them that, the actual patents for Pfizer’s and Moderna’s injections more truthfully describe them as “gene therapy,” not vaccines.
Definition of ‘Vaccine’
According to the U.S. Centers for Disease Control and Prevention,1 a vaccine is “a product that stimulates a person’s immune system to produce immunity to a specific disease, protecting the person from that disease.” Immunity, in turn, is defined as “Protection from an infectious disease,” meaning that “If you are immune to a disease, you can be exposed to it without becoming infected.”
Neither Moderna nor Pfizer claim this to be the case for their COVID-19 “vaccines.” In fact, in their clinical trials, they specify that they will not even test for immunity.
Unlike real vaccines, which use an antigen of the disease you’re trying to prevent, the COVID-19 injections contain synthetic RNA fragments encapsulated in a nanolipid carrier compound, the sole purpose of which is to lessen clinical symptoms associated with the S-1 spike protein, not the actual virus.
They do not actually impart immunity or inhibit transmissibility of the disease. In other words, they are not designed to keep you from getting sick with SARS-CoV-2; they only are supposed to lessen your infection symptoms if or when you do get infected.
As such, these products do not meet the legal or medical definition of a vaccine, and as noted by David Martin, Ph.D., in the video above, “The legal ramifications of this deception are immense.”
15 U.S. Code Section 41
As explained by Martin, 15 U.S. Code Section 41 of the Federal Trade Commission Act2 is the law that governs advertising of medical practices. This law, which dictates what you may and may not do in terms of promotion, has for many years been routinely used to shut down alternative health practitioners and companies.
“If this law can be used to shut down people of good will, who are trying to help others,” Martin says, “it certainly should be equally applied when we know deceptive medical practices are being done in the name of public health.”
Per this law, it is unlawful to advertise:
“… that a product or service can prevent, treat, or cure human disease unless you possess competent and reliable scientific evidence, including, when appropriate, well-controlled human clinical studies, substantiating that the claims are true at the time they are made.”3
What Constitutes ‘The Greater Good’?
Martin points to the 1905 Supreme Court ruling in Jacobson vs. Massachusetts,4 which essentially established that collective benefit supersedes individual benefit. To put it bluntly, it argued that it’s acceptable for individuals to be harmed by public health directives provided it benefits the collective.
Now, if vaccination is a public health measure that is supposed to protect and benefit the collective, then it would need to a) ensure that the individual who is vaccinated is rendered immune from the disease in question; and b) that the vaccine inhibits transmission of the disease.
Only if these two outcomes can be scientifically proven can you say that vaccination protects and benefits the collective — the population as a whole. This is where we run into problems with the mRNA “vaccines.”
Moderna’s SEC filings, which Martin claims to have carefully reviewed, specifies and stresses that its technology is a “gene therapy technology.” Originally, its technology was set up to be a cancer treatment, so more specifically, it’s a chemotherapy gene therapy technology.
As noted by Martin, who would raise their hand to receive prophylactic chemotherapy gene therapy for a cancer you do not have and may never be at risk for? In all likelihood, few would jump at such an offer, and for good reason.
Moreover, states and employers would not be able to mandate individuals to receive chemotherapy gene therapy for a cancer they do not have. It simply would not be legal. Yet, they’re proposing that all of humanity be forced to get gene therapy for COVID-19.
COVID-19 Vaccines — A Case of False Advertising
Now, if the COVID-19 vaccine really isn’t a vaccine, why are they calling it that? While the CDC provides a definition of “vaccine,” the CDC is not the actual law. It’s an agency empowered by the law, but it does not create law itself. Interestingly enough, it’s more difficult to find a legal definition of “vaccine,” but there have been a few cases. Martin provides the following examples:
• Iowa code — “Vaccine means a specially prepared antigen administered to a person for the purpose of providing immunity.” Again, the COVID-19 vaccines make no claim of providing immunity. They are only designed to lessen symptoms if and when you get infected.
• Washington state code — “Vaccine means a preparation of a killed or attenuated living microorganism, or fraction thereof …” Since Moderna and Pfizer are using synthetic RNA, they clearly do not meet this definition.
Being a manmade synthetic, the RNA used is not derived from anything that has at one point been alive, be it a whole microorganism or a fraction thereof. The statute continues to specify that a vaccine “upon immunization stimulates immunity that protects us against disease …”
So, in summary, “vaccine” and “immunity” are well-defined terms that do not match the end points specified in COVID-19 vaccine trials. The primary end point in these trials is: “Prevention of symptomatic COVID-19 disease.” Is that the same as “immunity”? No, it is not.
