‘The Proof is in the Pudding” My Letter to the TBDWG
They say, The proof is in the pudding.
 My husband and I, and thousands of others have regained our health due to extended antibiotic treatment.
My husband and I, and thousands of others have regained our health due to extended antibiotic treatment.
My name is Alicia Cashman and I run the Madison Lyme Support Group in Wisconsin.
Our dog became infected first, then my husband, then me. While our dog was put on a month’s worth of antibiotics (which is more than the CDC recommends for people) my husband and I languished, undiagnosed and untreated for years. Formerly an avid runner, my husband was reduced to playing Candy Crush on the couch in his robe. He wouldn’t admit there was a problem until he fell down the stairs. Meanwhile, I ignored my gynecological symptoms until they metastasized systemically, as he appeared far worse.
Trying to find answers to our spiraling health, I explained our multiple migrating & relapsing symptoms to my kids’ coach, who said,
“This sounds like a page out of my book. I was just diagnosed with Lyme disease.”
This new information sent me on a quest that has never ended.
In my experience, this is how people finally get answers to their perplexing health deterioration: from other experienced patients. Due to the ignorance of mainstream medicine which follows antiquated and biased science which relies heavily on abysmal testing that misses over 70% of cases, and in this case 86%, where patients rarely test positive, and if they do manage to ‘win the lotto’ with a positive, they are told it’s a false positive. A local woman called me yesterday with this exact scenario testing positive THREE times, but was told it was a false positive and was sent packing.
It’s a damned if you do, damned if you don’t situation where patients continue to lose.
The ugly history behind testing is something from a science fiction novel, only it’s very real. There’s been a concerted effort to suppress direct diagnostic tests, and questions go unheeded. There’s currently a $58.1 million lawsuit against the CDC for using its regulatory power to block application of a highly reliable direct DNA test and for channeling public funds to promote their own patented tests.
We are forced to seek help where we can find it due to this unscientific dogma which borders on the absurd.
Even though the history of tick-borne illness dates back to the 1800’s, working knowledge remains infantile, and having just read Polly Murray’s work, The Widening Circle, very little has changed in over 40 years. The issue of persistent infection continues on unabated, yet continues to be experienced by patients worldwide.
Due to our lives and health dissolving in front of our very eyes, we in Lyme-land learn quickly if we want to get our health back we need to go outside mainstream medicine which continues in this endless juggernaut due to the severe conflicts of interest of our public ‘authorities’, whom have rigged the diagnostic test for their own patent purposes and continue to control a narrative keeping people from proper diagnosis and treatment – which includes what is being taught in medical schools.
These are simple verifiable facts.
We also suffer due to mainstream medicine’s simplistic germ theory that doesn’t match our symptom picture at all; mainly that we are typically infected with far more than just borrelia, the causative agent of Lyme disease. Garg et al. not only show the polymicrobial (multiple pathogens) nature of the disease(s) but the fact borrelia is pleomorphic (shape-shifts); facts the chronic Lyme deniers continue to ignore.
These two issues are at the crux of understanding of Lyme/MSIDS – or multi systemic infectious disease syndrome.
Further, mythology abounds:
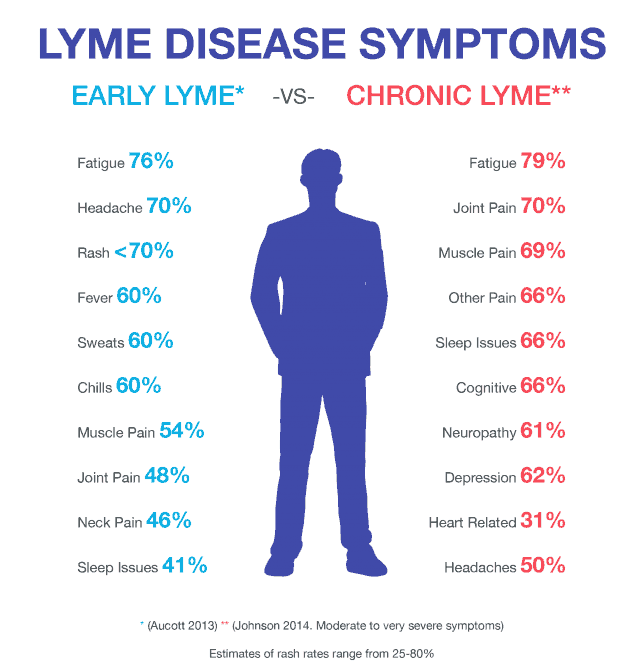
- We are are told nearly 80% get the “classic” bullseye rash, when it is highly variable and not “classic” at all. This is problematic not only from a diagnostic stand point but because having the EM rash is often entrance criteria into research studies. By utilizing this criteria, as well as only accepting positive 2-tiered serology, studies are omitting a huge subset of patients – probably the sickest ones.
