Deer, fragmented forests, ticks, a Lyme-like disease … and a little praise for possums
It’s a drag: In a photo from 2013, Joanna Weeks ’13 drags a cloth to collect ticks working with W&M biologists Matthias Leu (left) and Oliver Kerscher. The three were among the co-authors on a 2019 paper that examines the link between a Lyme-like tick-borne disease and fragmented forested habitat. Photo by Joseph McClain
by Joseph McClain | October 17, 2019
“…Say — what’s that?”
“Nothing but a tick.”
“Where’d you get him?”
“Out in the woods.”
“What’ll you take for him?”
“I don’t know. I don’t want to sell him.”
—Tom and Huck, in Tom Sawyer
Ticks were evidently so rare in Samuel Clemens’ Hannibal that a single live specimen had value enough to tempt Tom Sawyer to part with his newly shed tooth. Matthias Leu says it was the same in the Switzerland of his more recent youth.
“When I was a boy, I spent all my time in the forest,” Leu said. “I never saw one tick. And in Switzerland now, you should not leave the trails because there are so many ticks. So, it’s not just in North America; it’s global.”
__________________
**Comment*
Great read which exposes the fact that little is known about the Ehrlichia chaffeensis bacterium which gives similar symptoms as Lyme disease. According to biologist Matthias Leu, “There probably has been a lot of ehrlichiosis that was misdiagnosed as Lyme.” Leu and his colleagues studied the habitat of the Lone Star Tick and found that forest fragmentation causes more edges which deer love, giving ticks an easy meal.
Leu explains that deer are “competent hosts,” serving not only as a meal for the tick, but also a reservoir for ehrlichiosis, capable of infecting the next feasting tick with Ehrlichia chaffeensis. He states that fawns and yearling deer are especially important in transmission of the bacterium.
“The failure to test for Ehrlichia, even as more and more evidence suggests that the infection may be just as common as other endemic tick-borne diseases, appears to impact patient care with antibiotics prescribed less frequently when testing is not ordered.”
Failure of the Asian longhorned tick, Haemaphysalis longicornis, to serve as an experimental vector of the Lyme disease spirochete, Borrelia burgdorferi sensu stricto
The invasive, human-biting Asian longhorned tick, Haemaphysalis longicornis, was detected in New Jersey in the eastern United States in August of 2017 and by November of 2018 this tick had been recorded from 45 counties across 9 states, primarily along the Eastern Seaboard. The establishment of H. longicornis in the United States has raised the questions of how commonly it will bite humans and which native pathogens may naturally infect this tick. There also is a need for experimental vector competence studies with native pathogens to determine if H. longicornis can acquire a given pathogen while feeding, pass it transstadially, and then transmit the pathogen in the next life stage.
In this experimental study, we evaluated the vector competence of a population of H. longicornis originating from the United States (New York) for a native isolate (B31) of the Lyme disease spirochete, Borrelia burgdorferi sensu stricto (s.s.).
In agreement with a previous experimental study on the vector competence of H. longicornis for Borrelia garinii, we found that uninfected H. longicornis larvae could acquire B. burgdorferi s.s. while feeding on infected Mus musculus mice (infection prevalence >50% in freshly fed larvae) but that the infection was lost during the molt to the nymphal stage.None of 520 tested molted nymphs were found to be infected, indicating that transstadial passage of B. burgdorferi s.s. is absent or rare in H. longicornis; and based on the potential error associated with the number of nymphs testing negative in this study, we estimate that the upper 95% limit for infection prevalence was 0.73%.
An Ixodes scapularis process control showed both effective acquisition of B. burgdorferi s.s. from infected mice by uninfected larvae and transstadial passage to the nymphal stage (infection prevalence of 80–82% for both freshly fed larvae and molted nymphs). We also observed that although H. longicornis larvae could be compelled to feed on mice by placing the ticks within feeding capsules, attachment and feeding success was minimal (<0.5%) when larvae were placed freely on the fur of the mice.
We conclude that H. longicornis is unlikely to contribute more than minimally, if at all, to transmission of Lyme disease spirochetes in the United States.