There Are More Problems Than One
But there’s another problem. Martin points out that “COVID-19 disease” has been defined as a series of clinical symptoms. Moreover, there’s no causal link between SARS-CoV-2, the virus, and the set of symptoms known as COVID-19.
How is that, you might ask? It’s simple, really. Since a vast majority of people who test positive for SARS-CoV-2 have no symptoms at all, they’ve not been able to establish a causal link between the virus and the clinical disease.
Here’s yet another problem: The primary end point in the COVID-19 vaccine trials is not an actual vaccine trial end point because, again, vaccine trial end points have to do with immunity and transmission reduction. Neither of those were measured.
What’s more, key secondary end points in Moderna’s trial include “Prevention of severe COVID-19 disease, and prevention of infection by SARS-CoV-2.” However, by its own admission, Moderna did not actually measure infection, stating that it was too “impractical” to do so.
That means there’s no evidence of this gene therapy having an impact on infection, for better or worse. And, if you have no evidence, you cannot fulfill the U.S. Code requirement that states you must have “competent and reliable scientific evidence … substantiating that the claims are true.”
Why Are They Calling Them Vaccines?
As noted by Martin, you cannot have a vaccine that does not meet a single definition of a vaccine. So, again, what would motivate these companies, U.S. health agencies and public health officials like Dr. Anthony Fauci to lie and claim that these gene therapies are in fact vaccines when, clearly, they are not?
If they actually called it what it is, namely “gene therapy chemotherapy,” most people would — wisely — refuse to take it. Perhaps that’s one reason for their false categorization as vaccines. But there may be other reasons as well.
Here, Martin strays into conjecture, as we have no proof of their intentions. He speculates that the reason they’re calling this experimental gene therapy technology a “vaccine” is because by doing so, they can circumvent liability for damages.
As long as the U.S. is under a state of emergency, things like PCR tests and COVID-19 “vaccines” are allowed under emergency use authorization. And as long as the emergency use authorization is in effect, the makers of these experimental gene therapies are not financially liable for any harm that comes from their use.
That is, provided they’re “vaccines.” If these injections are NOT vaccines, then the liability shield falls away, because there is no liability shield for a medical emergency countermeasure that is gene therapy.
So, by maintaining the illusion that COVID-19 is a state of emergency, when in reality it is not, government leaders are providing cover for these gene therapy companies so that they can get immunity from liability.
Under the Cover of ‘Emergency’
As noted by Martin, if state governors were to lift the state of emergency, all of a sudden the use of RT PCR testing would be in violation of 15 U.S. Code FTC Act, as PCR tests are not an approved diagnostic test.
“You cannot diagnose a thing [with something] that cannot diagnose a thing,” Martin says.“That a misrepresentation. That is a deceptive practice under the Federal Trade Commission Act. And they’re liable for deceptive practices.”
Importantly, there’s no waiver of liability under deceptive practices — even under a state of emergency. This would also apply to experimental gene therapies. The only way for these gene therapies to enjoy liability shielding is if they are vaccines developed in response to a public health emergency. There is no such thing as immunity from liability for gene therapies.
Propaganda and Vaccine Rollout Run by Same Company
Martin brings up yet another curious point. The middleman in Operation Warp Speed is a North Carolina defense contractor called ATI. It controls the rollout of the vaccine. But ATI also has another type of contract with the Department of Defense, namely managing propaganda and combating misinformation.
So, the same company in charge of manipulating the media to propagate government propaganda and censor counterviews is the same company in charge of the rollout of “vaccines” that are being unlawfully promoted.
“Listen,” Martin says. “This is a pretty straight-forward situation. You’re being lied to. Your own government is violating its own laws … They have thrown this book [15 U.S. Code Section 41] on more people than we can count.
They have shut down practitioners around the country, time and time again, for violating what are called ‘deceptive practices in medical claims’ … Guess what? They’re doing exactly that thing.”
Martin urges listeners to forward his video to your state attorney, governor, representatives and anyone else that might be in a position to take affirmative action to address and correct this fraud.
Defense contractors are violating FTC law, and gene therapy companies — not vaccine manufacturers — are conducting experimental trials under deceptive medical practices. They’re making claims of being “vaccines” without clinical proof, and must be held accountable for their deceptive marketing and medical practices.
