Illustrative photo by Aleksandra Suzi via Shutterstock.com
It would be nice if Covid-19 disappeared before the flu and cold season hit us. Unfortunately, all three virus-caused conditions will likely be with us at once.
And that will put a dose of anxiety into every sneeze. How can we know if it’s trivial winter sniffles or something more serious? (See link for article)
_________________
**Comment**
The experts state that while some symptoms are common to each, others are unique, such as:
Covid-19 can give shortness of breath, loss of smell, and dry cough
Flu: headache, body aches, fever, chills, sore throat, loss of appetite Kids can get middle-ear infections and upset stomaches
Cold: runny/stuffy nose, no fever
Similarities:
both flu and Covid-19 can cause fever and dry cough
One of the experts state that a possible good surprise that could occur is infection rates could decline more quickly than expected and that although viruses don’t disappear they do wane over time.
They still don’t understand why seasonal flu epidemics tend to end after two months.
They also caution that differences in symptoms can be subtle and there are individual differences in presentation.
They state that rapid testing, which should be available soon, will change the game and can rule COVID out within 10 minutes.
Dr. Mike Yeadon, a former Vice President and Chief Science Officer for Pfizer for 16 years, says that half or even “almost all” of tests for COVID are false positives.
Tripura: 3-Day-Old Dies After Nurse Inserts Nasal Swab For COVID Test, Family Alleges Negligence
Soon after the cotton swabs were inserted, the infant started bleeding from the nose.
The Logical Indian Crew
Tripura | 16 Aug 2020
Writer : Sumanti Sen | Editor : Prateek Gautam | Creatives : Abhishek M
Image Credit: amarujala
A three-day-old baby died in a government hospital in Tripura’s Agartala on Wednesday, August 12, allegedly after a nurse inserted a nasal swab to take samples for its COVID-19 test. (See link for article)
In the toddler’s case, bleeding from the nose wouldn’t stop, and death occurred on the same day.
While the first case involved an undiagnosed skull defect, and the second also cannot be proven conclusively to be caused by the swab, they should serve as reminders that tests are not without risk and those risks need to be weighed.
I find it interesting that public ‘authorities,’ insist that people obtain, at all costs, vaccines and tests that they have financial interests in and turn a blind eye to risks – despite these things causing severe injury or death, but downplay, ignore, and actually sabotage patients by denying treatment to the thousands upon thousands who suffer due to the complex infection(s). Their bias couldn’t be more glaring.
Believe it or not, there are still doctors who claim that Lyme is nothing more than mass hysteria~ even with statistical data showing confirmation of the rise in new cases. How can this be? How can medical professionals still deny that Lyme is a serious health risk here in Maine? How can they argue with patients who present with information in hand about research, testing and treatment? And they do argue with the patients. They argue when a patient asks for their bloodwork to be sent to Igenex, the leading tick-borne disease laboratory for over 25 years (located in California). Patients have the right to have their bloodwork sent anywhere and yet they are being denied this option because providers use whoever their facility is networked with. Interesting…
Medical providers tell patients that Igenex scams patients and pays doctors for their usage. This is not true but I am beginning to wonder, by denying a patient the right to use whatever lab they want and by only using the lab that their medical office is contracted with, who’s scamming who here? Many providers don’t trust Igenex just because they don’t take insurance. To those providers I ask,” then why aren’t you using the tick-borne disease experienced labs that do take insurance??” Daily, I get calls and emails from patients asking what tests should their PCPs be using, which is why patient AND provider resources and educational links are on our website.
They say that Igenex is not FDA-approved.
Laboratories are not required to be FDA approved. They are, however, required to be CLIA approved. The Clinical Laboratory Improvement Amendments (CLIA) regulate laboratory testing and require clinical laboratories to be certificated by their state as well as the Center for Medicare and Medicaid Services (CMS) before they can accept human samples for diagnostic testing. In general terms, the CLIA regulations establish quality standards for laboratory testing performed on specimens from humans, such as blood, body fluid and tissue, for the purpose of diagnosis, prevention, or treatment of disease, or assessment of health.