_______________
**Comment**
Transmission can still happen and if you are the sorry sucker it happens to – it makes all the difference in the world. Here’s the deal – ticks are not your friends. Take each and every tick bite as seriously as a heart attack. Little is known about the Asian Longhorned tick but in Asia it’s bite KILLS 15% of those whom contract it. Don’t take this lightly.
Several other human pathogens have been detected in the ticks, but it’s not clear the Asian longhorned species are able to transmit them to humans. They include Anaplasma, Ehrlichia, Rickettsia, and Borreliaspecies. Lyme disease is caused by Borrelia burgdorferi bacteria.
She warned that the organisms are present in states where longhorned ticks have been found and that it’s possible that the tick—known to be an aggressive biter—might be able to transmit Heartland virus, given its close relationship to SFTS virus.
Pritt said it’s clear that the invasive species is here to stay for the foreseeable future, and next steps should include public awareness campaigns that incorporate the new information, easy-to-use resources for labs to identify the tick, and more research to understand the implications of the new findings.
Researchers get closer to rapid diagnostic test for Lyme disease
A study published in the Journal of Clinical Microbiology describes a new rapid assay for Lyme disease that could lead to a practical test for use by healthcare providers.
The researchers found the assay, which uses several biomarkers to detect Lyme disease infection, was more sensitive than current laboratory-based tests when diagnosing Lyme disease early after suspected infection.
The research was supported by the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health.
Lyme disease is caused by Borrelia burgdorferi, a spiral-shaped bacterium transmitted by deer ticks. Many cases of Lyme disease can be treated effectively with a short course of antibiotics.
However, Lyme disease can be difficult to diagnose because it causes a wide range of symptoms, from fever and rash to neurologic and cardiac symptoms and joint pain. Current Lyme disease tests also can miss an infection if performed too early.
The Centers for Disease Control and Prevention recommends a two-step blood test for diagnosing Lyme disease that looks for antibodies against Lyme disease. These tests require specialized laboratory equipment and can require days or weeks to return results.
Faster, more sensitive Lyme test?
The authors of the paper plan to develop a simpler, faster, more sensitive test that could be used at the point of care during a single visit to a healthcare provider.
The researchers first screened a set of known Lyme disease biomarkers for their ability to indicate infection. They then tested for the top three biomarkers on samples from people with early Lyme disease, from healthy individuals from areas where Lyme disease is endemic, and from people with Lyme arthritis.
This was compared to results obtained using the standard two-step testing procedure.
Overall, the new set of biomarkers was more sensitive than standard Lyme disease tests. These biomarkers were better at picking up signs of Lyme disease infection in early stage samples—possibly because they were able to detect antibodies that peak in the first two to six weeks after a person is infected with Lyme disease.
These results open the possibility of developing a point-of-care test for Lyme disease. The assay will require more refinement and testing before it can be approved by the Food and Drug Administration. However, the researchers say that these results show great potential.
It’s for EARLY detection – NOT for those who have struggled with symptoms for weeks to years.
It ONLY tests for Borrelia burgdorferi – ONE strain of Lyme disease. To the best of my knowledge there are still 300 strains of borrelia and counting worldwide and 100 strains of borrelia and counting in the U.S. These strains are influx as new strains are continually being discovered.
It DOES NOT test for coinfections which can cause symptoms identical to Lyme. It’s also common for patients to be infected with numerous pathogens. For instance a person might be infected with Lyme, Babesia, Bartonella, and Mycoplasma. There are nearly 20 diseases transmitted by ticks.
Lyme disease has ALWAYS been something that demands a clinical diagnosis by a trained health care provider.
While I appreciate new technology and efforts to simplify a complex illness – this illness is NOT for dummies. The best advice I can offer health care workers is to get educated! Do not be lazy. People are literally suffering untold agony, and dying from this.
