My Journey
When facing illness, the last thing on your mind is the price of delivery for an at-home Covid test or order of chicken noodle soup from a local restaurant. Or is it?
As medication, food, and personal wellness prices rise amongst a price gauged economy, the cost of being sick grows increasingly staggering. As a Chronic Lyme and POTS patient for eight years, financing sickness has become woven into the fabric of my short-term and long-term budgets.
I first became sick at 16 years old; the financial burden of my care fell on my parents. My public-school teacher Mom would take sick days to take me to countless doctor’s appointments, take credit cards out to pay for MRIs, and skimp on annual family vacations in lieu of schlepping me to specialists across the country.
Neither my doctors nor my family expected me to need treatment at age 24. The financial burden has now shifted to me, aptly parallel to my transition to adulthood.
When I suffer from cyclical declines in my health: bouts of fevers, chills, flu-like symptoms, neuropathy, migraines and cognitive fogging, I notice a sharp uptick in my daily and weekly expenses. But how much could some broth and Kleenex be, anyway?
Most recently, I suffered from an eight-day long bout of illness related to my chronic Lyme. Below is a breakdown of my expenses across the eight-day span only related to being sick.
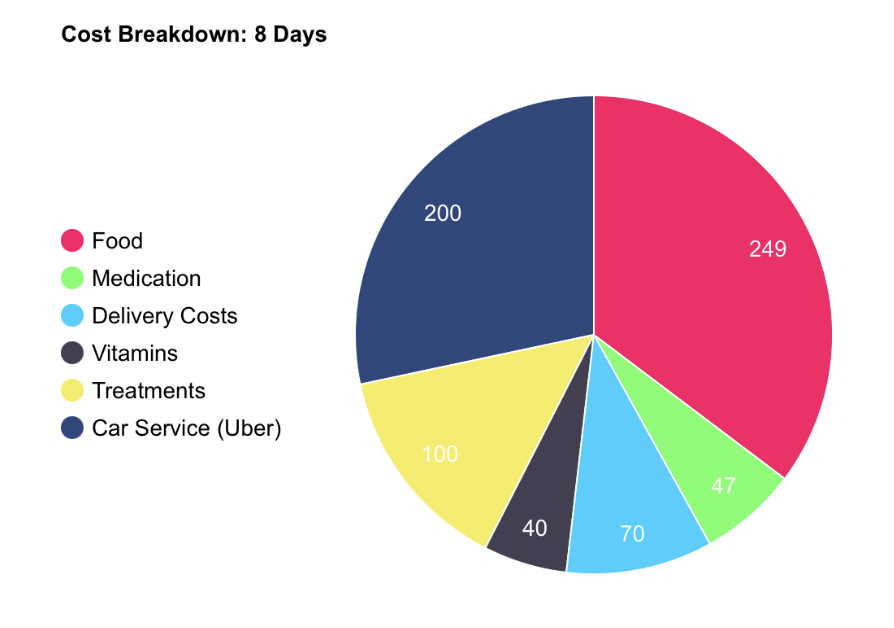
The above breakdown denotes expenses made during this bout of sickness, but are generally reflective of the categorical spending areas that increase when I am sick.
By The Numbers
Healthcare in the United States costs $12,555 per person annually. Omitted from that figure are the many ancillary services not listed strictly within the healthcare space. My loss in cognitive and muscle function requires me to get food delivered to my apartment. If I have to leave I use a car service like Uber, as I am too sick to walk, regardless of the distance.
Many of these expenses aren’t within reach for the average person; the tradeoff for maintaining full-time employment while chronically ill is the alleviation of financial burden during these bouts.
However, for the 38 million Americans living below the poverty level, and many more in the middle class, ordering takeout even for a meal is not a reality they can afford. Being sick, and properly caring for your physical wellbeing has barriers to entry in the 21st century.
Without proper immediate and preventative care, many chronic symptoms exacerbate. They result in increased future costs in the form of medication, lost wages when symptoms intensify, and piling hospital bills. As a direct result of the inflationary period in 2022, 100 million Americans– at the time 38% of the population- chose to delay or skip medical treatment and cut essentials like utilities and food to pay their medical bills.
While not all individuals are impacted by Lyme and POTS, 133 million Americans suffer from a chronic illness. The Center for Disease Control cites 6 out of 10 adults in the United States are chronically ill, 4 out of 10 suffering from 2 or more long-term conditions. Health-care, as we address these staggering, and growing, statistics, should address the total cost of operation of care.
There have been countless legislative initiatives in this light. The Patient Protection and Affordable Care Act, amongst others, served to expand health insurance coverage for individuals suffering from chronic disease, though its legislative progression is unclear at this juncture.
Most recently, the Chronic Disease Management Act of 2021 was introduced in the Senate, covering any preventative care service item used to treat a chronic condition, barring cost and efficacy stipulations. The bill never progressed.
There is also a profound opportunity cost of sickness. Along with every-day pain management and aforementioned incurred costs is the opportunity cost of a life without chronic illness.
Often, I have to log off right as the work day is over, or earlier, though I want to get a few extra hours in to prep for the week to come. I turned down demanding job offers with restrictive sick day policies or in-office mandates.
Despite achievement, I am financially bound by my illness, as are thousands of Americans suffering at the crux of an economic and burgeoning public health crisis.
Between the tests for Lyme disease and coinfections, doctor visits, and medications, the charges can add up for patients. Throughout the country, several organizations are working to make it easier to get a proper diagnosis and begin treatment. If you need financial assistance, click here to locate nonprofits that may be able to help you or your family with diagnostic testing and other Lyme-related expenses.
_______________
**Comment**
A topic that doesn’t get discussed much but is very important.
Back when my husband and I were in the thick of treatment we spent about $15K per year, per person under the care of a Lyme literate doctor. I’m certain this has increased exponentially.
Now, after we have reached “remission,” and are no longer in active treatment we spent $25K for the two of us in 2022. This includes doctor visits, supplements, prescriptions, etc. I can only imagine what this would cost if we were in active treatment.
For more: