“Southern Charm” star Olivia Flowers shared how her brother, Conner Flowers, battled Lyme disease for nearly two decades before he died in January at age 32.
“My brother suffered from this insidious disease for his entire adult life,” Olivia, 31, captioned an Instagram post Tuesday.
The Bravolebrity explained that Conner kept his “struggles” with the disease “very private,” but she and her family “saw the toll it took on his life trying to navigate the debilitating symptoms over the last 17 years.” (See link for video and article)
________________
**Comment**
Yet another patient with several misdiagnoses and medical treatment that didn’t address the underlying infection(s) who succumbed.
Ultimately, these issues boil down to human rights abuses. What has been going on domestically and worldwide needs to be viewed in that light. Those who have engaged in systematic medical neglect of persons with chronic Lyme disease need to be ‘called out’ and ‘called to account’. ~ Dr. Kenneth Liegner
I post this for two reasons: 1) it reveals the severe conflicts of interest in medicine today and shows advice from doctors can not be blindly followed 2) vaccines can serve as triggers to reactivate latent infections and autoimmune issues. Since Lyme/MSIDS patients are already in an epic war in which they are attempting to maintain immune balance, they need to understand a vaccine could serve to tip this balance making it easier for pathogens to emerge or reemerge.
Primary care providers across the U.S. were bribed with incentive programs to coerce patients into getting the toxic COVID shot. Anthem Blue Cross and Blue Shield paid doctors $50 for each Medicaid patient aged 6 months and older, who got the experimental jab
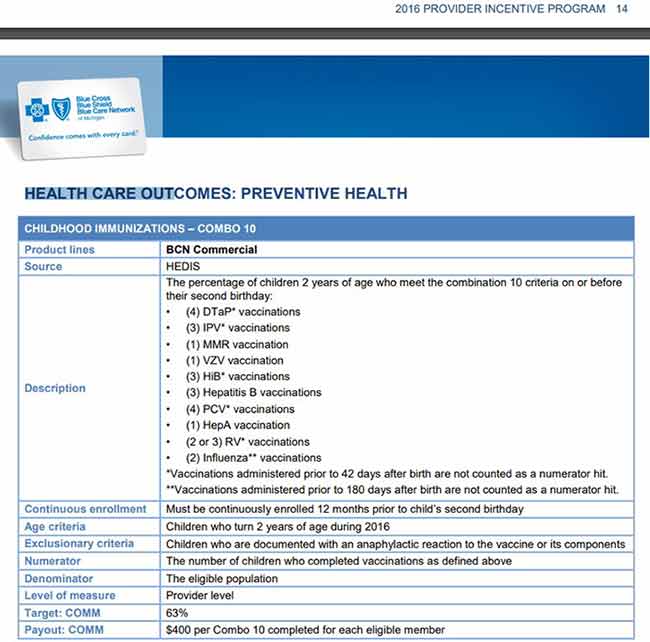
Doctors have been financially incentivized to vaccinate children for a long time. In 2016, Blue Cross Blue Shield paid pediatricians a $400 bonus for each patient that completed 10 vaccinations before their second birthday, provided 63% of their patients were fully vaccinated
“Client and family incentives” also exist. In 2015, the Community Preventive Services Task Force recommended boosting vaccination rates by giving small, inexpensive incentive rewards to patients
Bribery is also par for the course when it comes to vaccine mandates. Pfizer paid undisclosed sums to front groups that advocated for COVID jab mandates, thereby hiding their conflict of interest
While the COVID-19 pandemic furthered many globalist goals, it inadvertently tanked childhood vaccination rates. To get childhood vaccination rates back on track, a global alliance has launched “The Big Catch-Up” initiative. It’s touted as the largest childhood immunization effort ever
In April 2023, I reported how primary care providers across the U.S. were bribed with incentive programs to coerce patients into getting the toxic COVID shot. Since there was no medical malpractice liability, doctors profited while patients risked their lives as participants in an unprecedented medical experiment, all while being lied to about the safety and effectiveness of these injections.
Even more egregiously, once the U.S. Food and Drug Administration authorized the COVID shot for children, similar vaccination incentives were extended to pediatricians as well. As detailed in an Anthem Blue Cross and Blue Shield Medicaid provider bulletin1 dated July 2022, doctors received $50 for each Medicaid patient aged 6 months and older, who got the experimental jab.
Pediatricians Are Financially Incentivized to Vaccinate
As it turns out, doctors have been financially incentivized to vaccinate children for a long time. According to a 1999 JAMA Pediatrics article,2 the average patient load of American pediatricians is 1,546, although the number of patients was “significantly higher in less populated areas and solo practices.”
