Diagnosis of systemic cat scratch disease may be challenging. Here, we describe a case of an immunocompetent girl exhibiting fever and multifocal hepatosplenic abscesses.Diagnostic tests for Bartonella henselae infection (enzyme immunoassay and polymerase chain reaction) were found steadily negative and the diagnosis, suspected on the basis of the Margilet’s criteria, was finally confirmed by indirect immunofluorescent antibodies.
______________________
**Comment**
“Troublesome” is certainly an understatement!
According to this, hepatosplenic abscesses in CSD are rarely reported in immunocompetent children, and only 36 cases are listed in various databases: https://pubmed.ncbi.nlm.nih.gov/31307480/
Typically abdominal pain is noted (but not always) and abdominal ultrasounds show the abscesses.
The good news is according to this, antibiotic treatment improves patients quickly:
Herxheimer Reaction Cause Debunked as New Research Reveals True Cause
By Dr. David A. Jernigan
Remarkable new research debunks the dominant explanation for why people undergoing antibiotic treatment for Lyme disease very often experience a dramatic worsening of their symptoms, as well as new symptoms, in what is known as a Jarisch-Herxheimer reaction. The dominant explanation has been essentially that the guts or endotoxins of the dying bacteria spill into the body causing this worsening of symptoms. This explanation, though widely held as true is, according to the scientific research, completely incorrect.
This article will present research explaining why natural and prescription antibiotics cause severe herx reactions when compared to the use of induced native bacteriophages, which can completely annihilate the entire population of the targeted bacteria, with virtually no Herx reaction. The article will also present preventive measures to minimize herx reactions if inefficient treatments, such as natural and prescription antibiotics, are utilized.
What Actually Causes a Herx Reaction?
In order to develop effective therapeutic countermeasures to herx reactions, the pathophysiology, or the disordered physiological processes associated with a herx reaction, must be understood.
Many authors have incorrectly proposed that the Herxheimer reaction is caused by the release of toxins (endotoxins) by dying spirochetes, or Mast Cell Activation (MCAS) cytokine-responses causing inflammation in response to spirochete endotoxins. However, according to the most recent understanding, these mechanisms are largely unsupported by the research.
“After antibiotic treatment, spirochetes are rendered more susceptible to PMN phagocytosis likely caused by an alteration of the microbial surface to expose antigens and molecular patterns that allow antibody and complement to bind more effectively for phagocytic uptake. Once inside, PMN spirochetes probably provoke more severe inflammation.“
Butler goes on to say:
“Causes of inflammation in the JHR (Herx Reactions) are multi-factorial. When spirochetes are cleared from blood by phagocytosis, rises in concentrations of pro-inflammatory cytokines occur. Spirochetal inflammatory substances include lipoproteins and nonendotoxin pyrogens that cause rises in cytokines such as TNF-a, IL-6, and IL-8, as well as rises in histamine.”
The True Cause of a Herx Reaction in Layman’s Terms
In layman’s terms, a Herx is not just any worsening from any cause while undergoing treatment with antibacterial medication. A Herx occurs with antibiotics and other antibacterial efforts, such as botanicals, due to the fact that while the antibiotics do kill some of the bacteria, they often only injure many of the bacteria and/or cause a slow death, which allows your body’s immune cells, called phagocytes, time to come along and gobble up (PNM phagocytosis) these injured and dying bacteria, much like a Pac-Man from the old video game.
Once gobbled up, these live bacteria release genetic material inside of the phagocyte, causing it (the Pac-Man) to crank out excessive amounts and various types of cytokines, which are biochemicals that promote inflammation. This does not occur when bacteriophages kill the bacteria, since the phages literally kill the bacteria outright and so rapidly, that when the Pac-men of the immune system come along, they only gobble up the dead pieces, and no cytokines are produced, therefore there is no increased inflammation.
A Herx reaction:
Is not a desirable event.
Serves no therapeutic benefit.
Is a sign that the antibacterial medication is increasing inflammation and damage in the body.
Is a sign of inefficient medication is being utilized, causing live and damaged bacteria to be engulfed by phagocyte immune cells.
Should be avoided
Lessons from Bacteriophages: Less Herx From Bacteriophages Than Antibiotics:
Much of what we now understand about a Herx reaction is through the science of bacteriophages, which are viruses that only infect bacteria. When induced, or stimulated, bacteriophages can completely and rapidly kill all of the bacteria they infect, annihilating the entire target bacteria population. When the last of the bacterial population is dead, the bacteriophages themselves die within four days.
Anti-Herx Therapeutic Measures: (If antibiotics and botanicals are being used to kill bacteria )
Botanical/Nutitional/Homeopathic/Fatty Acid: Doctor recommended anti-inflammatory and anti-cytokine support
I.V. Hydration has been shown to reduce the occurrence and severity of herx reactions
Hyperbaric Oxygen therapy (HBOT), and other oxygen therapies have been shown to reduce the severity of herx reactions
BEMER mat therapy
Near/Mid/Far Infrared Sauna therapy
Antihistamines and enhance the optimum histamine clearance via enzyme activation in the metabolic pathway.
NSAID’s can have a beneficial effect on acute herx reactions
Note: Toxin-binder supplements used to bind up and eliminate bacterial endotoxins are understood now to not be of therapeutic benefit in that there are no bacterial endotoxins to bind. These binder products can often be beneficial for other environmental toxins.
Conclusion:
Antibiotics have dominated the medical treatment of infections for almost a century, are an inefficient approach to dealing with infections, especially in light of the more rapid and precise actions of therapeutic bacteriophage treatments.
Many people who believe they are feeling worse due to the medication working, are actually being injured by the clumsy manner in which antibiotics work, not to mention their direct pharmaco-toxic effects. Many people report having to ramp up to a therapeutic dose of the more popular antibiotics, such as Disulfiram, often experiencing horrible symptoms, leaving the patient to wonder if they should tough it out and continue the drug, risking being permanently injured by the process, or to discontinue altogether.
Patients are often left on their own, searching the social media groups for guidance and encouragement, since their physician offered no advice on dealing with the very predictable problems they will face.
In the article by Thomas Butler states, “Physicians need to anticipate a JHR when treating spirochetal diseases to provide supportive care of monitoring vital signs and administering fluids.” The prognosis according to the research linking in this article, is favorable for full recovery even if a herx reaction occurs, usually resolving in a few hours in most patients given supportive care and adequate weekly IV nutritional fluids, such as a Myers Cocktail, or High-dose Vitamin C with Glutathione.
Although for many years it was thought that a Herxheimer reaction was caused by the toxins released as bacteria die and break apart, we now know this is incorrect. A Herxheimer reaction the result of the ingesting of the live, antibiotic-weakened bacteria, by immune cells, specifically polymorphonuclear leukocytes, white blood cells, such as neutrophils, which eat the live bacteria and eventually digest them, but in the meantime the bacteria, through genetic transcription cause the production of highly proinflammatory cytokines, TNF-a, IL-6, IL-8, and histamine.
When the target bacteria die from phages causing their death by lysis, as is the case with INPT bacteriophage therapy, the bacteria burst and the polymorphonuclear cells gobble up the dead pieces. In that there are no live bacteria essentially being eaten by these immune cells, very little cytokines are produced.
Bacteriophages kill the targeted bacteria extremely quickly, killing all of the target bacterial population usually in less than seven days, which means that by the time the immune system can begin to respond, the war is over. This means that when neutrophils arrive at the scene to start the cleanup, there is only remnants of the dead bacterial, and no live bacteria are being engulf, therefore the bacteria cannot cause genetic transcription and thus cannot cause the production of excessive proinflammatory cytokine substances…thereby there is minimal if any Herx reaction. All of this translates into phages cause much less herx symptoms than do antibiotics.
Conversely, many of the worsening symptoms experienced with natural or prescription antibiotics, including the latest trending antibiotic, Disulfiram, are due to the disruptive nature of the medication on the patient’s metabolic processes and frank antibiotic toxicity. These antibiotic-induced Herxheimer reactions are often the cause of poor patient compliance, often causing the patient to self-reduce the therapeutic dosage, enabling improved tolerance but greater risk of bacterial mutations rendering the drug ineffective. Antibiotic treatment can also result in new symptoms that can last months or be permanent.
Bacteriophage therapies are a superior form of treatment in the fight of treatment-resistant microbial infections.
Ongoing Development of INPT at the Biologix Center
INPT was developed by Phagen Corp. and is being used at the Biologix Center for Optimum Health, as a part of an IRB study, to go beyond Borrelia and target any microbial issue, including all of the co-infections associated with Lyme disease, as well as Candida sp., mold, and parasite infections, however at this time the only lab test for detecting bacteria-specific phages is for Borrelia strains.
The future of INPT includes intravenous and injectable forms of application, in addition to the present oral medication, available through doctors only. INPT is not projected to be sold directly to the public at this time.
I know practitioners are all quite biased in their approach to Lyme/MSIDS based upon their own experiences and preferences. Some promote herbal therapy, some ozone therapy, some have used antibiotics for decades, some hyperthermia with antibiotics, and so on. Here we read of a practitioner using phage therapy, so his experiences are going to be viewed through that lens.
To my knowledge there is still no magic bullet treatment for Lyme/MSIDS. The jury’s out for me on phage therapy until I learn more and hear of actual patient success with it, but in my experience, the axiom “If it’s too good to be true, it usually is,” has proven true again and again. I think we would all give our left arms to eradicate Lyme/MSIDS quickly , inexpensively, and without pain, but alas, I’ve yet to discover this secret elixir. I remember the promised Stem Cell Therapy which turned out to be a big, fat dud for tick-borne illness. This stem-cell documentary was eye-opening to say the least: https://madisonarealymesupportgroup.com/2020/07/27/free-documentary-from-jail-cell-to-stem-cell-the-next-con-for-the-ex-con-documentary/ (You can probably still find it on another platform for free)
The information on the cause of herxheimer reactions is also interesting – but the result is somewhat the same: inflammation and pain. Patients really don’t care why. This inflammation and pain can make many patients question their treatment and even quit – or mistakenly believe if they just change doctors all will be well. I’ve experienced this myself too many times to count, but slow and steady – utilizing a multi-pronged approach (treat, detox, support) with numerous antimicrobials (antibiotic, ozone, herbs, EO’s, and more) won the race for my husband and I. We relapsed twice, requiring 2-3 month stints which brought us to our current remission. I’m also hearing good reports of Disulfiram. Go here for Lyme treatments: https://madisonarealymesupportgroup.com/2016/02/13/lyme-disease-treatment/ (Numerous sources for treatment outcomes within link as well)
I think there are still many ways to skin a cat, and I truly hope phage therapy actually works as we definitely need more tools in our toolbox for this beast that ‘authorities’ continue to under appreciate.
Marna Ericson, PhD, Assistant Professor, University of Minnesota
Monica Embers, PhD, Associate Professor, Tulane University
Edward Breitschwerdt, DVM
Melanie S. Steele Professor of Medicine and Infectious Diseases, North Carolina State University College of Veterinary Medicine
Robert Mozayeni, MD, Translational Medicine Group
Neil Spector, MD (posthumously), Associate Professor Medicine, Duke University Medical Center
Why is Bartonella important to consider as a differential diagnosis? What should patients and the public know about prevention, diagnosis and treatment? What does the latest science tell us about Bartonella? How does it interact with Lyme and other tick-borne diseases? What should patients/public know about prevention, diagnosis and treatment?
Hosted by “Icahn School of Medicine at Mount Sinai proudly supported by the Steven & Alexandra Cohen Foundation: Cohen Lyme & Tickborne Disease Initiative”
Effect of Dapsone alone and in combination with intracellular antibiotics against the resistant morphological forms of Borrelia burgdorferi, Richard Horowitz, MD
Also see:https://www.mdpi.com/2079-6382/9/11/725 Case study of 3 patients with relapsing and remitting Lyme disease as well as a retrospective chart review of 37 additional patients undergoing DDD CT therapy (40 patients in total) was also performed, which demonstrated tick-borne symptom improvements in 98% of patients, with 45% remaining in remission for 1 year or longer.
Melatonin has been shown to play a role in viral infections and research suggests it may be an important adjunct to COVID-19 treatment
Data analysis by Cleveland Clinic found patients who used supplemental melatonin had a 28% lower risk of testing positive for COVID-19. Blacks who used melatonin were 52% less likely to test positive for the virus
Melatonin attenuates several pathological features of COVID-19, including excessive inflammation and oxidation, exaggerated immune response resulting in a cytokine storm, acute lung injury and acute respiratory distress syndrome
A case series reports patients given 36 mg to 72 mg of intravenous melatonin per day as an adjunct therapy to standard of care improved within four to five days; all survived
Texas urgent care clinics using high-dose melatonin in combination with vitamin C and vitamin D say they’ve successfully treated hundreds of COVID-19 patients.Melatonin enhances vitamin D signaling and the two work synergistically to enhance your mitochondrial function
Melatonin is a hormone synthesized in your pineal gland and many other organs.1 While it is most well-known as a natural sleep regulator, it also has many other important functions.2 For example, melatonin:
Is a potent antioxidant3 with the rare ability to enter your mitochondria,4 where it helps “prevent mitochondrial impairment, energy failure and apoptosis of mitochondria damaged by oxidation.”5 It also helps recharge glutathione,6 and glutathione deficiency has been linked to COVID-19 severity
May prevent or improve autoimmune diseases, including Type 1 diabetes10
Is an important energy hormone that can influence your energy level11
Helps regulate gene expression via a series of enzymes12
Has anticonvulsant and antiexcitotoxic properties13
Melatonin Also Has Important Role in COVID-19 Treatment
Melatonin has also been shown to play a role in viral infections14 and according to a June 2020 research paper15,16,17 in Life Sciences journal, it may be an important adjunct to COVID-19 treatment. According to the authors, melatonin attenuates several pathological features of COVID-19, including:18
Excessive oxidative stress and inflammation
Exaggerated immune response resulting in a cytokine storm
Acute lung injury
Acute respiratory distress syndrome
They point out that melatonin is also “effective in critical care patients by reducing vessel permeability, anxiety, sedation use, and improving sleeping quality, which might also be beneficial for better clinical outcomes.”19
The scientific review paper,20 “Melatonin Potentials Against Viral Infections Including COVID-19: Current Evidence and New Findings,” published October 2020 in Virus Research journal, also summarizes the many potential mechanisms by which melatonin can protect against and ameliorate viral infections.
The authors review research looking at melatonin’s beneficial effects against a variety of viruses, including respiratory syncytial virus, Venezuelan equine encephalitis virus, viral hepatitis, viral myocarditis, Ebola, West Nile virus and dengue virus. Based on these collective findings, they believe melatonin may offer similar protection against SARS-CoV-2.
