A Blind Spot on Autism
https://www.lymedisease.org/autism-infectious%E2%80%91disease-lens/
Looking at autism through an infectious‑disease lens
The following excerpt comes from A Blind Spot on Autism. The book is co‑authored by Debbie Kimberg, a mother and advocate whose writing for LymeDisease.org has chronicled her son’s improvement after treatment for vector‑borne infections including Borrelia, Bartonella, and Babesia. She partners with Dr. Ed Breitschwerdt, one of the world’s leading Bartonella researchers. Together, they blend lived experience and scientific expertise to explore biological patterns they believe have been overlooked in autism research.
By Debbie Kimberg and Dr. Ed Breitschwerdt
Article Excerpts:
From the moment we step into a doctor’s office, we’re taught to think of health problems as separate boxes. A child’s learning issues go to a specialist for educational testing. A sibling’s anxiety is treated by a mental health professional. A parent’s autoimmune disease is managed by a rheumatologist. A grandparent’s memory loss goes to neurology.
Medicine is organized this way.
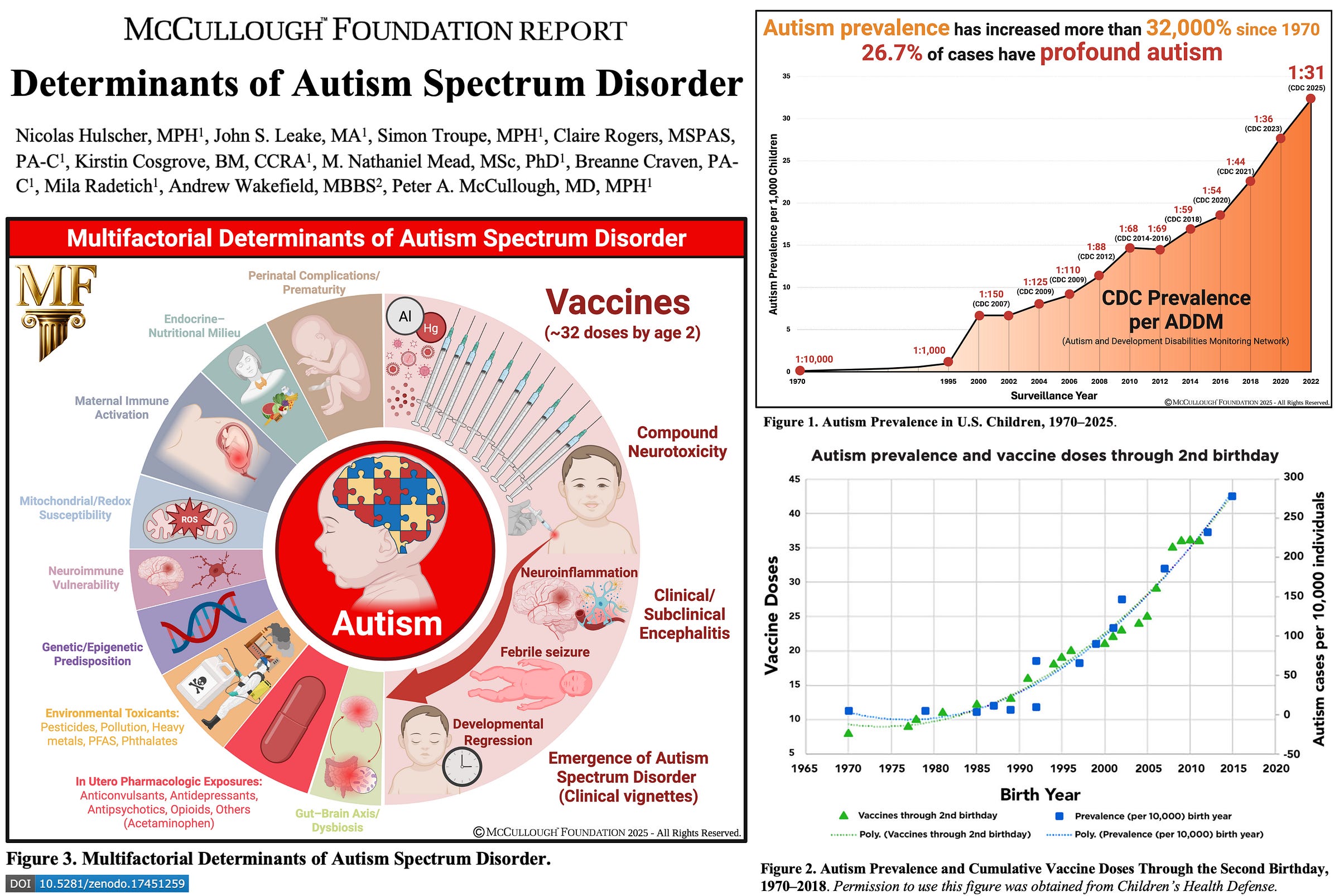
This book brings together two perspectives rarely combined: the lived experience of navigating these patterns as a parent and patient advocate, and the decades of research from one of the world’s leading infectious disease experts. Our goal is not to dismiss the work already done on autism, but to attempt to connect the dots between existing research that has remained scattered across a thousand scientific papers, often among different fields of study. When viewed together, these studies point toward a hypothesis that could explain both the near-exponential rise in autism cases and the convoluted web of health problems in so many families.
This is not the first time medicine has been blindsided by an invisible infectious cause. History is full of examples where an infectious trigger hid in plain sight for decades before science caught up. Syphilis was once thought to be a mysterious neurological illness, ulcers were blamed on stress, and HIV was first recognized only by its complications. Each time, the truth emerged slowly, in pieces, and often against the resistance of the medical establishment.
….Bartonella species may represent one of the most stealth and dangerous pathogens seen in generations, pathogens that have been allowed to spread silently, reshaping the health of millions without recognition. (See link for article & ordering info)
_____________
**Comment**
Sadly, autism is only one such illness with an infectious connection. In this study, it was found that 92% of pediatric bip0lar disorder had tick-borne infections exposure. PANS is connected with Lyme and mycoplasma.
For more:
- https://madisonarealymesupportgroup.com/2025/04/30/autism-guide/
- https://madisonarealymesupportgroup.com/2023/09/08/case-report-substantial-improvement-of-autism-in-child-by-using-treatment-for-vector-borne-infections/
- https://madisonarealymesupportgroup.com/2022/07/19/does-unrecognized-lyme-in-mothers-lead-to-autism-spectrum-disorder/
- https://madisonarealymesupportgroup.com/2019/01/07/the-vaccine-debate-top-government-expert-states-vaccines-can-cause-autism-in-some-children/
- https://madisonarealymesupportgroup.com/2023/03/20/when-treating-bartonella-clears-symptoms-of-autism-what-next/
- https://madisonarealymesupportgroup.com/2025/10/27/landmark-study-vaccination-is-the-dominant-risk-factor-for-autism/
- https://madisonarealymesupportgroup.com/2025/11/20/cdc-quietly-rewrites-its-vaccine-autism-guidance-where-does-their-dishonesty-come-from/
- https://madisonarealymesupportgroup.com/2021/08/13/its-a-gene-environment-immune-complex-how-mycotoxins-impact-lyme-autism-and-pans/