Background: Morgellons disease (MD) is a dermopathy that is associated with tick-borne illness. It is characterized by spontaneously developing skin lesions containing embedded or projecting filaments, and patients may also experience symptoms resembling those of Lyme disease (LD) including musculoskeletal, neurological and cardiovascular manifestations. Various species of Borrelia and co-infecting pathogens have been detected in body fluids and tissue specimens from MD patients. We sought to investigate the coexistence of Borrelia burgdorferi(Bb) and Helicobacter pylori(Hp) in skin specimens from MD subjects, and to characterize their association with mixed amyloid biofilm development.
Methods: Testing for Bb and Hp was performed on dermatological specimens from 14 MD patients using tissue culture, immunohistochemical (IHC) staining, polymerase chain reaction (PCR) testing, fluorescent in situ hybridization (FISH) and confocal microscopy. Markers for amyloid and biofilm formation were investigated using histochemical and IHC staining.
Results: Bb and Hp were detected in dermatological tissue taken from MD lesions. Bb and Hp tended to co-localize in foci within the epithelial tissue. Skin sections exhibiting foci of co-infecting Bb and Hp contained amyloid markers including β-amyloid protein, thioflavin and phosphorylated tau. The biofilm marker alginate was also found in the sections.
Conclusions: Mixed Bb and Hp biofilms containing β-amyloid and phosphorylated tau may play a role in the evolution of MD. View Full-Text
New research from theCompanion Animal Parasite Council (CAPC)gives people and their health care providers a way to assess their risk for Lyme disease, thanks to man’s best friend. The studyconfirms dogs are sentinels to assess human risk for tick-borne Lyme disease.
Lyme disease (LD) is the most common vector-borne disease in the United States. Early confirmatory diagnosis remains a challenge, while the disease can be debilitating if left untreated. Further, the decision to test is complicated by under-reporting, low positive predictive values of testing in non-endemic areas and travel, which together exacerbate the difficulty in identification of newly endemic areas or areas of emerging concern. Spatio-temporal analyses at the national scale are critical to establishing a baseline human LD risk assessment tool that would allow for the detection of changes in these areas. A well-established surrogate for human LD incidence is canine LD seroprevalence, making it a strong candidate covariate for use in such analyses. In this paper, Bayesian statistical methods were used to fit a spatio-temporal spline regression model to estimate the relationship between human LD incidence and canine seroprevalence, treating the latter as an explanatory covariate. A strong non-linear monotonically increasing association was found. That is, this analysis suggests that mean incidence in humans increases with canine seroprevalence until the seroprevalence in dogs reaches approximately 30%. This finding reinforces the use of canines as sentinels for human LD risk, especially with respect to identifying geographic areas of concern for potential human exposure.
Joining me to discuss the study and it’s uses is Dr. Craig Prior. Dr. Prior is a board member and past-president of the Companion Animal Parasite Council (CAPC). From Australia, he’s been a practicing veterinarian in Nashville, Tennessee for over 25 years and currently consults with vets nationwide.
Rocky Mountain spotted fever (RMSF) is associated with high mortality and requires prompt identification and treatment to ensure better outcomes.
Case Report:
We describe an advanced case of RMSF in a 45-year-old female patient with pet dog exposure who presented with altered mental status, dyspnea, and ataxia progressing to septic shock and acute hypoxic respiratory failure requiring intubation and mechanical ventilation.
Conclusions:
This case illustrates the importance of keeping RMSF in the differential diagnosis in patient populations outside of the usual geographic areas of incidence in the appropriate clinical setting.
___________________
**Comment**
This is what can happen when diagnosis is delayed.
This woman that lived in the suburbs had a 7-day history of fevers associated with headache, arthralgias, nausea, fatigue, and neck pain, but did NOT have the tell-tale blotchy RMSF rash.
Two days later, she worsened with confusion, combativeness, dyspnea, and ataxia. She got multiple recent bug bites from her pet dogs sleeping inher bed. The dogs were not up to date on flea and tick medication but were healthy and showed no sign of illness.
Rule #1: Do NOT sleep with pets. The risk is too great.
Rule #2: If you choose to have pets, make sure you treat them if they go outdoors. The risk is too great.