Of these, 8.3% were younger than 1 year, 9.5% were 1 year old and 8.6% were 2 years old.3 That means approximately 26.4% of the average pediatrician’s patients were 2 years old and younger. More recent data,4 published in 2021, show 75% of pediatricians have between 1,000 and 1,800 patients and 21% have around 1,200 patients; most practices, 65%, are in the 1,000 to 1,500 range.
As shown in the 2016 provider incentive program document from Blue Cross Blue Shield below,5,6 pediatricians were getting $400 for each pediatric patient that completed all the 10 vaccinations listed — 25 doses in all7 — before their second birthday. (Keep in mind that incentives can vary by state. The example provided is part of Michigan’s Blue Cross Blue Shield Performance Recognition Program.)8
How Much Money Is at Stake?
The math from there is pretty straight-forward (although keep in mind that we’re dealing with presumed averages and aged statistics here). Just multiply the number of patients under age 2 times $400. Using the average statistics from 1999, if a pediatrician has 1,000 patients, 264 can be expected to be 2 years old or younger. If all are fully vaccinated, the pediatrician would be eligible for a $105,600 year-end bonus.
While $400 per fully vaccinated child might seem incentivizing enough, there’s an added pressure here, because Blue Cross Blue Shield also has (or at least had, in 2016) a “target” level of 63%.
This means that if the pediatrician fails to vaccinate 63% of his eligible patients, he or she gets nothing. So, the pediatrician has a VERY high incentive to get as many toddlers fully vaccinated as possible, so as not to miss that target. It’s not just $400 that is at stake when parents decline one or more shots. Tens of thousands of dollars could be on the line. As noted by Dr. Bob Sears:9
“Such incentives … end up forcing a doctor to consider the financial implications of accepting patients who even just want to opt out of one vaccine … Maybe a few such families wouldn’t make them fail the chart reviews, but if they have too many, there goes their year-end bonus.”
Why Pediatricians Become Adversaries
Anytime financial incentives are part of the equation, one can reasonably assume that the lure of self-enrichment will win. With tens of thousands of dollars at stake, pediatricians can easily be lulled into complacency when it comes to digging deeper into the science.
After all, who wants to see evidence that what they’re doing is causing more harm than good? These kinds of incentives also encourage pediatricians to simply toss questioning parents out of their practice, to make room for more compliant patients that don’t put their income at risk. As reported by Children’s Health Defense back in 2018:10
“… the 11 well-child visits recommended by the AAP over a child’s first 30 months (with annual visits thereafter through age 21) ensure a steady stream of repeat customers and revenue for pediatricians.
In accordance with the Centers for Disease Control and Prevention’s vaccine schedule, pediatric practices are expected to administer vaccines (often as many as six at a time) at about half of well-child visits through the adolescent years, making vaccination a foundational bread-and-butter component of pediatricians’ job description …
It is quite common for pediatricians (and family doctors) to encounter parents who refuse one or more infant vaccines, most often due to safety concerns. These concerns also mean that pediatricians frequently get requests to modify or delay the vaccine schedule — nearly three-fifths (58%) of pediatricians reported such requests in a 2014 AAP survey …
Rather than recognize the validity of parents’ safety concerns or admit to their own ambivalence about some of the newer vaccines, many pediatricians — nearly two in five according to some estimates — choose to boot uncooperative families out of their practice …
Ultimately … subtle and not-so-subtle financial incentives and social pressures are likely to maintain widespread adherence by pediatricians to the vaccine schedule — even in instances where contraindications are present.
Although pediatricians have a legal duty to fully inform patients about vaccine risks and side effects, the lure of monetary perks and the desire to fit in may lessen their motivation to do so.”
Patients Are Bribed Too
In addition to the financial incentives given to physicians, “client and family incentives” also exist. A nongovernmental panel of public health and prevention experts called the “Community Preventive Services Task Force”11 in 2015 published a guide12 on how to boost vaccination rates using incentive rewards for patients.
The task force was established by the U.S. Department of Health and Human Services in 1996 “to develop guidance on which community-based health promotion and disease prevention intervention approaches work and which do not work, based on available scientific evidence.”13 As explained by this task force:14
“The Community Preventive Services Task Force recommends client or family incentive rewards, used alone or in combination with additional interventions, to increase vaccination rates in children and adults.
Client or family incentive rewards are used to motivate people to obtain recommended vaccinations. Rewards may be monetary or non-monetary, and they may be given to clients or families in exchange for keeping an appointment, receiving a vaccination, returning for a vaccination series, or producing documentation of vaccination status. Rewards are typically small (e.g., food vouchers, gift cards, lottery prizes, baby products).”
The scientific evidence supporting bribery of patients with food vouchers, gift cards and other products of limited value was said to be 4 out of 4, meaning very strong. In other words, incentives, even near-worthless ones, work.