Many call this a “tick-borne” illness, but please be aware that a PhD believes there are many, many modes of transmission including sexual and congenital:
More than Lyme: Tick study finds multiple agents of tick-borne diseases
COLUMBIA UNIVERSITY’S MAILMAN SCHOOL OF PUBLIC HEALTH
IMAGE: THREE PRIMARY HUMAN-BITING TICK SPECIES PRESENT ON LONG ISLAND WERE EXAMINED IN THIS STUDY. LEFT — BLACKLEGGED TICK ALSO KNOWN AS THE DEER TICK, MIDDLE — THE AMERICAN DOG TICK,… view more
CREDIT: SANTIAGO SANCHEZ-VICENTE, STONY BROOK UNIVERSITY
In a study published in mBio, a journal of the American Society for Microbiology, Jorge Benach and Rafal Tokarz, and their co-authors at Stony Brook University and Columbia University, reported on the prevalence of multiple agents capable of causing human disease that are present in three species of ticks in Long Island.
Tick-borne diseases have become a worldwide threat to public health. In the United States, cases more than doubled, from 22,000 in 2004 to more than 48,000 in 2016, according to the U.S. Centers for Disease Control. Tick-borne diseases range from subclinical to fatal infections with disproportionate incidence in children or the elderly. Moreover, some infections can also be transmitted by blood transfusions and cause severe disease in patients with underlying disorders. While public attention has focused on Lyme disease, in recent years, scientists have uncovered evidence that ticks can carry several different pathogens capable of several different tick-borne diseases, sometimes in a single tick.
In the new study, researchers collected ticks from multiple locations throughout Suffolk county in the central and eastern part of Long Island, where seven diseases caused by microbes transmitted by ticks are present. In total, they examined 1,633 individual ticks for 12 separate microbes. They found that more than half of the Ixodes (deer ticks) were infected with the Lyme disease agent, followed by infections with the agents of Babesiosis and Anaplasmosis. Importantly, nearly one-quarter of these ticks are infected with more than one agent, resulting in the possibility of simultaneous transmission from a single tick bite.
Notably, the lone star tick, a species originating from the southern U.S., has expanded its range, possibly fueled by climate change. This study documents that the invasive lone star tick is abundant in Long Island, and that it is a very aggressive tick that can transmit a bacterium that causes a disease known as Ehrlichiosis. The lone star tick has also been implicated in cases of a novel form of meat allergy, and the immature stages can cause an uncomfortable dermatitis.
“Polymicrobial infections represent an important aspect of tick-borne diseases that can complicate diagnosis and augment disease severity,” says corresponding author Jorge Benach, PhD, Distinguished Professor at the Department of Microbiology and Immunology at the Renaissance School of Medicine at Stony Brook University. “Some of the polymicrobial infections can be treated with the same antibiotics, but others require different therapies, thus enlarging the number of drugs to treat these infections.”
“In evaluating tick-borne infection, more than one organism needs to be considered,” says senior author Rafal Tokarz, PhD, assistant professor of epidemiology in the Center for Infection and Immunity at the Columbia Mailman School of Public Health, and a graduate of the Department of Microbiology and Immunology at Stony Brook University. “This study emphasizes the need to focus on all tick-borne diseases, not just Lyme.”
###
The first author is Santiago Sanchez, a post-doctoral fellow in the Department of Microbiology and Immunology at Stony Brook University. Teresa Tagliafierro from Columbia and James Coleman from Stony Brook are co-authors of the study.
This study was funded by a grant from the National Institutes of Health to Benach. Support was also provided by the Island Outreach Foundation in Blue Point, NY, to the Stony Brook Renaissance School of Medicine. Support from the Steven & Alexandra Cohen Foundation (CU18-2692) was provided to Tokarz.
Disclaimer: AAAS and EurekAlert! are not responsible for the accuracy of news releases posted to EurekAlert! by contributing institutions or for the use of any information through the EurekAlert system.
Patients with Bartonella species infection (bartonellosis) complain of a variety of nonspecific vision problems that can affect every function of the eye. Making diagnosis and treatment decisions even more difficult, these problems can be caused by a variety of other pathogens and diseases. Fortunately, many peer-reviewed case publications, especially in ophthalmology journals, are available that describe both common and uncommon eye symptoms caused by bartonellosis.
Documented links between Bartonella species infection and vision problems focus on Bartonella henselae (cat scratch disease) and Bartonella quintana (trench fever). B. henselae is associated with contact with animals and vectors, especially cats and fleas, while B. quintana is associated with body lice. Additional species implicated include B. elizabethae and B. grahamii.