Rule #3: Doctors need to start treating this plague with the respect it deserves and frankly should keep it in the back of their minds AT ALL TIMES.
Positive findings were R. typhi IgM 1: 1024 (normal <1: 64), R. Rickettsii IgM 1: 1024 (normal <1: 64), IgG 1: 128 (normal <1: 64), and echovirus Ab 1: 80 titer (normal <1: 80). The Rickettsial titers were repeated for possible cross-reactivity and R. typhi antibodies were noted to be negative (<1: 64).
Although R.typhi was ruled out due to cross-reactivity, I believe we will start seeing more of this strain in the future.
The patient improved on doxycycline, the drug of choice for RMSF and was discharged.
Ehrlichia muris subsp. eauclairensis is recognized as the etiological agent of human ehrlichiosis in Minnesota and Wisconsin. We describe the culture isolation of this organism from a field-collected tick and detail its relationship to other species of Ehrlichia. The isolate could be grown in a variety of cultured cell lines and was effectively transmitted between Ixodes scapularis ticks and rodents, with PCR and microscopy demonstrating a broad pattern of dissemination in arthropod and mammalian tissues. Conversely, Amblyomma americanum ticks were not susceptible to infection by the Ehrlichia. Histologic sections further revealed that the wild-type isolate was highly virulent for mice and hamsters, causing severe systemic disease that was frequently lethal. A Himar1 transposase system was used to create mCherry and mKate-expressing EmCRT mutants, which retained the ability to infect rodents and ticks.
Importance: Ehrlichioses are zoonotic diseases caused by intracellular bacteria that are transmitted by ixodid ticks. Here we report the culture isolation of bacteria which are closely related to, or the same as the Ehrlichia muris subsp. eauclairensis, a recently recognized human pathogen. EmCRT, obtained from a tick removed from deer at Camp Ripley, Minnesota, is the second isolate of this subspecies described, and is distinctive in that it was cultured directly from a field-collected tick. The isolate’s cellular tropism, pathogenic changes caused in rodent tissues, and tick transmission to and from rodents are detailed in this study. We also describe the genetic mutants created from the EmCRT isolate, which are valuable tools for the further study of this intracellular pathogen.
_________________
**Comment**
OTHER MODES OF TRANSMISSION
Ehrlichia chaffeensis has been shown to survive for over a week in refrigerated blood. Therefore these bacteria may present a risk for transmission through blood transfusion and organ donation. It has also been suggested that ehrlichiosis can be transmitted from mother to child, and through direct contact with slaughtered deer.(14, 15)
The first-line standard of care treatment for adults with Lyme disease is doxycycline, a tetracycline antibiotic. Other antibiotics that have activity against borrelia include the penicillin-like antibiotic, amoxicillin, and the cephalosporin, Ceftin. The mainstay of treatment is with oral (pill) antibiotics, but intravenous antibiotics are sometimes indicated for more difficult to treat cases such as meningitis, late Lyme arthritis, or neurologic-Lyme disease.
Why are antibiotics the first line of treatment for Lyme disease?
The use of antibiotics is critical for treating Lyme disease. Without antibiotic treatment, the Lyme bacteria can more easily evade the host immune system and persist in the body. Antibiotics go into the bacteria preferentially and either stop the multiplication of the bacteria (doxycycline) or disrupt the cell wall of the bacteria and kill the bacteria (penicillins). By stopping the growth or killing the bacteria the human host immune response is given a leg up to eradicate the residual infection. Without antibiotics, the infection in Lyme disease can more readily persist and disseminate.
What are the side effects of Lyme disease treatments?
Antibiotics, like all medications, have the potential for side effects. Any antibiotic can cause skin rashes, and if an itchy red rash develops while on antibiotics, a patient should see their physician. Sometimes symptoms worsen for the first few days on an antibiotic. This is called a Herxheimer reaction and occurs when the antibiotics start to kill the bacteria. In the first 24 to 48 hours, these dead bacteria stimulate the immune system to release inflammatory cytokines and chemokines that can cause increased fever and achiness. This should be transient and last no more than a day or two after the initiation of antibiotics.