Melatonin Reduces Risk of Positive COVID-19 Test
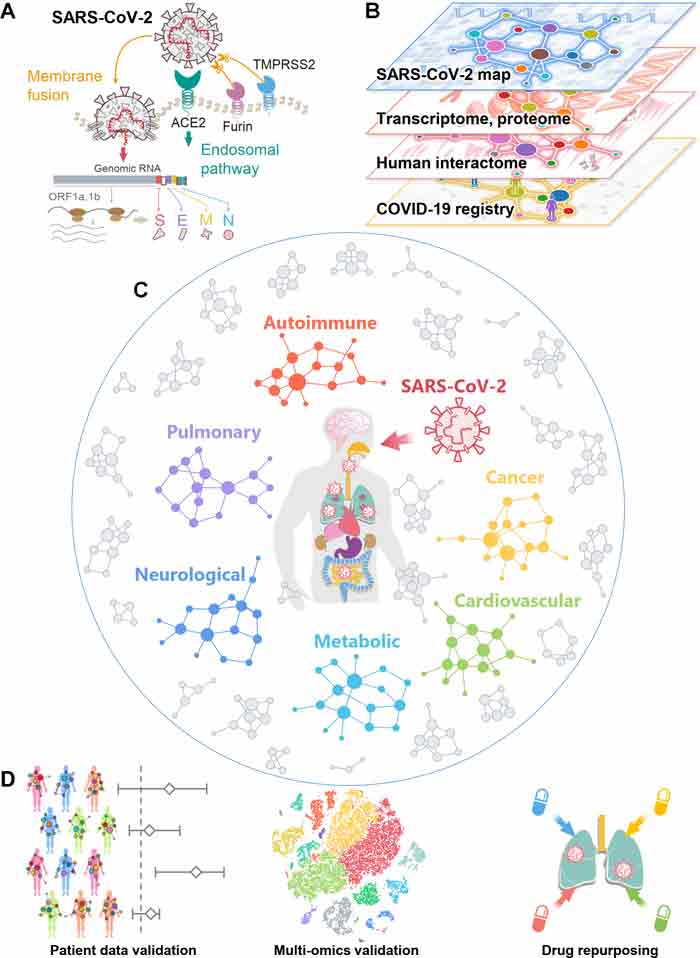
Data21,22 from Cleveland Clinic also supports the use of melatonin. Here, the researchers analyzed patient data from the Cleveland Clinic’s COVID-19 registry using an artificial intelligence platform designed to identify drugs that may be repurposed.23,24
By identifying clinical manifestations and pathologies shared by COVID-19 and 64 other diseases, they were able to conclude that certain proteins associated with chronic diseases are highly connected with SARS-CoV-2 proteins. Put another way, a number of proteins appear to play a key role in the pathologies seen both in COVID-19 and other chronic diseases. For example:25
“Analyses of single-cell RNA sequencing data show that co-expression of ACE2 and TMPRSS2 is elevated in absorptive enterocytes from the inflamed ileal tissues of Crohn disease patients compared to uninflamed tissues, revealing shared pathobiology between COVID-19 and inflammatory bowel disease.
Integrative analyses of metabolomics and transcriptomics (bulk and single-cell) data from asthma patients indicate that COVID-19 shares an intermediate inflammatory molecular profile with asthma (including IRAK3 and ADRB2).”
The diagram below illustrates (among other things) the basic pathogenesis of SARS-CoV-2 (figure A) and the network of disease manifestations associated with the infection (figure C).
These connections suggest that drugs already in use for a chronic disease may be repurposed and used in the treatment of COVID-19, as it acts on one or more shared biological targets. Melatonin stood out in this regard. Patients who used melatonin as a supplement had, on average, a 28% lower risk of testing positive for SARS-CoV-2. Blacks who used melatonin were 52% less likely to test positive for the virus.
Confounding variables adjusted for in the calculations included age, sex, race, smoking history and several known comorbidities. The authors point out that while the findings look promising, large observational studies and randomized controlled trials are still needed to validate the clinical benefits of melatonin.
Two key data points missing from the analysis are the dosage used and the length of supplementation. These data were not included in the patient registry, so we don’t know how much melatonin is required to lower your risk of SARS-CoV-2 infection to the degree found in this study.
High-Dose Melatonin Successfully Treats COVID-19
It’s possible that higher doses than those used for sleep may be needed, at least when treating an active infection. A recent case series26published in the journal Melatonin Research details how high-dose intravenous melatonin can benefit patients with COVID-19 pneumonia.
Here, patients were given 36 mg to 72 mg per day in four divided doses as an adjunct therapy to standard of care. Most supplements contain between 0.5 mg and 5 mg, and when used for sleep, you’d typically start with the lowest dose and work your way up as needed.
