It’s confirmed. The tick from hell has been found on a hawk in Virginia.
This Asian “dracula” tick causes SFTS (severe fever with thrombocytopenia syndrome), “an emerging hemorrhagic fever,” causing fever, fatigue, headache, nausea, muscle pain, diarrhea, vomiting, abdominal pain, disease of the lymph nodes, and conjunctival congestion, but the potential impact of this tick on tickborne illness is not yet known. In other parts of the world, this Longhorned tick, also called the East Asian or bush tick, and has been associated with several tickborne diseases, such as spotted fever rickettsioses, Anaplasma, Ehrlichia, and Borrelia, the causative agent of Lyme Disease. https://madisonarealymesupportgroup.com/2018/06/12/first-longhorned-tick-confirmed-in-arkansas/
“I think I’m losing this battle,” the 58-year-old man told his wife one Saturday night nearly a year ago.
While she was at the theater — they’d bought the tickets months earlier — he had to crawl up the stairs on his hands and knees to get to bed. Terrible bone-shaking chills racked him, despite the thick layer of blankets. The chills were followed by sudden blasts of internal heat and drenching sweats that made him kick off the covers — only to haul them back up as the cycle repeated itself.
“I need to go to the E.R.,” he told his wife. He’d been there three times already. They’d give him intravenous fluids and send him home with the diagnosis of a viral syndrome. He would start to feel better soon, he was told. But he didn’t.
Too Sick to Work
This all began nine days before. That first day he called in sick to his job as a physical therapist. He felt feverish and achy,as if he had the flu. He decided to drink plenty of fluids, take it easy and go back to work the next day. But the next day he felt even worse. That’s when the fever and chills really kicked in. He was alternating between acetaminophen and ibuprofen, but the fever never let up. He’d started sleeping in the guest room because his sweat was soaking the sheets, and his chills shook the bed, waking his wife.
After three days of this, he made his first visit to the Yale New Haven Hospital emergency room. He was already taking antibiotics. Several weekends earlier, he developed a red, swollen elbow and went to an urgent-care center, where he was started on one antibiotic for a presumed infection. He took it for 10 days, but his elbow was still killing him. He went back to urgent care, where he was started on a broader-spectrum drug, which he had nearly finished. Now his elbow was fine. It was the rest of his body that ached as if he had the flu.
But at the hospital, his flu swab was negative. So was his chest X-ray. It was probably just a virus, he was told. He should take it easy until it passed. And come back if he got any worse.
High Fever
The next day his fever spiked above 105. He went again to the E.R. It was a mob scene — crowded with people who, like him, appeared to have the flu. It would be hours before he could be seen, he was told, because they already knew he didn’t have it. Discouraged, he went home to bed. He went back the next morning after a nurse called to say the E.R. was more manageable.
He might not have the flu, he thought, but he was sure he had something. But the E.R. doctor didn’t know what. He didn’t have chest pain or shortness of breath. No cough, no headache, no rash, no abdominal pain, no urinary symptoms. He felt weak but no longer achy. His heart was beating hard and fast, but otherwise his exam was fine. His white count was low — which was a little strange. White blood cells are expected to increase with an acute infection. Still, a virus can cause white counts to drop. His platelets — the tiny blood fragments that form clots — were also low. That can also be seen in viral infections, but it was less common.
No Help From His Internist
The E.R. staff sent the abnormal blood results to the patient’s primary-care provider and told the patient to follow up with him. He’d been trying get in to see him for days, but the doctor’s schedule was full. When he called again, he was told that the soonest he could be seen was the following week.
The patient asked the doctor to order blood tests to look for an infection in his blood. And could they also test him for tick-borne infections? This was Connecticut, after all. He dragged himself to the lab and then waited for his doctor to call with the results. The call never came. In his mind, he fired his doctor. He’d been sick for over a week, and the doctor’s office couldn’t arrange an appointment, and they couldn’t even call him with the lab results for the test he had to ask for in the first place.
Back to the Hospital
That Sunday morning after the man’s wife had been to the theater, he went once more to the emergency room. It was brought to the attention of the physician assistant on duty that the man had been there several times before and had lab abnormalities. She ordered a bunch of blood tests — looking for everything from H.I.V. to mono. She ordered another chest X-ray and started him on broad-spectrum antibiotics, as well as doxycycline, an antibiotic often used for tick-borne infections. He was given Tylenol for his fever and admitted to the hospital. As he was preparing to leave the emergency department, a new flu test came back positive. He was pretty sure he didn’t have it; he’d never heard of a flu being this bad for this long. But if he could stay in the hospital, where someone could monitor him, he was happy to take Tamiflu.