The most common side effect of the penicillin antibiotics is diarrhea, and occasionally even serious cases caused by the bacteria Clostridium difficile. This bacterial overgrowth condition occurs because antibiotics kill the good bacteria in our gut. It can be helpful to use probiotics to restore the good bacteria and microbiome balance.
Prognosis
The prognosis after early treatment of Lyme disease is generally very good. The prognosis worsens, however, when diagnosis and treatment are delayed.
Most patients with early Lyme disease infection recover with antibiotics and return to their normal state of health. However, some patients suffer from chronic symptoms related to Lyme disease despite standard of care antibiotic therapy. For research studies, a defined subset of this condition is called Post Treatment Lyme Disease Syndrome (PTLDS).
What is Post Treatment Lyme Disease Syndrome?
Symptoms of Post Treatment Lyme Disease
Include severe fatigue, musculoskeletal pain, & cognitive problems
Can significantly impact patients’ health and quality of life
Can be debilitating and prolonged
Post Treatment Lyme Disease Syndrome (PTLDS) represents a subset of patients who remain significantly ill 6 months or more following standard antibiotic therapy for Lyme disease. PTLDS is characterized by a constellation of symptoms that includes severe fatigue, musculoskeletal pain, sleep disturbance, depression, and cognitive problems such as difficulty with short-term memory, speed of thinking, or multi-tasking. In the absence of a direct diagnostic biomarker, PTLDS has been difficult to diagnose by physicians, and its existence has been controversial. However, our clinical research shows that meticulous patient evaluation when used alongside appropriate diagnostic testing can reliably identify patients with typical symptom patterns of PTLDS.
Our research indicates the chronic symptom burden related to PTLDS is significant. Although often invisible to others, the negative impact on quality of life and daily functioning is substantial for PTLDS sufferers.
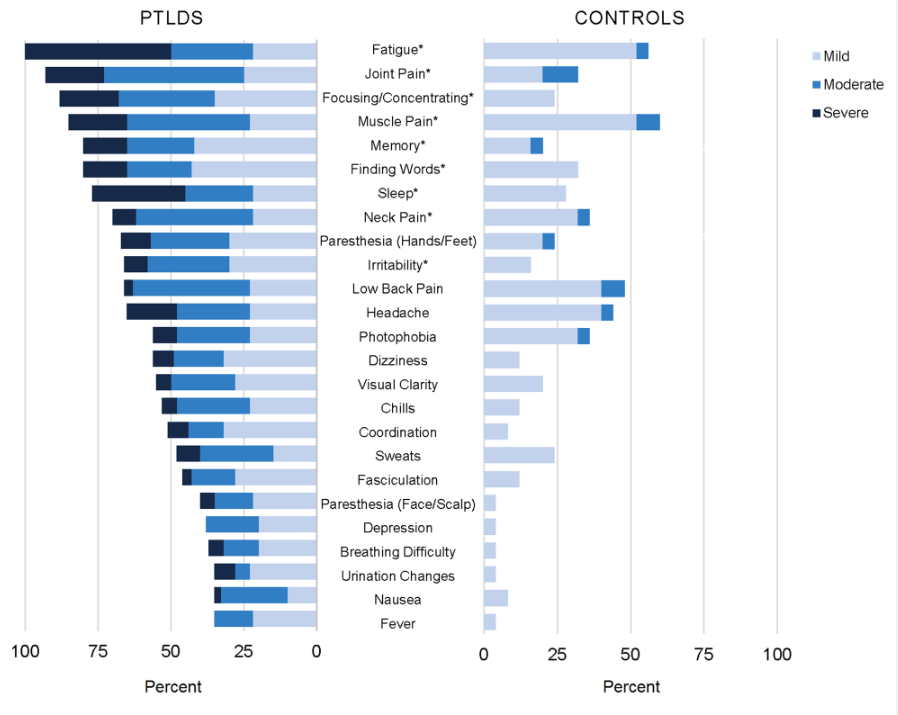
In our study, participants with Post Treatment Lyme Disease Syndrome (PTLDS) & controls were asked about presence and severity of 36 signs/symptoms over the past 2 weeks. Displayed are the 25 signs/symptoms with a statistically significant difference in severity by group (P<0.05) ordered by frequency within the PTLDS group. The nine signs/symptoms with a statistically significant difference at the p<0.001 level are indicated with an asterisk*.
