Feb. 18, 2022
Analysis by Dr. Joseph Mercola
A simple mouth and nose spray could act as an effective shield to protect against COVID-19, adding one more tool to the arsenal of antiviral options. The straightforward solution was recommended by Dr. Mostafa Kamal Arefin of Dhaka Medical College & Hospital in Bangladesh and includes polyvinyl pyrrolidone or povidone iodine (PVP-I), a microbicidal agent with a virucidal efficacy of 99.99%.1
Writing in the Indian Journal of Otolaryngology and Head & Neck Surgery, Arefin recommended the PVP-I oro-nasal spray for health care workers and anyone else to help prevent COVID-19,2 echoing a number of other studies that have also found benefits to gargling, nasal irrigation and nebulization of PVP-I and other compounds, including Lugol’s iodine, saline and hydrogen peroxide.3
How Oronasal Sprays May Shield You From COVID-19
Arefin’s oronasal spray is made of a 0.6% PVP-I solution, kept in a “simple nasal spray device.” The spray formulation works better than drops, he noted, because it allows the active ingredient to diffuse further and reach deeper into the nose and nasopharynx, which is the upper part of the throat behind the nose. When applied, the oronasal spray acts as a protective layer, coating the nasal and oral mucosa.
Typically, if you’re exposed to SARS-CoV-2, it will enter your body through your nose and mouth, remaining there for a time before binding with ACE2 receptors and entering cells. Once inside your cells, the virus has an opportunity to multiply.
“The first step in the development of URTIs [upper respiratory tract infections],” Arefin writes, “is the adherence and colonization of the respiratory pathogen to the nasopharyngeal and oropharyngeal mucosa. Assuming nasal and oral entry of such pathogens, intranasal and intra oral application of Povidone Iodine offers a practical measure for their prevention.”4
By creating a protective shield, oronasal spray helps prevent SARS-CoV-2 from binding with ACE2 receptors and gaining entry into your cells. In a clinical trial that has not yet been published,5 Arefin and colleagues got positive results using 0.6% PVP-I Oro-nasal spray in 189 patients with COVID-19. The 0.6% solution had an efficacy rate of about 81.5%, which was greater than that of other concentrations (0.4% and 0.5%) and produced “almost no mucosal irritation.”6
Povidone-Iodine Inactivates SARS-CoV-2
Already, PVP-I gargles, throat sprays and nasal sprays are available over-the-counter in countries such as Japan and Canada.7 In Japan, a 0.45% PVP-I throat spray is available for the prevention of colds and sore throats, while gargling with the compound is part of their national respiratory guidelines.8
A 2002 study, during which patients were asked to gargle more than four times a day with a PVP-I solution, for several months up to two years, found the practice significantly reduced the incidence of chronic respiratory infections.9 In a preprint study that also advocated for the use of PVP-I nasal sprays and mouthwash to protect health care workers and reduce cross infection during the COVID-19 pandemic, it’s explained:10
“The antimicrobial action of PVP-I occurs after free iodine (I2) dissociates from the polymer complex. Once in the free form, iodine rapidly penetrates microbes and disrupts proteins and oxidizes nucleic acid structures. This interaction ultimately results in microbial death.”
PVP-I has been found to be effective in-vitro against coronaviruses that caused the severe acute respiratory syndrome (SARS) epidemic of 2002 to 2003 and the Middle East respiratory syndrome (MERS) epidemic of 2012 to 2013.11
Povidone iodine solutions have also been found to inactivate SARS-CoV-2 in as little as 15 seconds12 and potentially reduce the carriage of infectious SARS-CoV-2 in people with mild to moderate COVID-19.13 In another study of nasal irrigation among high-risk patients with COVID-19, the use of nasal irrigation with povidone iodine or baking soda reduced the risk of hospitalization by eight times compared to the national rate.14
In a letter to the editor of the Journal of Otolaryngology, Head & Neck Surgery, researchers further noted:15
“Because the reservoir for SARS-CoV-2 shedding is in the nasopharynx and nasal and oral cavities, the application of viricidal agents to these surfaces may reduce virus burden.
Numerous studies have confirmed that povidone-iodine inactivates many common respiratory viruses, including SARS-CoV-1. Povidone-iodine also has good profile for mucosal tolerance. Thus, we propose a prophylactic treatment protocol for the application of topical povidone-iodine to the upper aerodigestive tract.”
Benefits and How to Use PVP-I Oro-Nasal Spray
Using 0.6% PVP-I Oro-nasal spray is low cost, safe and effective against coronaviruses, including SARS-CoV-2. It can be used both in healthy individuals as a protective agent and in people with COVID-19 to reduce viral load and the potential for transmitting the virus to close contacts.