Igenex, MDL and Galaxy Labs are just a few of over 260,000 US labs that are CLIA-approved and offer highly reliable tests sand panels tarting at $495.
This is a smoke screen practiced by doctors who do not:
understand how labs work and are federally regulated
do not support the new evidence-based scientific research
And why, Why is this still so controversial in 2020?
Did you know that vitamins and supplements are not FDA approved? They are regulated by the U.S. Dietary Supplement Health and Education Act of 1994. Now you know, and does that change how you feel about taking that One A Day vitamin or Melatonin before bed? I didn’t think so.
Medical providers who do not fully understand tick-borne disease will use this argument every time and it back fires, every time. It only shows their patient what they don’t know.
Medical providers who continue to spread “fake news” about how other medical providers and labs work, well folks, that is the real scam and it goes to show what they don’t know.
Doctors are just ignorant pawns used by ‘authorities’ who have severe conflicts of interest. Time for doctors to wake up and listen to patients who have been saying the same things for over 40 years. Time for a public health reboot and a CDC, NIAID, FDA walk-away movement:
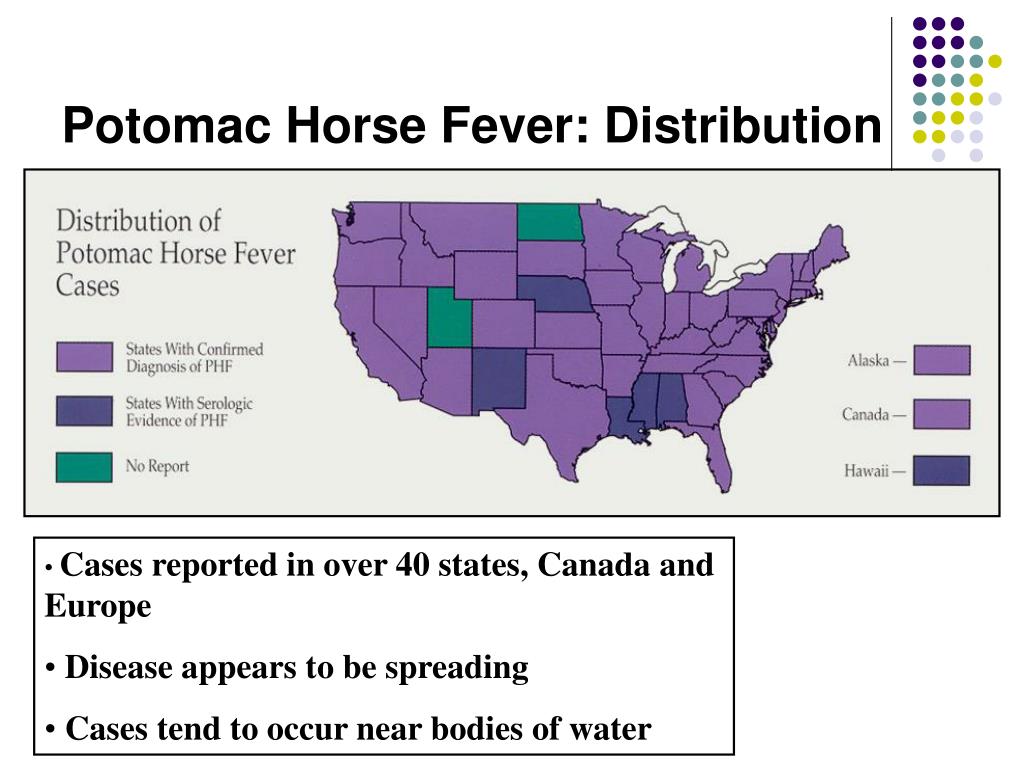
Horse owners and veterinarians in Alberta are on alert after an outbreak of Potomac horse fever, which causes death in up to 30 percent of cases. The disease causes diarrhea, depression and intestinal problems and can occur after horses ingest snails, slugs and insects in their food. (See link for article)
_________________
**Comment**
Equine monocytic ehrlichiosis, or Equine neorickettsiosis is commonly known as Potomac horse fever (PHF).