The chronic symptom burden related to Lyme disease is considerable, as shown on the left side of the graph above, and statistically significantly greater than the aches and pains of daily living experienced by the control group, on the right.
What are the risk factors for Post Treatment Lyme Disease Syndrome?
Risk factors for Post Treatment Lyme Disease Syndrome include:
Delay in diagnosis
Increased severity of initial illness
Presence of neurologic symptoms
Increased severity of initial illness, the presence of neurologic symptoms, and initial misdiagnosis increase the risk of Post Treatment Lyme Disease Syndrome. PTLDS is especially common in people that have had neurologic involvement. The rates of Post Treatment Lyme Disease Syndrome after neurologic involvement may be as high as 20% or even higher. Other risk factors being investigated are genetic predispositions and immunologic variables.
In addition to Borrelia burgdorferi, the bacteria that causes Lyme disease, there are several other tick-borne co-infections that can also contribute to more prolonged and complicated illness.
What causes Post Treatment Lyme Disease Syndrome?
The causes of PTLDS are not yet well understood but our Center is investigating the potential roles of:
Infection-induced immune dysfunction or auto-immunity
Inflammation
Persistent bacterial infection or bacterial debris
Neural network alteration
Other tick-borne infections
Other biologic mechanisms of disease
Our research has validated PTLDS as a serious and impairing condition. However, the causes of PTLDS are not yet well understood or validated, and the term PTLDS does not mean post-infection or imply an assumption of underlying biologic mechanisms. The roles of immune dysfunction, autoimmunity, persistent bacterial infection, neural network alteration, and other potential causative biologic mechanisms of PTLDS are being investigated at our Center.
Research at our Center aims to understand the biologic drivers of all manifestations of Lyme disease so that diagnostics can be improved, and more effective treatments developed to enhance patients’ health outcomes.
Is there a cure for Post Treatment Lyme Disease Syndrome?
Currently there are no FDA approved treatments for Post Treatment Lyme Disease Syndrome. Therefore, treatments must be individualized by addressing specific symptoms and circumstances for each individual.
Late Lyme Arthritis
What is the prognosis for Late Lyme Arthritis?
Following antibiotic therapy, approximately 90% of late Lyme arthritis patients recover from extensive joint swelling, arthritis, and pain.
What happens if a patient doesn’t recover from Late Lyme Arthritis?
After extensive antibiotic treatment, approximately 10% of late Lyme arthritis patients remain symptomatic with a condition termed antibiotic refractory late Lyme arthritis. Extensive research has shown that the bacteria can no longer be found in the tissue or fluid of this subgroup of patients. Their continued swelling of the joints and pain is thought to be perpetuated by their own immune system’s autoimmune condition. Their autoimmunity continues to inflame the tissues and cause swelling and pain even in the absence of detectable bacteria.
Why are patients often referred to the Center?
Patients are often referred to the Lyme Disease Research Center for evaluation of chronic Lyme disease, an umbrella term that encompasses many different subsets of illness. Examples of defined Lyme disease subsets are Post Treatment Lyme Disease Syndrome (PTLDS), and Antibiotic Refractory Late Lyme Arthritis. The mechanisms of these Lyme disease conditions are different and effective treatments need to be tailored accordingly.
The symptoms of chronic Lyme disease are similar to and overlap with other conditions involving fatigue, pain, and cognitive symptoms. Therefore, rigorous diagnostic evaluation is necessary to determine if Lyme disease could be the trigger for ongoing disease processes or if some other disease processes are involved.
By distinguishing subsets of Lyme disease, such as PTLDS, our research program is illuminating the pathophysiology of the illness to improve diagnostics, treatments, and quality of life for patients.
USE OF THIS SITE
All information contained within the Johns Hopkins Lyme Disease Research Center website is intended for educational purposes only. Physicians and other health care professionals are encouraged to consult other sources and confirm the information contained within this site. Consumers should never disregard medical advice or delay in seeking it because of something they may have read on this website.