The lab called again the next day to say that the test had been read incorrectly; he did not have the flu. By then other results started to come in. It wasn’t an infection in his elbow. He didn’t have H.I.V.; he didn’t have mono or Lyme; he didn’t have any of the other respiratory viruses that, along with the worse influenza outbreak in years, had filled up so much of the hospital.
CreditIllustration by Andreas Samuelsson
Getting Better
Yet after a couple of days, the patient began to feel better. His fever came down. The shaking chills disappeared. His white count and platelets edged up. It was clear he was recovering, but from what? More blood tests were ordered, and an infectious-disease specialist consulted.
Gabriel Vilchez, the infectious-disease specialist in training, reviewed the chart and examined the patient. He thought that the patient most likely had a tick-borne infection. The hospital had sent off blood to test for the usual suspects in the Northeast: Lyme, babesiosis, ehrlichiosis and anaplasmosis. Except for the Lyme test, which was negative, none of the results had come back yet. Vilchez considered that given the patient’s symptoms — and his response to the doxycycline — it would turn out that he’d have one of them.
And yet, the results for tick-borne infections were negative. Vilchez thought about other tick-borne diseases that are not on the usual panel. The most likely was Rocky Mountain spotted fever (R.M.S.F.).The name is a misnomer: R.M.S.F. is much more common in the Smoky Mountains than the Rocky Mountains, and the spotted-fever part, the rash, is not seen in all cases. It’s unusual to acquire the infection in Connecticut but not unheard-of. Vilchez sent off blood to be tested for R.M.S.F. The following day, the patient felt well enough to go home. A couple of days later, he got a call. He had Rocky Mountain spotted fever.
A Diagnostic Delay
Why did the diagnosis take so long? The patient had an unusual infection. But perhaps the bigger issue was that he was one of many patients in the emergency room with flulike symptoms in the midst of a flu epidemic. Under those circumstances, the question for the staff simply becomes: Does he have the flu? When the answer is no, doctors tend to move on to the next very sick patient in line. It’s hard to get back to the question of what the nonflu patient does have.
For the patient, recovery has been tough. Though the antibiotic helped with the acute symptoms, it took months before he had the stamina to resume his usual patient load at work. He feels that the illness brought him as close to dying as he had ever been. Indeed, Rocky Mountain spotted fever is one of the most dangerous of all the tick-borne infections, with a mortality rate as high as 5 percent even with current antibiotics.
One thing he was certain about, however: He needed a new primary-care doctor. And he got one.
Lisa Sanders, M.D., is a contributing writer for the magazine and the author of “Every Patient Tells a Story: Medical Mysteries and the Art of Diagnosis.” If you have a solved case to share with Dr. Sanders, write her at Lisa.Sandersmd@gmail.com.
________________
**Comment**
This is playing out all over the world. He was one of the lucky ones to finally get an accurate diagnosis.
It is interesting; however, that they are quick to state he doesn’t have the other tick-borne infectionswhen the testing for all of them misses over half of all cases. Once they gave him doxy, they should have retested him. This is called a “provocation test” and is used by many LLMD’s (Lyme literate doctors) as they’ve learned this often finally shows an active infection(s) due to the ability of the body to NOW see the pathogens in the blood stream allowing antibodies to be made and picked up by the tests.
RMSF is a nasty beast on it’s own; however, this man should be monitored over time. If symptoms come back or new ones show up, TBI’s should be suspected.
It’s also a mind boggler how in Connecticut of all places, TBI’s wouldn’t be the FIRST thing medical practitioners think of. It’s literally ground zero.
It’s also been found to be spread by the common brown dog tick:
https://madisonarealymesupportgroup.com/2018/08/16/new-tick-causes-epidemic-of-rmsf/ It’s usually spread by the American dog tick and the closely related Rocky Mountain wood tick. But in recent years the bacterial infection has also been spread by the brown dog tick — a completely different species…The researchers were investigating an epidemic of the infection that broke out in the border town of Mexicali starting in 2008. It’s already sickened at least 4,000 people, according to Mexican government estimates. Several hundred have died, and at least four people have died in the U.S. after crossing the border, according to this report and others.
“I was absolutely startled,” Foley said in an interview.
The people who had been sickened in Mexicali had a heavy load of the infectious agent in their blood — something that had not been seen in past outbreaks. The epidemic is worrisome because the brown dog tick is more likely to bite people and it adapts easily to living in a house, as opposed to living on wild animals, the researchers said.
“The Rocky Mountain spotted fever epidemic in Mexicali has not been contained and may be spreading to other parts of Baja California and into the United States,” the team wrote.