All of the patients given melatonin improved within four to five days, and all survived. On average, those given melatonin were discharged from the hospital after 7.3 days, compared to 13 days for those who did not get melatonin.
This is far better than the expensive treatment Remdesivir, which costs over $3,000 and doesn’t produce anywhere near this improvement.
Other Doctors Are Also Using Melatonin Against COVID-19
Dr. Richard Neel and colleagues at Little Alsace and Uvalde Urgent Care clinics in Texas also report using high-dose melatonin in combination with vitamin C and vitamin D, and had as of the last week of July 2020 successfully treated more than 400 patients.27
As reviewed in a section below, melatonin enhances vitamin D signaling and the two work synergistically to enhance your mitochondrial function. Melatonin and vitamin C are both also involved with ACE2, the receptor that SARS-CoV-2 uses to gain entry into the cell.
Together, melatonin and vitamin C help reduce SARS-CoV-2 virulence by inhibiting NLRP3 inflammasomes, which in turn inhibits cytokine storms. The Front Line COVID-19 Critical Care Working Group (FLCCC)28 also lists melatonin as an optional addition to their MATH+ protocolfor COVID-19.
How Melatonin Combats COVID-19
Research suggests melatonin may have the ability to combat COVID-19 via several different mechanisms. For example, it’s been shown to regulate immune responses and prevent cytokine storms.29 As explained by the authors of one such study,30 when your immune cells are in a hyper-inflammatory state, their metabolism changes in a way similar to that of cancer cells:
“Similar to cancer cells … immune cells such as macrophages/monocytes under inflammatory conditions abandon mitochondrial oxidative phosphorylation for ATP production in favor of cytosolic aerobic glycolysis (also known as the Warburg effect) …
The change to aerobic glycolysis allows immune cells to become highly phagocytic, accelerate ATP production, intensify their oxidative burst and to provide the abundant metabolic precursors required for enhanced cellular proliferation and increased synthesis and release of cytokines …
Because of melatonin’s potent antioxidant and anti-inflammatory activities, it would normally reduce the highly proinflammatory cytokine storm and neutralize the generated free radicals thereby preserving cellular integrity and preventing lung damage.”
Cytokine storm is one of the reasons why sepsis (blood poisoning) is so lethal, and studies have confirmed melatonin has a favorable influence on sepsis. (Sepsis is also a feature of severe COVID-19.) As reported in a 2010 study in the Journal of Critical Care:31
“Melatonin is an effective anti-inflammatory agent … Its anti-inflammatory action has been attributed to inhibition of nitric oxide synthase with consequent reduction of peroxynitrite formation, to the stimulation of various antioxidant enzymes thus contributing to enhance the antioxidant defense, and to protective effects on mitochondrial function and in preventing apoptosis.
In a number of animal models of septic shock, as well as in patients with septic disease, melatonin reportedly exerts beneficial effects to arrest cellular damage and multiorgan failure …
Apart from action on the local sites of inflammation, melatonin also exerts its beneficial actions through a multifactorial pathway including its effects as immunomodulatory, antioxidant and antiapoptotic agent.”
More recently, a 2019 animal study32 in the journal Frontiers in Immunology discusses how melatonin can protect against polymicrobial sepsis — i.e., sepsis caused by more than one microbial organism — which has a twofold higher lethality than unimicrobial sepsis (sepsis caused by a single microbe).33
In this case, melatonin appears to offer protection by having an antibacterial effect on white blood cells called neutrophils. A high neutrophil count is an indicator for infection. Melatonin may also combat SARS-CoV-2 infection by:34
Suppressing oxidative stress35
Regulating blood pressure (a risk factor for severe COVID-19)
Improving metabolic defects associated with diabetes and insulin resistance (risk factors for severe COVID-19) via inhibition of the renin-angiotensin system (RAS)
Protecting mesenchymal stem cells (MSCs, which have been shown to ameliorate severe SARS-CoV-2 infection) against injuries and improving their biological activities
Promoting both cell-mediated and humoral immunity
Promoting synthesis of progenitor cells for macrophages and granulocytes, natural killer (NK) cells and T-helper cells, specifically CD4+ cells
Inhibiting NLRP3 inflammasomes36
General Guidance for Supplementation
As mentioned, it’s very difficult to make dosage recommendations based on the limited evidence currently at hand, but since Cleveland Clinic looked at the supplements patients reported using, it seems reasonable to assume they were using it as you typically would. Most melatonin supplements contain between 0.5 mg and 5 mg.
