Rickettsiales in Ticks Removed From Outdoor Workers From Georgia & Florida
https://wwwnc.cdc.gov/eid/article/25/5/18-0438_article
Volume 25, Number 5—May 2019
Research Letter
Rickettsiales in Ticks Removed from Outdoor Workers, Southwest Georgia and Northwest Florida, USA
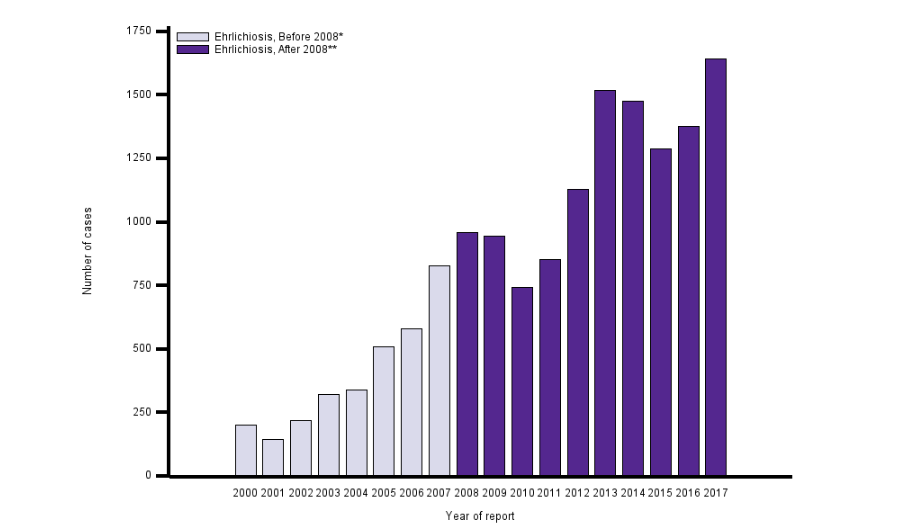
The southeastern United States has multiple tick species that can transmit pathogens to humans. The most common tick species, Amblyomma americanum, is the vector for the causative agents of human ehrlichioses and southern tick-associated rash illness, among others (1). Dermacentor variabilis ticks can transmit the causative agent of Rocky Mountain spotted fever, and Ixodes scapularis ticks can transmit the causative agents of Lyme disease, babesiosis, and human granulocytic anaplasmosis (1). Although less common in the region, A. maculatum ticks are dominant in specific habitats and can transmit the causative agent of Rickettsia parkeri rickettsiosis (1).
Persons who have occupations that require them to be outside on a regular basis might have a greater risk for acquiring a tickborne disease (2). Although numerous studies have been conducted regarding risks for tickborne diseases among forestry workers in Europe, few studies have been performed in the United States (2,3). The studies that have been conducted in the United States have focused on forestry workers in the northeastern region (2). However, because of variable phenology and densities of ticks, it is useful to evaluate tick activity and pathogen prevalence in various regions and ecosystems.
Burn-tolerant and burn-dependent ecosystems, such as pine (Pinus spp.) and mixed pine forests commonly found in the southeastern United States, have unique tick dynamics compared with those of other habitats (4). The objective of this study was to determine the tick bite risk and tickborne pathogen prevalence in ticks removed from forestry workers working in pine and mixed pine forests in southwest Georgia and northwest Florida, USA.
During June 2009–December 2011, forestry workers in southwestern Georgia (7 counties) and northwestern Florida (1 county) submitted ticks crawling on or attached to them. We identified ticks and tested them for selected pathogens (Appendix). Immature forms of the same species from the same day and person were pooled (<5 nymphs and <20 larvae) for testing.
A total of 53 persons submitted 362 ticks (Table). Excluding larvae, the most common tick species submitted was A. maculatum, followed by A. americanum, I. scapularis, and D. variabilis. On 4 occasions, 1 person submitted A. tuberculatum ticks (3 batches of larvae and 1 batch of nymphs) from a longleaf pine site in Baker County, Georgia. Average submissions per persons were 2.6 ticks (median 1 tick), but 1 person submitted 100 ticks. A total of 24 persons submitted ticks more than once, and they submitted an average of 0.08–6.5 ticks/month (overall average submission rate of 1.1 ticks/month). Three ticks were engorged (1 D. variabilis adult, 1 A. americanum nymph, and 1 Amblyomma sp. nymph); only the Amblyomma sp. nymph was positive for a pathogen (R. amblyommatis).
- Rickettsia spp. prevalence was 36.4% in adult, 27.9% in nymphal, and 20% in larval A. americanum ticks; R. amblyommatis was the only species identified (Table).