Overview
The eye consists of structures that focus light on nerve receptors at the back of the eye, nerves that feed into the optic nerve which connects to the brain, and a blood supply that connects through a central artery and vein into the body’s blood circulation. Bartonellosis can affect each of these parts of the eye.
Patients with bartonellosis-related eye problems may have symptoms in other organs as well that can help clarify whether the eye symptoms are caused by bartonellosis. Ophthalmologists and other physicians look for these additional signs because all of the eye conditions that can be caused by bartonellosis can be caused by a variety of bacteria and viruses, as well as other health conditions including autoimmune disorders.
It can be difficult to narrow down the possible causes of bartonellosis. Sometimes patients can’t remember any events that would have exposed them to Bartonella species. Other times the event, such as a cat scratch, may have occurred weeks to a month or more before symptoms appear and the patient may not think there is a connection. It can take detailed questioning by physicians to identify the possibility of Bartonella species exposure.
Structural Eye Symptoms
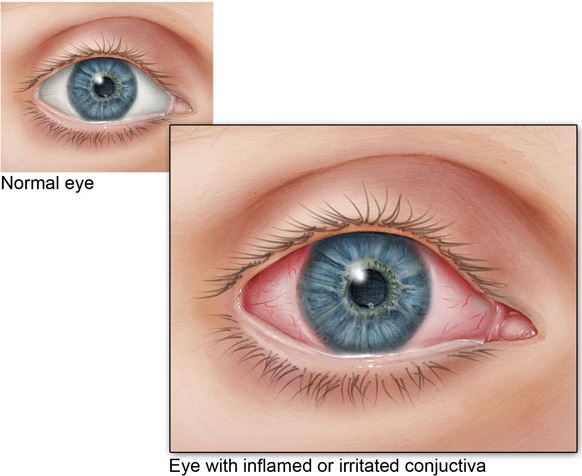
The most common way bartonellosis is seen in the eye is called Parinaud oculoglandular syndrome (POGS). About five percent of patients with acute cat scratch disease have this syndrome, which is characterized by follicular conjunctivitis (pink eye) with swollen lymph nodes nearby. It is often accompanied by a fever, and there may be bumps on the eyelid. Other symptoms known to be caused by bartonellosis, such as endocarditis (swelling of the inner lining of the heart), may also indicate that bartonellosis should be suspected.
Conjunctivitis results in easily seen inflammation of the usually white part of the eye (Source: CDC).
Inflammation of the middle layer of the structure that surrounds the eyeball is called uveitis. Uveitis causes redness of the eye and can cause light sensitivity, pain and floaters. Uveitis is sometimes associated with bartonellosis.
While case reports of eye symptoms caused by bartonellosis generally describe a sudden-onset condition, one case report describes a woman who had symptoms of bartonellosis in various body organs for more than five years, including chronic conjunctivitis (pink eye). She had multiple tests and treatments over that time including a Bartonella species test that was positive but considered nonspecific. It was only after other treatments didn’t work that antibiotics were administered. The antibiotics resolved her various symptoms.
Neurological Eye Symptoms
Neuroretinitis, an inflammation of the optic nerve head, occurs in about 2% of people with cat scratch disease (acute Bartonella henselae infection). Two-thirds of cases of neuroretinitis are caused by bartonellosis.
Neuroretinitis is usually characterized by sudden, complete vision loss and swelling that creates a star pattern in the macula (the light-sensitive tissue at the back of the eye that feeds information into the optic nerve). Though this is the typical case of neuroretinitis caused by bartonellosis, it can vary greatly. It can cause changes such as seeing odd shapes or colors Furthermore, case reports have included people who lose their vision with no other symptoms, have blurry vision with a headache, and more.
Treatment can usually, but not always, restore vision, but it can take months to resolve and there can still be long-term consequences. Complications can also occur. In one case, a child was diagnosed with neuroretinitis. Treatment was started six weeks after the diagnosis, but his vision in one eye got worse. After treatment, a full-thickness macular hole was discovered. The hole was monitored and resolved after six months.