And now it’s possible that for some reason, the infection the brown dog tick transmits is more virulent, Foley said.
https://madisonarealymesupportgroup.com/2017/10/21/mom-got-rocky-mountain-spotted-fever-while-picking-pumpkins/ “When you go to these pumpkin patches and petting zoos and all those fun fall activities, wear pants, long socks and shoes!” “Make sure you check for tics! This was me 2 years ago after being bit by a tick and contracting Rocky Mountain spotted fever at a pumpkin patch,” she continued. “I couldn’t walk, my whole body was in pain, my hair fell out, and I almost died.”
My journey was similar with the same issue in both my elbow and knee in the middle of January in Wisconsin. I was told, and I promise I didn’t make this up, that I had “Washer Woman’s Knee,” and “Barstool elbow.”
I kid you not.
Now, first, I use a mop and rarely get on my knees. Second, I assure you, I’m not sitting at the bar and have NO reason to have a red, swollen, excruciatingly painful elbow.
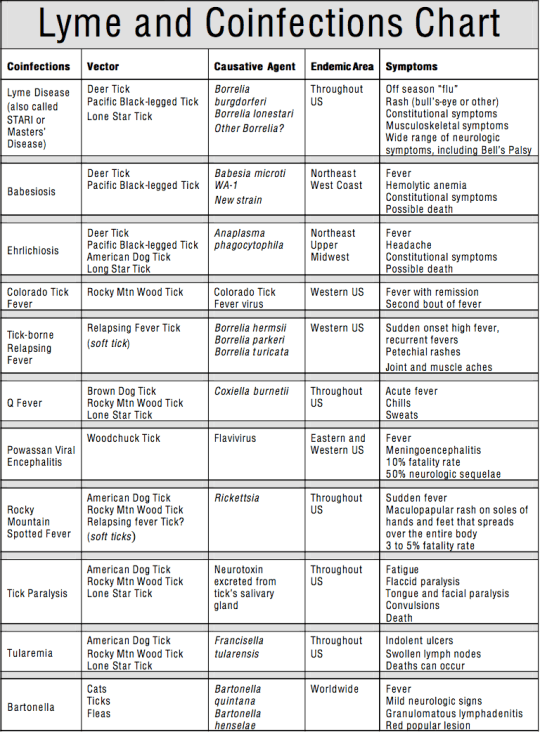
Please remember, Lyme is the rock star we all know by name. There are many, many other players involved and people are often coinfected. Mainstream medicine has yet to accept and deal with this very real fact.
A group of 14 persons who live in an area of Australia endemic for the Australian paralysis tick, Ixodes holocyclus, and who were involved in regularly collecting and handling these ticks, was examined for antibodies to tick-transmitted bacterial pathogens.
Five (36%) had antibodies to Coxiella burnetii, the causative agent of Q fever and three (21%) had antibodies to spotted fever group (SFG) rickettsiae (Rickettsia spp). None had antibodies to Ehrlichia, Anaplasma, Orientia, or Borrelia (Lymedisease) suggesting that they had not been exposed to these bacteria.
A total of 149 I. holocyclus ticks were examined for the citrate synthase (gltA) gene of the SFG rickettsiae and the com1 gene of C. burnetii; 23 (15.4%) ticks were positive for Rickettsia spp. and 8 (5.6%) positive for Coxiella spp. Sequencing of fragments of the gltA gene and the 17 kDa antigen gene from a selection of the ticks showed 99% and 100% homology, respectively, to Rickettsia australis, the bacterium causing Queensland tick typhus.
Thus, it appears that persons bitten by I. holocyclus in NE NSW, Australia have an approximate one in six risk of being infected with R. australis.Risks of Q fever were also high in this region but this may have been due to exposure by aerosol from the environment rather than by tick bite. A subset of 74 I. holocyclus ticks were further examined for DNA from Borrelia spp., Anaplasma spp. and Ehrlichia spp. but none was positive. Some of these recognised human bacterial pathogens associated with ticks may not be present in this Australian tick species from northeastern New South Wales.
While they still deny Lyme (borrelia) this recent study definitively shows a number of pathogens in Australian ticks and humans including Rickettsia (more commonly known as Tick & arthropod Typhus, Queensland typhus or Rickettsia australis), as well as Q Fever.
Tick Typhus is similar to Rocky Mountain spotted fever, but deemed not as severe. Symptoms include:
Fever
Headache
Malaise
Bloodshot eyes
Red lump at tick bite site
Ulceration at tick bite site
Black scab at tick bite site
Enlarged local lymph nodes
Forearm red rash
Red body rash
Palm rash
Rash on soles of feet
Doxycycline is the front-line drug for typhus and broad-spectrum antibiotics aren’t helpful.