The side effects are minimal and include mucosal irritation, teeth staining and thyroid dysfunction. At least one study, which used both PVP-I mouthwashes and gargles four times a day for five days, found an elevation in thyroid stimulating hormone during treatment, but levels returned to normal after the treatment was stopped.16
Arefin recommends the spray for both health care workers and the general population, prior to attending public gatherings or working outside the home, and following exposure to a suspected COVID-19 patient. He advises two to three puffs in each nostril and one to three puffs in the throat every three to four hours. After every one to two weeks of use, he recommends taking a one-day break from the treatment.17
There are, however, many ways to use nasal irrigation, gargles and nebulization against COVID-19. For instance, Dr. Peter McCullough, an internist, cardiologist and epidemiologist, tweeted, “Nasal/oral viricidal washes can be done prophylactically twice a day and up to every 4 hours during early treatment. Reduce viral load for less severe illness.”18
The Front Line COVID-19 Critical Care Working Group (FLCCC) also recommends povidone-iodine as part of their I-Mask+ protocol for prevention and early outpatient treatment of COVID-19. Part of their prevention protocol includes twice daily gargling with a 1% povidone/iodine solution, while iodine nasal spray or drops are recommended as one of the first line agents in their early treatment protocol. Specifically, they recommend:19
“Use 1 % povidone-iodine commercial product as per instructions 2–3 x daily. If 1 %-product not available, must first dilute the more widely available 10 %-solution and apply 4–5 drops to each nostril every 4 hours. (No more than 5 days in pregnancy.)”
Importantly, povidone-iodine solutions sold as topical skin disinfectants to treat cuts and wounds should not be used for gargling due to potentially harmful ingredients.
Nebulized Hydrogen Peroxide for COVID-19
As I discuss in my interview with Dr. David Brownstein above, he has successfully treated hundreds of COVID-19 patients using immune boosting strategies such as intravenous or nebulized hydrogen peroxide, iodine, oral vitamins A, C and D, and intramuscular ozone. In a case report of 107 confirmed COVID-19 patients that he treated, 91 (85%) used nebulized peroxide diluted with normal saline, plus Lugol’s iodine. As explained in Brownstein’s paper:20
“A solution of 250 cc of normal saline was mixed with 3 cc of 3% hydrogen peroxide providing a final concentration of 0.04% hydrogen peroxide … Additionally, 1 cc of magnesium chloride (200 mg/ml) was added to the 250 cc saline/hydrogen peroxide bag. (This was mixed in the office for the patients.)
Patients were instructed to nebulize 3 cc of the mixture three times per day or more often if there were breathing problems. Usually one or two nebulizer treatments were reported to improve breathing problems … They reported no adverse effects. We have been using nebulized saline/hydrogen peroxide at this concentration for over two decades in his practice.
Hydrogen peroxide is continually produced in the human body with substantial amounts produced in the mitochondria. Every cell in the body is exposed to some level of hydrogen peroxide. The lungs are known to produce hydrogen peroxide. Nebulized hydrogen peroxide has been shown to have antiviral activities. Hydrogen peroxide can activate lymphocytes which are known to be depleted in COVID-19.”
I’ve embraced nebulized peroxide since the COVID-19 pandemic broke out and have received many anecdotal reports from people who have successfully used it, even at more advanced stages. Based on Brownstein’s experience, I also recommend adding iodine when nebulizing, as it appears to make it even more effective.
Proper Dilution Is the Key to Safety
Povidone-iodine gargles and nasal sprays, and nebulized peroxide diluted with saline, with or without iodine, can be safely used by most people both for prevention and in cases of active infection, provided the substances are properly diluted.
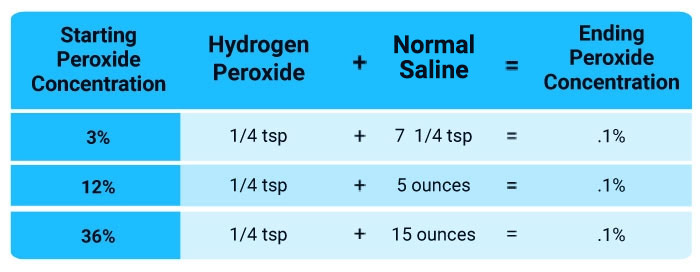
For instance, while nebulization with 0.1% to 3% hydrogen peroxide appears to be quite safe, it would be a very serious hazard to use peroxide of greater concentrations. Food grade peroxide up to 35% concentration can be obtained but should NEVER be used topically or internally. It MUST be diluted or severe injury can occur. Your safest bet is to use 3% food grade peroxide and dilute it as indicated in the chart provided below so you end up with a solution of 0.1%.
It’s interesting to note that even nebulizing normal saline may be an effective treatment for acute viral bronchiolitis, a viral infection in the small airways of your lungs.21 So while saline is considered the “inert” substance in the solution — and is often used as a placebo in trials that evaluate nebulized drugs — it may have benefits of its own.
I recommend using nebulized peroxide for any suspected respiratory infection, and the earlier you start, the better. There is no danger in doing it every day if you’re frequently exposed, and there may even be additional beneficial effects, such as a rapid rise in your blood oxygen level.
It is important to understand that this is a protocol that you need to implement BEFORE you attempt to treat COVID. Since early treatment is vital, ideally on Day 1, you want to have the nebulizer and materials already in your house ready to go. I would avoid using a battery powered hand held nebulizer and rather opt for a unit you plug into the wall.
You can find them on eBay or Amazon but make sure they have a face mask and not just a mouthpiece as you want to put the mist into your nose in addition to your lungs as many of the viruses lodge there and if you merely use a mouthpiece you will not reach these viral particles. This is an example of one that plugs in the wall and has a face mask.