Vascular Eye Symptoms
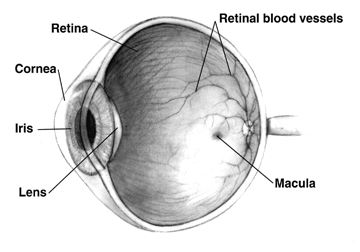
The eye has an important network of tiny blood vessels that provide nourishment to the tissue, but unnecessary growth of new capillaries can lead to a range of symptoms such as vision problems. Vasoproliferation (irregular growth of new blood vessels) may be more common in immunocompromised people, such as those being treated with chemotherapy products. These symptoms can be observed on the skin and in the liver and spleen and may also occur in the eye.
Tiny blood vessels in the eyes supply nutrients to cells. In the above image, larger retinal blood vessels can be seen (Source: NIH).
Vasoproliferative symptoms seem to be caused by vascular endothelial growth factor (VEGF) stimulated by bartonellosis. More research on the relationship between VEGF and bartonellosis is needed. Meanwhile, anti-VEGF agents have been used to treat vasoproliferative eye symptoms.
Conclusion
Bartonellosis can affect every part of the eye, and symptoms can be sudden and severe. Diagnosis and treatment decisions are complicated by other pathogens and diseases that can cause similar symptoms. It is important for patients and physicians to be aware of any prior animal or insect exposure that may indicate Bartonella infection. Considering additional systemic symptoms of bartonellosis may also help to clarify the diagnosis.
Learn more about bartonellosis and the testing that Galaxy Diagnostics offers here.
References
Kalogeropoulos, C. et al. (2011). Bartonella and intraocular inflammation: A series of cases and review of literature. Clinical Ophthalmology, 5, 817-829. doi:10.2147/OPTH.S20157 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3130920/
Woo, M. et al. (2018). A case of retinal vessel occlusion caused by Bartonella infection. Journal of Korean Medical Science, 33(47), e297. doi:10.3346/jkms.2018.33.e297 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6236082/
Fairbanks, A. M. et al. (2019). Treatment strategies for neuroretinitis: Current options and emerging therapies. Current Treatment Options in Neurology, 21(8), 36. doi:10.1007/s11940-019-0579-0 https://www.ncbi.nlm.nih.gov/pubmed/31278547
Michel, Z. et al. (2019). Multimodal imaging of two unconventional cases of Bartonella neuroretinitis [epub ahead of print]. Retinal Cases & Brief Reports. doi:10.1097/ICB.0000000000000893 https://www.ncbi.nlm.nih.gov/pubmed/31348120
Gunzenhauser, R. C. et al. (2019). The development and spontaneous resolution of a full-thickness macular hole in Bartonella henselae neuroretinitis in a 12-year-old boy. American Journal of Ophthalmology Case Reports, 15, 100515. doi:10.1016/j.ajoc.2019.100515 https://www.ncbi.nlm.nih.gov/pubmed/31341998
Toumanidou, V. et al. (2017). Neuroretinitis secondary to Bartonella henselae in a patient with myelinated retinal nerve fibers: Diagnostic dilemmas and treatment. Ocular Immunology and Inflammation, 27(3), 396-398. doi:10.1080/09273948.2017.1409357 https://www.ncbi.nlm.nih.gov/pubmed/29283743
Mabra, D. et al. (2018). Ocular manifestations of bartonellosis. Current Opinion in Ophthalmology, 29(6), 582-587. doi:10.1097/ICU.0000000000000522 https://www.ncbi.nlm.nih.gov/pubmed/30124532
Beckerman, Z. et al. (2019). Rare presentation of endocarditis and mycotic brain aneurysm [epub ahead of print]. The Annals of Thoracic Surgery. doi:10.1016/j.athoracsur.2019.06.073 https://www.ncbi.nlm.nih.gov/pubmed/31425670
_________________
**Comment**
Another great article by Galaxy Lab. Please read the following article for more information on Bartonella, as various strains are suspected to be transmitted by ticks, mites, various flies and spiders, and other modes, and it is far more prevalent than thought: https://madisonarealymesupportgroup.com/2016/01/03/bartonella-treatment/ Fifteen species of gram-negative aerobic Bartonella are known to infect humans; however Dr. Ricardo Maggi’s statement is quite telling, “This case reinforces the hypothesis that any Bartonella species can cause human infection.”