- Rickettsia spp. were detected in 23% of A. maculatum adults; R. amblyommatis was most common (6.0%), followed by R. parkeri (4.8%).
- A previously detected novel Rickettsia sp. was identified in 10 of 11 A. tuberculatum larval pools and was reported by Zemtsova et al. (6). An additional pool of A. tuberculatum nymphs was tested in this study and also was positive for the novel Rickettsia sp.
- E. chaffeensis was detected in 1 A. maculatum adult (prevalence 1.2%), and Panola mountain Ehrlichia sp. was detected in 2 A. maculatum adults (prevalence 2.4%) and 1 D. variabilis adult (prevalence 10%).
- No ticks were positive for Borrelia spp., E. ewingii, or Anaplasma phagocytophilum.
Thus, forestry workers were found to encounter ticks on a regular basis, and peak encounter rates reflected previously reported tick seasonality in this region (4). Only 3 (0.8%) of the ticks submitted were engorged, indicating prompt removal of most ticks and thus low risk for pathogen transmission. A. maculatum, a fairly uncommon tick in the southeastern United States, was the most commonly submitted tick. However, A. maculatum ticks dominate in regularly burned pine ecosystems (4), which is where most of these workers spent their time.
We observed several unique findings related to pathogens during this study. Larvae and nymphs of A. tuberculatum ticks were submitted on multiple occasions, a tick rarely reported on humans (7). These findings in conjunction with the identification of a novel Rickettsia sp. (6), suggest that additional research is warranted. This study also identified E. chaffeensis and Panola Mountain Ehrlichia in A. maculatum ticks. Although A. americanum ticks are considered the primary vector of Ehrlichia spp., these pathogens have been occasionally reported in questing A. maculatum ticks, suggesting that this tick might be involved in their transmission cycles (5,8). We also detected Panola Mountain Ehrlichia in 1 D. variabilis tick. Thus, further research regarding these alternative tick species as potential vectors of these pathogens is warranted, particularly in the case of A. maculatum ticks, which were a common species on forestry workers and are widespread in this region (4).
At the time of this study, Dr. Gleim was a research scientist at the University of Georgia, Athens, GA. She is currently a disease ecologist at Hollins University, Roanoke, VA. Her research interests include wildlife and zoonotic diseases with a particular emphasis on tickborne diseases.
Acknowledgments
We thank the persons whom submitted ticks for this study and members of the Yabsley and Levin laboratories for providing laboratory assistance.
This study was supported by the Centers for Disease Control and Prevention/University of Georgia (UGA) collaborative grant (#8212, Ecosystem Health and Human Health: Understanding the Ecological Effects of Prescribed Fire Regimes on the Distribution and Population Dynamics of Tick-Borne Zoonoses); the Oxford Research Scholars Program at Oxford College of Emory University; the Joseph W. Jones Ecological Research Center, the Warnell School of Forestry and Natural Resources (UGA); the Southeastern Cooperative Wildlife Disease Study (UGA) through the Federal Aid to Wildlife Restoration Act (50 Statute 917); and Southeastern Cooperative Wildlife Disease Study sponsorship from fish and wildlife agencies of member states.
References
-
Allerdice ME, Hecht JA, Karpathy SE, Paddock CD. Evaluation of Gulf Coast ticks (Acari: Ixodidae) for Ehrlichia and Anaplasma species. J Med Entomol. 2017;54:481–4.https://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&list_uids=28031351&dopt=Abstract
Table
**Comment**
Again, folks down South should be taken seriously when they present with symptoms. BTW: Southern advocates tell me that STARI looks, smells, and feels just like Lyme disease.
Lyme IS in the South: https://madisonarealymesupportgroup.com/2016/10/25/hope-for-southerners/
The take home: Clark is finding borrelia (Lyme) strains in the South that the current CDC two-tier testing will never pick up in a thousand years.
The take home: Clark found live Bbsl (bissettii-like strain) in people from the Southeast who had undefined disorders not typical of LD, and were treated for LD even though they were seronegative, proving that B. bissetti is responsible for worldwide human infection.
He also showed DNA of Bbsl in Lone Star ticks which might be a bridge vector of transmission to humans.
Dr. Clark was the first to report finding LD spirochetes in animals and ticks in South Carolina, as well as in wild lizards in South Carolina and Florida. He has documented the presence of LD Borrelia species, Babesia microti, Anaplasma phagocytophilum, Rickettsia species, and other tick-borne pathogens in wild animals, ticks, dogs, and humans in Florida and other southern states.
Clark is infected. Surprised? This is why he’s finding answers – it’s much more than a job to him.
https://madisonarealymesupportgroup.com/2018/05/31/no-lyme-in-the-south-guess-again/
Time to start believing people!