Caused by the bacteria Coxiella burnetii, it can cause pneumonia and hepatitis (liver inflammation) in its early stage, and infection of the heart valves (endocarditis) in its chronic stage. Perps are the Brown Dog Tick (Rhipicephalus sanguine us), Rocky Mountain Wood Tick (Dermacentor andersoni), and the Lone Star Tick (Amblyomma americium).
https://coloradoticks.org/tick-borne-diseases/q-fever/ This article states it’s usually a mild disease with flu-like symptoms but sometimes it can resurface years later. This more deadly, chronic form, of Q fever can damage heart, liver, brain and lungs. C. burnetii is highly infectious. Humans that are susceptible to this disease can be infected by a single organism. It is considered a significant threat for bio warfare and is classified as a Category B agent of bioterrorism.
The severity and combination of signs and symptoms vary greatly. About half the people infected with Q fever will get sick. Symptoms include:
High fever (up to 105°F)
Fatigue
Severe headache
General malaise
Myalgia
Chills or sweats
Non-productive cough
Nausea
Vomiting
Diarrhea
Abdominal pain
Chest pain
Doxycycline is also the front-line drug for this with quinolone antibiotics as an alternative.
Add the Ixodes holocyclus tick to this list as well.
And before you think it can only ever be in Australia, this article in the 2013 issue of the Australian Veterinary Journal shows the likelihood of a population of Ixodes holocyclus breeding outside their common range. https://conference.ava.com.au/13097.
August, 2018: Nymphal deer ticks are less abundant but still active in Wisconsin right now. About 20-25% of nymphs are infected with the Lyme spirochete. Overall, 2018 has been normal in terms of tick numbers.
Live in Wisconsin and want your tick identified?
NEW for 2018: Page over to check out the Tick App, http://labs.russell.wisc.edu/wisconsin-ticks/the-tickapp/our new tool for studying tick exposure and providing mobile information about ticks and tick-borne disease. More than 600 Wisconsinites have already participated in 2018.
NEW for 2018: We are starting a tick identification service. Identifying the stage and species of a tick are crucial to deciding whether to seek medical attention or not. Tick-borne diseases are only carried by certain ticks in specific regions. We can help you identify the tick you’ve found based on your images and geographical location. Use the following link to submit your photos and information:
Go to link for pictures and information on each. There are 4 ticks listed including the Lone Star Tick, which was until recently considered a Southern tick but is here as well. Wisconsin had its first RMSF death, transmitted by the Lone Star Tick, recently: https://madisonarealymesupportgroup.com/2018/07/10/first-rmsf-death-in-wisconsin/
There is also a tab titled “Tick-Borne Diseases.” Go to link to read about them. They give WI stats as well. Please remember ALL the numbers are low as many go unreported:
Lyme (Bb or Bm)
Borrelia miyamotoi (relapsing fever)
Anasplasmosis
Ehrlichia muris eauclairensis (EML)
Babesiosis
Powassan virus/deertick virus
Ehrlichia chaffeensis
Rocky Mountain Spotted Fever
__________________
A few points stick out to me:
Please take pictures of these ticks & send them in so we finally have an accurate record. They are asking us for help so let’s give it. It will only help us in the end. Flood them with ticks!
Baronella didn’t make the list, yet nearly everyone I work with has it. WHY? Because while Bart has been found in ticks, it hasn’t been proven conclusively they transmit. Bart is a nasty, nasty bug and alone can kill you. Coupled with Lyme it can make you want to die.
The lack of data is glaring. Seriously. Glaring. Zika makes front page news here and our mosquitoes can’t even carry it. https://madisonarealymesupportgroup.com/2018/03/13/wed-nite-the-lab-talk-on-mosquitoes-ticks-disease/ There were only 46 cases of Zika in the U.S. in 2018 – ALL due to travelers returning from affected areas.The CDC “estimates” that there are 300,000 NEW Lyme Disease cases annually in the U.S. Anyone see a disparity here between Zika and Lyme? (Other tick-borne diseases aren’t even on the radar yet)
Positive cases of Lyme, Anaplasmosis, and Ehrlichiosis in dogs have been documented in Colorado over the past 6 years as shown in prevalence maps compiled by the Companion Animal Parasite Council, and the cases for of these diseases have increased annually. Although dogs are at greater risk of contact with ticks based on their behavior, they frequently travel and recreate with their owners. Dogs may be both host and victim to many tick-borne diseasesin Colorado, and can increase risk of exposure to ticks for their owners. There are gaps of information regarding tick species distribution, prevalence, infection rates and disease surveillance in humans within Colorado, making the CAPC data a great resource of information. Protecting your pets from exposure to ticks is the best way to prevent these diseases.