In the case report mentioned earlier, patients were given 36 mg to 72 mg of melatonin intravenously per day, which would likely be excessive for prophylactic use. That said, research37 has found no adverse effects for dosages ranging from 20 mg up to 100 mg.
Whatever dose you take, and I recommend starting low, at 1 mg or less, be sure to take melatonin at night, before bed. Rising melatonin levels is the reason you feel sleepy in the evening, so it’s ill advised to take it in the morning or during the day, when your natural level is (and should be) low. If you happen to wake up in the middle of the night, especially if you’re exposed to a light source, you could also take some then, to help you go back to sleep.
Melatonin is also best taken sublingually, either in the form of a spray or sublingual tablet. Sublingually, it can enter your blood stream directly and doesn’t have to go through the digestive tract. As a result, its effect will be felt more rapidly.
Melatonin and Vitamin D Are a Winning Combo
Another supplement of crucial importance in the age of COVID-19 is vitamin D. Interestingly, melatonin enhances vitamin D signaling, and optimizing your vitamin D may be one of the most beneficial steps you can take to lower all of the risks associated with COVID-19, from reducing your risk of testing positive to lowering your risk of severe infection and death.
To learn more about this, download my free vitamin D report from StopCovidCold.com. Together, melatonin and vitamin D synergistically act to optimize your mitochondrial function. In fact, your mitochondria are the final common target for both.38
A deficiency in either vitamin D or melatonin has been associated with the pathogenesis of several chronic diseases, including high blood pressure, cardiovascular disease, metabolic syndrome and diabetes, just to name a few.39
These conditions have also emerged as comorbidities that significantly raise your risk of death from COVID-19. Synthesis of both vitamin D and melatonin is also dramatically reduced with advancing age, and old age is a primary risk factor for COVID-19 death. So, while vitamin D3 and melatonin supplementation may be beneficial for most people, it’s particularly important for the elderly.
Support Your Body’s Production of Melatonin and Vitamin D
Keep in mind, however, that it makes little sense to take a supplement unless you’re also seeking to optimize your body’s natural production. In the case of melatonin, this includes making sure you get good sleep on a regular basis.
You also need a good dose of natural sunlight around midday to synchronize your circadian clock so that your body produces melatonin at the appropriate time (i.e., in late evening). As the evening wears on and the sun sets, you’ll want to avoid bright and all blue lighting, as blue light inhibits melatonin synthesis. Blue lighting is predominant in LED and fluorescent bulbs that are “cool white.”
Sun exposure, of course, is also the ideal way to optimize your vitamin D. I recommend getting sensible sun exposure on large portions of your body on a regular basis, ideally daily. For further guidance, see “The Risks and Benefits of Sun Exposure.”
If for whatever reason you cannot get sufficient amounts of sun exposure, consider taking a vitamin D3 supplement (along with a little extra vitamin K2 to maintain a healthy ratio between these two nutrients).
I personally have not taken any oral vitamin D for well over 10 years and my levels are typically over 60 ng/mL, even in the winter. I have, however, started taking sublingual melatonin a few years ago as I am now in my mid-60s, even though I sleep in pitch dark and get bright sun exposure during the day.
Despite these COVID-19 treatments, our government has done all in its power to malign them. Their only answer is an experimental, fast-tracked vaccine that has caused serious adverse reactions.