CDC Owns Coronavirus Patents
On a side note, the CDC appears to be neck-deep in this scam pandemic, and is therefore wholly unsuitable to investigate the side effects of these experimental COVID-19 therapies. As noted by Martin, it’s like having a bank robber investigate its own crime.
Details about this came out in the documentary “Plandemic,” in which Martin explained how the CDC has broken the law — in one way or another — related to its patenting of the 2003 SARS virus.
Martin is a national intelligence analyst and founder of IQ100 Index, which developed linguistic genomics, a platform capable of determining the intent of communications. In 1999, IBM digitized 1 million U.S. patents, which allowed Martin’s company to conduct a review of all these patents, sending him down a proverbial “rabbit trail” of corruption.
In 2003, Asia experienced an outbreak of SARS. Almost immediately, scientists began racing to patent the virus. Ultimately, the CDC nabbed ownership of SARS-CoV (the virus responsible for SARS) isolated from humans.
So, the CDC actually owns the entire genetic content of that SARS virus. It’s patented under U.S. patent 7776521. They also own patents for detection methods, and for a kit to measure the virus.
U.S. patent 7279327,5 filed by the University of North Carolina at Chapel Hill, describes methods for producing recombinant coronaviruses. Ralph Baric, Ph.D., a professor of microbiology and immunology who is famous for his chimeric coronavirus research, is listed as one of the three inventors, along with Kristopher Curtis and Boyd Yount.
According to Martin, Fauci, Baric and the CDC “are at the hub” of the whole COVID-19 story. “In 2002, coronaviruses were recognized as an exploitable mechanism for both good and ill,” Martin says, and “Between 2003 and 2017, they [Fauci, Baric and CDC] controlled 100% of the cash flow to build the empire around the industrial complex of coronavirus.”
How the CDC Broke the Law
The key take-home message Martin delivers in “Plandemic” is that there’s a distinct problem with the CDC’s patent on SARS-CoV isolated from humans, because, by law, naturally occurring DNA segments are prohibited from being patented.
The law clearly states that such segments are “not patent eligible merely because it has been isolated.” So, either SARS-CoV was manmade, which would render the patent legal, or it’s natural, thus rendering the patent on it illegal.
However, if the virus was manufactured, then it was created in violation of biological weapons treaties and laws. This includes the Biological Weapons Anti-Terrorism Act of 1989, passed unanimously by both houses of Congress and signed into law by George Bush Sr., which states:6
“Whoever knowingly develops, produces, stockpiles, transfers, acquires, retains, or possesses any biological agent, toxin, or delivery system for use as a weapon, or knowingly assists a foreign state or any organization to do so, shall be fined under this title or imprisoned for life or any term of years, or both. There is extraterritorial Federal jurisdiction over an offense under this section committed by or against a national of the United States.”
So, as noted by Martin in the documentary, regardless of which scenario turns out to be true, the CDC has broken the law one way or another, either by violating biological weapons laws, or by filing an illegal patent. Even more egregious, May 14, 2007, the CDC filed a petition with the patent office to keep their coronavirus patent confidential.
Now, because the CDC owns the patent on SARS-CoV, it has control over who has the ability to make inquiries into the coronavirus. Unless authorized, you cannot look at the virus, you cannot measure it or make tests for it, since they own the entire genome and all the rest.
“By obtaining the patents that restrained anyone from using it, they had the means, the motive, and most of all, they had the monetary gain from turning coronavirus from a pathogen to a profit,” Martin says.
In the lecture above, Dr. Simone Gold — founder of America’s Frontline Doctors, which has been trying to counter the false narrative surrounding hydroxychloroquine — reviews the dangers discovered during previous coronavirus vaccine trials, and the hazards of current mRNA gene therapies, including antibody-dependent immune enhancement.
Antibody-dependent immune enhancement results in more severe disease when you’re exposed to the wild virus, and increases your risk of death. The synthetic RNA and the nanolipid its encased in may also have other, more direct side effects. As explained by Mikovits in our recent interview:
“Normally, messenger RNA is not free in your body because it’s a danger signal. The central dogma of molecular biology is that our genetic code, DNA, is transcribed, written, into the messenger RNA. That messenger RNA is translated into protein, or used in a regulatory capacity … to regulate gene expression in cells.
So, taking a synthetic messenger RNA and making it thermostable — making it not break down — [is problematic]. We have lots of enzymes (RNAses and DNAses) that degrade free RNA and DNA because, again, those are danger signals to your immune system. They literally drive inflammatory diseases.
