Why Doctor Treated Patient for Lyme – Even When His Test Was Negative
https://danielcameronmd.com/treated-lyme-negative-test/
Patients Deserve an Explanation
One of the most common—and most important—questions I hear from patients is:
“If my Lyme test is negative, why are you still treating me?”
It’s a fair question. And if you’re asking it, you deserve a clear and compassionate answer. The truth is, when it comes to Lyme disease, test results don’t always tell the full story.
Let’s break down why.
Lyme Disease Testing Isn’t Always Reliable
The standard test used to diagnose Lyme disease is called the two-tier system. It includes an ELISA screening test followed by a Western blot if the first result is positive. But this system is far from perfect—especially when the infection is in its early or late stages.
Here’s what you should know:
- Early in the infection, your body may not have produced enough antibodies yet to trigger a positive result
- Some patients never produce detectable antibodies at all
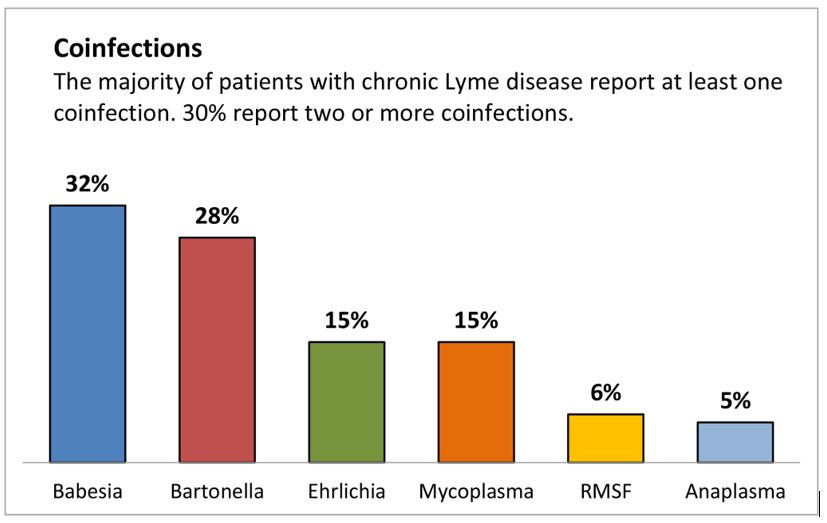
- Co-infections like Babesia or Bartonella are not picked up by this test
- Many rashes don’t appear in the textbook “bulls-eye” pattern—or don’t appear at all
So yes—you can absolutely have Lyme disease, even if your test is negative. And unfortunately, this is more common than many realize.
In Medicine, We Don’t Wait for Disease to Get Worse
In most areas of healthcare, we don’t wait for a serious event before we start treatment.
- We don’t wait for a stroke to treat high blood pressure
- We don’t wait for vision loss to manage diabetes
- We don’t wait for full organ failure to address chronic kidney disease
We act early—because we know that early treatment improves outcomes. So why does Lyme disease often get treated differently?
When it comes to Lyme, many patients are told to “wait and see”—even when the symptoms are clear and distressing.
Waiting Is Not a Neutral Decision
Here’s what I tell my patients:
Waiting is not harmless. It’s a medical decision with consequences.
Delaying treatment can allow symptoms to worsen. It can allow the infection to persist or spread. In some cases, patients who were told to wait eventually end up with a label: Post-Treatment Lyme Disease Syndrome (PTLDS)—a condition where symptoms linger long after the initial infection was treated, or in some cases, never properly treated at all.
What if we had treated earlier? Could we have prevented months—or even years—of suffering?
In many cases, the answer is yes.
Clinical Judgment Is Not Guesswork
When I decide to treat someone for Lyme disease despite a negative test, it’s not a random decision. It’s based on:
• The full pattern of your symptoms
• Your medical history
• Your response to prior treatments
• Known or likely tick exposure
• And experience with thousands of Lyme patients
This is called clinical judgment. It’s a core part of good medical practice. I don’t ignore science—I apply it in context. Because Lyme doesn’t always follow the rules, and neither should we when those rules are failing real people.
You Know When Something Feels Wrong
I’ve met patients who’ve been told their symptoms are “just stress” or “hormonal” or “all in their head.” But they know their bodies. They’ve tracked their fatigue, their joint pain, their cognitive changes. They’ve seen something shift—and they’re right to speak up about it.
Many of those patients improve once treatment begins, even if their test results never confirmed the diagnosis. That’s not luck. That’s Lyme disease showing up in real life—even when it doesn’t show up in the lab.
It’s Time to Rethink How We Treat Lyme
We’re in a new era of medicine. Patients are more informed, more proactive, and more in tune with their own health than ever before. But too often, our Lyme diagnostic standards are stuck in the past—waiting for certainty while people lose months or years of their lives to untreated illness.
We need to bring clinical judgment back into focus. We need to listen more, wait less, and treat Lyme disease with the urgency it deserves.
Final Thoughts
If you’ve been told your test is negative, but you’re still struggling with symptoms—please know this:
You’re not imagining it. You’re not overreacting. And you’re not alone.
In my practice, I treat the whole patient—not just the lab result. Because when it comes to Lyme, early treatment can change everything.
Want to learn more? Follow my blog series for more insights on Lyme disease diagnosis and care—or reach out to my office if you’re looking for answers.
You deserve to be heard.
Related Articles:
Relying on a negative Lyme disease test can prove deadly
Don’t wait for a positive Lyme disease test
Can’t trust single dose of doxycycline to prevent Lyme disease
_______________
**Comment**
A very needed article with crucial information for all to understand.
Testing for Lyme/MSIDS is abysmal. Clinical judgement is required; however, doctors receive little training for tick-borne infections and whatever training they do receive is antiquated and biased. The fact the needle hasn’t budged in 40 years is proof of this fact.
Dr. Cameron is an example of an independent doctor who could save your life. He’s also a Lyme-literate doctor who has studied under ILADS and who has years of experience treating this. Like many of his colleagues, he’s been attacked by the state medical board – which is common for these doctors because they do not partake in the globalist idea for ‘consensus-based’ medicine – which turns doctors into robots who blindly follow dictates from bureaucrats who are profiting from conflicts of interests including patents, drugs, and other metabolomics.
Due to the horrific lack of education on all things Lyme/MSIDS, there is a parallel group to the tyrannical IDSA (Infectious Diseases Society of America) called ILADS (International Lyme and Associated Diseases Society) which holds their own medical conferences to educate doctors on what is happening in reality with Lyme/MSIDS and through independent, global research that the IDSA simply ignores or maligns. Their next conference, “The Complexity of Lyme: Diagnosing and Treating Tick-Borne and Related Diseases,” is June 7-8 in Philadelphia.
Our conference will include:
- Introduction to diagnosing and treating vector-borne diseases
- Case discussions with experts
- Advanced topics in clinical treatments such as PANS/PANDAS, Mold toxicity, MCAS, supportive natural therapies and more.
- Exhibitors showcasing medical services
- CME credit available
The conference is open to healthcare professionals. Students enrolled in a medical degree program and PhD candidates conducting Lyme-related research are also eligible to attend and qualify for discounted rates. Email conference@ilads.org for more information.