While PHF occurs typically in late spring and early fall in temperate areas, it is spreading and has been reported in over 40 states, Canada, and Europe. It tends to occur near bodies of water:
The agent behind it is Neorickettsia risticii, found in flukes (flatworms) that develop through one stage in aquatic snails. Horses drinking from streams swallow them but they are also picked up by aquatic insects – the second stage (caddisflies, mayflies, damselflies, dragonflies) that might transmit it to horse as they graze.
The second link in the cycle are in bats and barn swallows (N. risticci has been found in their intestinal tracts) that feed on the aquatic insects. It is unknown if bat and barn swallow fecal material infects horses as well.
Potomac horse fever can be mild to life-threatening affecting intestinal cells and monocytes. It causes fever, poor appetite, depression, and diarrhea. Possible lameness with limb edema may occur as well as elevated heart rate, dark mucus membranes, sweating, and signs of mild colic.
PHF is confirmed by lab identification in blood or manure samples. It may be confused with salmonella and the horse should be considered contagious to both animals and humans until fecal salmonella tests are negative.
Treatment is antibiotics, particularly oxytetracycline, IV fluids, electrolyte therapy, and non-steroidal anti-inflammatory drugs to alleviate pain.
There was a 2005 outbreak in Minnesota. They theorize mayflies from the Missippi River were attracted to bright lights outside barns which blew into the show grounds and infected at least six horses. Other cases occured on area farms at the same time that had lights by horse barns.
Turn off lights when aquatic insects are hatching in summer.
According to this article, PHF is NOT considered contagious or is passed between horses with casual contact. If more than one horse is affected it is believed that they all consumed infected insects: https://equusmagazine.com/diseases/potomac-horse-fever-brief
Bartonella henselae is a fastidious intraerythrocytic, gram-negative bacteria that causes cat scratch disease in humans. Ixodes ricinus (castor bean tick) has been confirmed to be a competent vector of B. henselae, and some indirect evidences from clinical cases and epidemiological studies also suggested that some other tick species, including Rhipicephalus sanguineus (brown dog tick, pantropical dog tick or kennel tick), may transmit the bacteria. B. henselae has been detected in R. sanguineus but no experimental investigations have been performed to evaluate the vector competency of this tick species regarding B. henselae transmission.
To this end, this work aimed to assess the transstadial transmission of B. henselae between larvae and nymphs of R. sanguineus as well as transmission by nymphs infected at the larval stage. Four hundred B. henselae negative larvae were fed with B. henselae-infected blood by using an artificial membrane feeding system.
After five days of feeding:
B. henselae was detected by PCR in 57.1% (8/14) of engorged larval pools
66.7% (4/6) of semi-engorged larval pools
66.7% (2/3) of larval feces pools
after molting, B. henselae DNA was also detected in 10% (1/10) of nymph pools, but not in tick feces
after a pre-fed step of nymphs infected at the larval stage on non-infected blood meal, B. henselae was detected by PCR in blood sample from the feeder, but no Bartonella colonies could be obtained from culture
These findings showed that B. henselae could be transstadial transmitted from R. sanguineus larvae to nymphs, and also suggest that these nymphs may retransmitted the bacteria through the saliva during their blood meal.
This is the first study that validated the artificial membrane feeding system for maintaining R. sanguineus tick colony. It shows the possibility of transstadial transmission of B. henselae from R. sanguineus larvae to nymphs.
The other theory is that the tick’s ability to suppress the immune system reactivates a latent Bartonella infection already within the body. Bartonella is prolific and can be obtained in many, many ways besides the bite or scratch of a cat: https://madisonarealymesupportgroup.com/2016/01/03/bartonella-treatment/
To date, Bartonella isn’t even on mainstream doctor’s radar for those bitten by ticks. This must change. Bartonella can be a severe, chronic infection that causes untold damage both physically and mentally.