Now you’ve got PEG, PEGylated and polyethylene glycol, and a lipid nanoparticle that will allow it to enter every cell of the body and change the regulation of our own genes with this synthetic RNA, part of which actually is the message for the gene syncytin …
Syncytin is the endogenous gammaretrovirus envelope that’s encoded in the human genome … We know that if syncytin … is expressed aberrantly in the body, for instance in the brain, which these lipid nanoparticles will go into, then you’ve got multiple sclerosis.
The expression of that gene alone enrages microglia — literally inflames and dysregulates the communication between the brain microglia — which are critical for clearing toxins and pathogens in the brain and the communication with astrocytes.
It dysregulates not only the immune system, but also the endocannabinoid system, which is the dimmer switch on inflammation. We’ve already seen multiple sclerosis as an adverse event in the clinical trials … We also see myalgic encephalomyelitis. Inflammation of the brain and the spinal cord …”
Making matters worse, the synthetic mRNA also has an HIV envelope expressed in it, which can cause immune dysregulation. As we discussed in previous interviews, SARS-CoV-2 has been engineered in the lab with gain-of-function research that included introducing the HIV envelope into the spike protein.
Are You in a High-Risk Group for Side Effects?
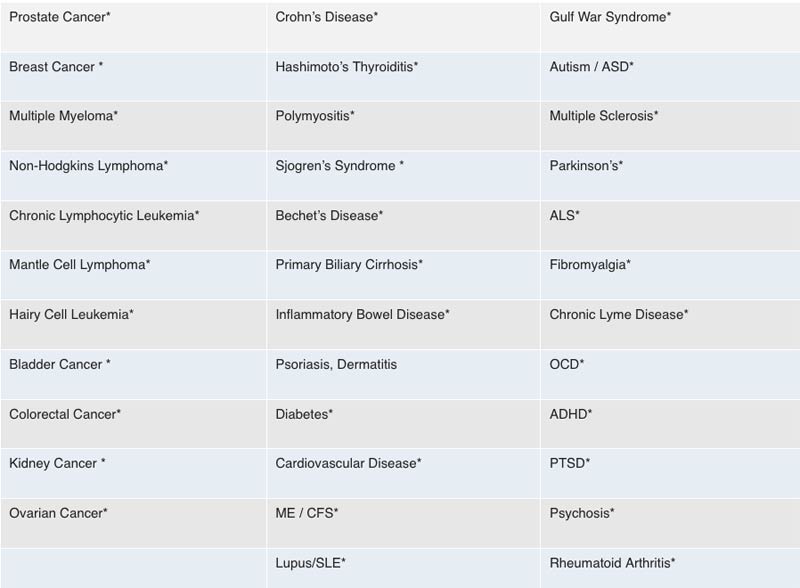
Mikovits’ hypothesis is that those who are most susceptible to severe neurological side effects and death from the COVID-19 vaccines are those who have previously been injected with XMRVs, borrelia, babesia or mycoplasma through contaminated vaccines, resulting in chronic disease, as well as anyone with an inflammatory disease like rheumatoid arthritis, Parkinson’s disease or chronic Lyme disease, for example, and anyone with an acquired immune deficiency from any pathogens and environmental toxins.
The chart below lists 35 diseases that are likely to render you more susceptible to severe side effects or death from COVID-19 gene therapy injections.
Many of the symptoms now being reported are suggestive of neurological damage. They have severe dyskinesia (impairment of voluntary movement), ataxia (lack of muscle control) and intermittent or chronic seizures. Many cases detailed in personal videos on social media are quite shocking. According to Mikovits, these side effects are due to neuroinflammation, a dysregulated innate immune response, and/or a disrupted endocannabinoid system.
Another common side effect from the vaccine we’re seeing is allergic reactions, including anaphylactic shock. A likely culprit in this is PEG (polyethylene glycol), which an estimated 70% of Americans are allergic to.
Experimental Gene Therapy Is a Bad Idea
Circling back to where we began, COVID-19 vaccines are not vaccines. They are experimental gene therapies that are falsely marketed as vaccines, likely to circumvent liability. World governments and global and national health organizations are all complicit in this illegal deception and must be held accountable.
Ask yourself the question Martin asked in his video: Would you agree to take an experimental chemotherapy gene therapy for a cancer you do not have? If the answer is no, then why would you even consider lining up for an experimental gene therapy for COVID-19 — a set of clinical symptoms that haven’t even been causally linked to SARS-CoV-2?