___________________
**Comment**
Overall, a balanced and accurate article. A few points for consideration:
I like how the author states that, “for research purposes a defined subset of this condition is called Post Treatment Lyme Disease Syndrome (PTLDS).” What’s important to understand is that this defined subset only includes patients who are diagnosed and treated early who go on to develop persistent symptoms. It does not and should not include those who were undiagnosed and untreated for months to years, which one microbiologist states is 30-40%. By adding the two groups, a whopping 60% go onto develop chronic symptoms. To date, researches are utilizing the falsely skewed 10-20% which isn’t based in reality: https://madisonarealymesupportgroup.com/2019/02/25/medical-stalemate-what-causes-continuing-symptoms-after-lyme-treatment/ This important fact indicates the pressing importance of this neglected group that nobody is noticing.
Please note that the top reason for patients to develop PTLDS is delayed diagnosis, yet the CDC/IDSA keep pushing their worthless tests and taking a “wait and see” approach. This tactic hasn’t worked for over 40 years yet they continue to blindly recommend this. It’s laughable if it wasn’t so serious.
There are far more patients with neurological involvement than mainstream medicine has a clue of.
I’m thankful the author states that one reason for PTLDS could be persistent bacterial infection or bacterial debris. Mainstream medicine and authorities STILL are not acknowledging this. I’m also thankful they state that PTLDS is a serious and impairing condition. Now, they need to acknowledge that 60% or more suffer with this, with corresponding prioritized research reflecting the vast numbers.
The authors state that there are, “no FDA approved treatments for Post Treatment Lyme Disease Syndrome; therefore, treatments must be individualized by addressing specific symptoms and circumstances for each individual.” Since this is true, why are Lyme doctors STILL being persecuted for treating people individually and outside the CDC guidelines of 21 days of doxycycline and why won’t insurance cover it? Case in point: https://madisonarealymesupportgroup.com/2017/06/24/llmd-daniel-cameron-disciplined-by-ny-medical-authorities/ Within this article is another article in “Sciencebasedmedicine.org,” that states, “Chronic Lyme” VIP Daniel Cameron Discipled by New York Medical Authorities. The title alone should be a foreshadowing of the type of ad hominem attacks against Lyme literate doctors for decades. Expert: “He is not a “recognized leader” among board-certified infectious diseases doctors and other experts who agree that “chronic Lyme” is not a real disease and who rely on well-conducted trials showing that long-term antibiotics do not substantially improve the outcome for patients diagnosed with so-called “chronic Lyme.” Long-term antibiotics can, in fact, result in serious harm, including death, a subject our good friend Orac covered just yesterday over on Respectful Insolence. The CDC, the Infectious Diseases Society of America (IDSA), the American Academy of Pediatrics, the American College of Physicians, the Medical Letter and the American Academy of Neurology all reject the notion that “chronic Lyme” exists and that long-term antibiotics are an appropriate treatment.(Orac’s post nicely summarizes the differences between real Lyme disease and “chronic Lyme,” “a prototypical fake medical diagnosis,” and the dangers of long-term antibiotics, as have posts on SBM, here, here, here, and here.)”
Malicious articles such as the one above which strangely chastises Cameron for not being a “recognized leader” which means part of the “Good old boy club,” among infectious disease doctors is a bit ironic when you consider that due to serious medical abuse, patients have been FORCED to go to doctors willing to listen to them to perhaps learn something new. The “well conducted” clinical trials don’t exist. There’s serious flaws with each of them. And people HAVE improved immensely using long-term antibiotics. Case in point: https://madisonarealymesupportgroup.com/2017/07/09/idsa-founder-used-potent-iv-antibiotics-for-chronic-lyme/Excerpt: A founding member of the IDSA, Dr. Waisbren disagreed with their stance that Lyme is hard to get and easy to treat, is not persistent, and that IV antibiotics are too dangerous to use as a treatment option. In his book, “Treatment of Chronic Lyme Disease,” he discusses 51 difficult cases, nearly all Chronic Lyme disease sufferers that had been misdiagnosed with everything from ALS to mental disorders. They had all been neglected by main stream medicine that was following the CDC/IDSA stringent guidelines of essentially 21 days of doxycycline. BTW: Waisbren’s book was written nearly a decade ago yet the IDSA/CDC infectious disease “leaders” haven’t learned a thing and continue to live in the Stone Ages.