Indeed, we saw this during COVID-19 as well. People were lining up for experimental COVID shots in return for a doughnut, hamburger and fries or even a free lap dance at the local strip club. The pattern is the same. Throw the patient a bone and they’ll agree to things that bring others big profits.
As patients, we need to get savvier about these kinds of tricks and interpret them for what they are. These kinds of “gifts” are not given out of kindness or concern for your well-being. It’s a compliance bribe, and your compliance is making someone rich. Meanwhile, any risks involved are on you.
Bribery and Vaccine Mandates
Bribery is also par for the course when it comes to vaccine mandates. As detailed in a previous article, Pfizer paid undisclosed sums to front groups that advocated for COVID jab mandates, thereby hiding their conflict of interest. In part due to the fake “grassroots” work of these groups, Pfizer was able to rake in a record-breaking $100 billion in sales in 2022.15
But the pressure from consumer groups, civil rights groups, patient groups and doctors’ groups — all of which had been paid off — was probably why COVID jab mandates could even be officially considered by the government. They created a false consensus that people desperately wanted vaccine mandates to keep everyone “safe.”
Special interest groups paid by Pfizer16 to push for COVID jab mandates and coercive vaccine policies included the Chicago Urban league (which argued that the jab mandate would benefit the Black community), the National Consumers League, the Immunization Partnership, the Advertising Council and a long list of universities and cancer, liver diseases, cardiology, rheumatology and medical science organizations.
Each of these organizations received anywhere from several thousand to hundreds of thousands of dollars from Pfizer in 2021 alone. Is it any wonder, then, that more than 50 major health care organizations called for vaccine mandates that year, including for their own workers?17
Childhood Vaccination Rates Tanked During COVID
While the COVID-19 pandemic furthered many globalist goals, it inadvertently tanked childhood vaccination rates, as many parents ended up missing routine well-child visits due to clinic closures, lockdowns and fear of taking their children outside. As reported by the American Medical Association (AMA) in November 2021:18
“… recently published research sheds new light on how the COVID-19 pandemic has disrupted some of those routine vaccinations, as parents and their children didn’t just stay home — they stayed away from the doctor.
The JAMA Pediatrics study19 … found that vaccine-administration rates were significantly lower across all pediatric age groups as the pandemic first surged in the U.S. … For example, only 74% of infants turning 7 months old in September 2020 were up to date on their vaccinations, a drop from 81% in September 2019.
And just 57% of infants who hit the 18-month mark in September 2020 were up to date, down from 61% the year before. The proportion of children up to date for routine vaccinations was lowest among Black children, with inequities more pronounced in the 18-month-old group.”
The Big Catch-Up Initiative
To get childhood vaccination rates back on track, Chelsea Clinton is now making the rounds promoting a new vaccine initiative called “The Big Catch-Up.” In a recent interview with Fortune Magazine,20 Clinton promised it would be “the largest childhood immunization effort ever.” Over the next 18 months, this initiative will attempt to “catch as many kids up as possible,” she said.
Partners in this effort include the World Health Organization, UNICEF, Gavi, the Vaccine Alliance, the Bill & Melinda Gates Foundation, Immunization Agenda 2030, and several other “global and national health partners.” As reported by the WHO, April 24, 2023:21
“The pandemic saw essential immunization levels decrease in over 100 countries, leading to rising outbreaks of measles, diphtheria, polio and yellow fever. ‘The Big Catch-up’ is an extended effort to lift vaccination levels among children to at least pre-pandemic levels and endeavors to exceed those …
While calling on people and governments in every country to play their part in helping to catch up by reaching the children who missed out, The Big Catch-up will have a particular focus on the 20 countries where three quarters of the children who missed vaccinations in 2021 live …
The 20 countries where three quarters of the children who missed vaccinations in 2021 live are: Afghanistan, Angola, Brazil, Cameroon, Chad, DPRK [Democratic People’s Republic of Korea], DRC [Democratic Republic of the Congo], Ethiopia, India, Indonesia, Nigeria, Pakistan, Philippines, Somalia, Madagascar, Mexico, Mozambique, Myanmar, Tanzania, Viet Nam.”
Vaccine Program Is Run ‘Soft Mafia’ Style
When you look at all these areas of bribery and financial incentives, doesn’t it seem as though the entire vaccine program runs on financial coercion? A sort of “soft mafia” kind of operation, where the threats and promises all revolve around money and public/professional shaming versus accolades.
What would happen if all financial incentives were removed? All the performance bonuses paid to doctors, the freebies given to patients, the “charitable donations” to industry-friendly organizations and payments to front groups?
What would happen if parents were simply given unbiased evidence and no one was financially driven to pressure them either way? I don’t have the answer. It’s a thought experiment. But I suspect that vaccination rates would drop dramatically.