- We are told that only 10-20% go onto develop symptoms after treatment, when it’s more like 40-60% when you count those that were diagnosed and treated late (nearly everyone I deal with).
- We are continually told things are “rare,” only to have information quietly updated later.
- We are continually told Lyme/MSIDS can’t be in certain locations only to be told later it exists after denying thousands treatment.
- Southern patients have been fighting for decades to be properly diagnosed and treated but have been ruled by Andrew Speilman’s Iron Curtain.
- Researchers continue to use the popular “climate change” moniker in their work, eating up precious research dollars, when independent research has proven tick proliferation to be caused by migrating birds and photo-period. Ticks laugh at the weather. Rather than answering the very real question of the bioweaponization of ticks being dropped from airplanes, public ‘authorities’ continue a slight of hand by pushing the climate agenda.
- We continue to be told Lyme/MSIDS can’t be spread sexually when research and experience indicates it can be. We were told it didn’t occur congenitally, yet much research and experience shows otherwise.
Wisconsin has a long history of tick-borne illness with many experienced doctors. Dr. Waisbren, an IDSA founder and Wisconsin physician, disagreed with his colleagues and successfully used high dose IV antibiotics for those with chronic Lyme disease.
“I have to come to the conclusion that there is an epidemic of chronic Lyme disease occurring in the United States that warrants more attention than it is getting from the government and the academic medical establishment. It is hard for me to believe that 51 cases of what I call the chronic Lyme disease syndrome represent a figment of my imagination….I suggest that those who doubt that the Lyme disease syndrome exists and that it can be treated turn to the over 200 peer-reviewed references included in summary articles written by two giants in the Lyme disease field: Dr. B.A. Fallon and Dr. Steven Phillips.” Dr. Waisbren
If Waisbren thought chronic Lyme disease was an epidemic in 2011, what would he think now?
And what about those peer reviewed references showing chronic infection? Why are they continually ignored? Here’s over 700.
The reason chronic Lyme/MSIDS is the crucial issue to be addressed is because there are thousands upon thousands that continue with severe symptoms after the outdated and unscientific CDC mono-therapy.
Biased, poorly done research on this issue states that further treatment doesn’t help yet my husband, myself, and countless others prove that axiom to be completely wrong.
Thankfully, ILADS trained doctors despite being persecuted, listen to patients, defy the accepted narrative, and are willing to treat longer and with numerous antimicrobials to address the often present coinfections. After-all, relapses have occurred in nearly every single antibiotic study ever done.
Treatment for this complex illness takes a savvy nuanced approach. My husband and I are living proof that a judicious use of antibiotics is not only effective but safe if done correctly. Antibiotics are only part of a multi-pronged approach in treating this beast. I suggest you listen to the thousands of ILADS trained doctors and other professionals rather than vilifying them.
I often shutter when I consider what would have happened had we remained under a doctor adhering the CDC guidelines which mainstream medicine follows as a literal mandate. We very well might be dead as we both had heart involvement.
Research for Lyme/MSIDS has only progressed by being independently done.
Lastly, I would like to include some quotes:
“The presence of live spirochetes in a genital lesion strongly suggests that sexual transmission of Lyme disease occurs,” said Middelveen. “We need to do more research to determine the risk of sexual transmission of this syphilis-like organism.” Marianne Middelveen, PhD
“I AM CONVINCED THAT LYME DISEASE IS TRANSMITTABLE FROM PERSON TO PERSON.” Lida Mattman PhD
“We never had in the last five years a single MS patient, a single ALS patient, a single parkinson’s patient, who did not test positive for Borrelia burgdorferi. Not a single one. Dr. Dietrich Klinghardt
“The CDC is responsible for the current Lyme disease crisis where patients cannot obtain a timely diagnosis through accurate early detection.” Lyme patient and advocate Carl Tuttle
“The people who test positive are ironically the ones who really aren’t sick other than a bad knee (Lyme arthritis). This is how after the Dearborne conference, where the case definition was fraudulently changed to a very narrow set of criteria that lyme came to be associated with arthritis, namely an arthritic knee, when in reality that is the very least of the symptoms most lyme patients encounter.
I liken the two tiered testing for lyme to giving a blind person a vision test then telling them they can see – it’s madness!” Malia McClean
The ongoing and prolific conflicts of interest impede our public ‘authorities’ from making wise public health decisions. The fact that only ONE patient representative is on the TBDWG succinctly proves my point.
Prove me wrong.