These injections are not vaccines. They do not prevent infection, they do not render you immune, and they do not prevent transmission of the disease. Instead, they alter your genetic coding, turning you into a viral protein factory that has no off-switch. What’s happening here is a medical fraud of unprecedented magnitude, and it really needs to be stopped before it’s too late for a majority of people.
_______________________
**Comment**
Remember, the same people/organizations behind the Lyme/MSIDS fraud are behind the current fraud surrounding COVID. They’ve been committing fraud for over 40 years and they haven’t stopped.
PLEASE NOTE CHRONIC LYME IS LISTED AS HIGH RISK FOR SIDE EFFECTS.
The entire house of cards is built upon faulty testing. Please see the following quote from the creator of the PCR test who states this fact:
It discusses the nanotechnology used in the COVID testing swab:https://www.sciencedirect.com/science/article/abs/pii/S0169409X08002640 (Are we being tested or vaccinated and nano chipped without our knowledge?) A Morgellons patient states that the same silver fibers coming out of her body are found in the COVID test swab. https://www.morgellonsexposed.com A doctor discusses this at about 12:00 (these fibers won’t burn).
Gene editing
At about 17:50 Dr. Lorraine Day states that this genetic modification makes you patentable. She states that the COVID test vaccinates you & hooks you up to the Cloud. The following patents are revealing: https://patents.google.com/patent/US10163055B2/enAbstract: Methods, systems, and products provide interfaces between intrahost networks and interhost networks within biological hosts. Neuroregional translations are performed to route communications to and from the biological hosts. Bioregional translations may also be performed to route communications to and from the biological hosts. Also see: https://madisonarealymesupportgroup.com/2020/04/29/gates-patent-for-body-activity-data-apparatus/Abstract:“Human body activity associated with a task provided to a user(1) may be used in a mining process of a cryptocurrency system. A server may provide a task to a device of a user which is communicatively coupled to the server(2). A sensor communicatively coupled to or comprised in the device(3) of the user may sense body activity of the user. Body activity data may be generated based on the sensed body activity of the user. The cryptocurrency system communicatively coupled to the device of the user may verify if the body activity data satisfies one or more conditions set by the cryptocurrency system(4), and award cryptocurrency to the user whose body activity data is verified.”(5)
Around 29:00 Dr. Martin goes into how the COVID injection is NOT a vaccine but a pathogen creator, and that the use of the term “vaccine” for this is unconscionable. A “packet of technology” is being inserted into the human body.
The Chinese biological lab in Wuhan is owned by GlaxoSmith Kline which merged with and owns 70% controlling stake in Pfizer (a COVID injection manufacturer). Pfizer manages the finances of Black Rock & Black Rock owns stakes in both Pfizer, AstraZeneca, and another company developing a COVID injection. Black Rock also has a partnership with Thompson Reuters, a multimillion dollar national media conglomerate, which essentially controls all the news.
The COVID-19 test kit (902780) was ordered back in 2018 by many countries including the U.S.
There’s an important section on anaphylaxis and a bit of history on Charles Richet’s work found here: https://www.nobelprize.org/prizes/medicine/1913/richet/lecture/ In short, it’s all about the importance of the interval between injections. Experiments by 1902 showed: (1) a subject that had a previous injection is far more sensitive than a new subject; (2) that the symptoms characteristic of the second injection, namely swift and total depression of the nervous system, do not in any way resemble the symptoms characterizing the first injection; (3) a three or four week period must elapse before the anaphylactic state results. This is the period of incubation. This 3 weeks is now what the UK is recommending for the second dose.
This alleged virus has never been isolated, has the same survival rate as the flu, many are asymptomatic or have mild symptoms, and those that die are typically elderly with comorbidities. Also – the seasonal flu has completely disappeared: https://madisonarealymesupportgroup.com/2020/11/03/why-is-cdc-scaring-us-to-death/ Yet our public ‘authorities’ want us to believe that we must get this shot due to some horrific threat.
At about 1:43 Dr. Cowan describes 31 papers from peer-reviewed journals claiming isolation of COVID-19. Here’s another similar article: https://blog.nomorefakenews.com/2020/10/19/dr-tom-cowan-explores-the-covid-virus-invented-out-of-sheer-nonsense/He states there is NOT ONE study proving COVID-19 exists. His explanation needs to be understood and shared. This is the root of the issue scientifically. Please listen to his explanation as he does a fantastic job explaining this to the lay-man.