Detection of five bacterial and five viral pathogens in serum and cerebrospinal fluid.
An increased frequency of Alzheimer’s disease patients positive for Treponema spp.
A significantly higher prevalence of cases with two and more simultaneous infections.
The studied pathogens were widespread equally in serum and cerebrospinal fluid.
Paralleled analysis of multiple sample specimens provides complementary information.
Abstract
Although the link between microbial infections and Alzheimer’s disease (AD) has been demonstrated in multiple studies, the involvement of pathogens in the development of AD remains unclear. Here, we investigated the frequency of the 10 most commonly cited viral (HSV-1, EBV, HHV-6, HHV-7, and CMV) and bacterial (Chlamydia pneumoniae, Helicobacter pylori, Borrelia burgdorferi, Porphyromonas gingivalis, and Treponema spp.) pathogens in serum, cerebrospinal fluid (CSF) and brain tissues of AD patients. We have used an in-house multiplex PCR kit for simultaneous detection of five bacterial and five viral pathogens in serum and CSF samples from 50 AD patients and 53 healthy controls (CTRL). We observed a significantly higher frequency rate of AD patients who tested positive for Treponema spp. compared to controls (AD: 62.2 %; CTRL: 30.3 %; p-value = 0.007). Furthermore, we confirmed a significantly higher occurrence of cases with two or more simultaneous infections in AD patients compared to controls (AD: 24 %; CTRL 7.5 %; p-value = 0.029). The studied pathogens were detected with comparable frequency in serum and CSF. In contrast, Borrelia burgdorferi, human herpesvirus 7, and human cytomegalovirus were not detected in any of the studied samples. This study provides further evidence of the association between microbial infections and AD and shows that paralleled analysis of multiple sample specimens provides complementary information and is advisable for future studies.
BREAKING: In Surprise Move, New York Says It Will End COVID Vaccine Mandate for Healthcare Workers
An attorney for the state also requested the court overturn a previous ruling striking down the mandate — a move plaintiffs’ attorneys opposed because it “leaves open the very real possibility that this constitutional violation could happen again and ruin many more lives.”
Defendants include the New York State Department of Health (NYSDOH), New York Gov. Kathleen C. Hochul and Mary T. Bassett, the state’s health commissioner.
New York’s Supreme Court Appellate Division in Rochester was set to hear arguments today — but the plaintiffs’ attorneys were cut short by the state’s announcement.
According to a joint statement released today by CHD and Gibson:
“In what can only be described as pure gamesmanship, New York State asked the court to withdraw their appeal but overturn the lower court’s decision without looking at the merits on the grounds that it was now moot.
“What that means is New York State wants the victory Sujata Gibson and Children’s Health Defense already obtained in the lower court to be thrown out because today they announced a plan to withdraw the vaccine mandate for healthcare workers.”
Gibson told CHD.TV, “The law does not allow an agency to voluntarily stop an illegal activity and then claim they shouldn’t be held legally accountable.”
(See link for article)
_________________
**Comment**
Everyone wants amnesty and offers hollow pseudo-apologies as if the tyranny of the past three years is all just a simple misunderstanding, but nobody wants to be held accountable for “vaccine” mandates that cost jobs, lives, and health.
Falling Off the “COVID Cliff” – The Collapse of Big Pharma Has Begun as 30% of Rural Hospitals in America Facing Closure
Comments by Brian Shilhavy Editor, Health Impact News
Article Excerpts:
The Big Pharma financial bubble that was created in 2020 during the Trump Administration, which pumped $trillions into Big Pharma for COVID, has burst.
It is being referred to in the corporate media as falling off of the “COVID Cliff.”
Those falling the deepest are the ones who greatly benefited from the COVID scam, as reflected in the 2023 first quarter financial reports of drug makers.
There are 646 rural hospitals at risk of closure due to financial issues, comprising around 30 percent of all rural hospitals in the U.S., according to the Center for Healthcare Quality & Payment Reform.
The hospitals face losses on patient services as health plans aren’t paying enough to cover the cost of care delivery. The losses will likely increase as inflation and workforce shortages persist, according to the report, which was released in April. While rural hospitals are receiving some support through grants, local tax revenues or other profits, they still have low financial reserves and remain at risk.
More than half the states in the U.S. report 25 percent or more of their rural hospitals are at risk of closure, and more than 200 hospitals nationwide are at immediate risk of closing. (Source.)
Normally all these financial losses in the U.S. medical system would have crashed the economy by now, but of course the U.S. Stock Market ponzi casino is pumping money into the current financial bubble: Big Tech.
No more “kicking the can down the road.” We just fell off the COVID cliff, and the rest of the economy will follow.