
Low Immune Response to COVID-19 Vaccines in Patients With Impaired Immune Systems
This article is based on research findings that are yet to be peer-reviewed. Results are therefore regarded as preliminary and should be interpreted as such. Find out about the role of the peer review process in research here. For further information, please contact the cited source.The OCTAVE study – a multi-centre UK-wide trial led by the University of Glasgow and co-ordinated by the University of Birmingham’s Cancer Research UK Clinical Trials Unit – is evaluating the immune responses to COVID-19 vaccination in patients with immune-mediated inflammatory diseases such as cancer, inflammatory arthritis, diseases of the kidney or liver, or patients who are having a stem cell transplant.
The OCTAVE trial is one of the largest studies in the world so far into post-SARS-CoV-2 vaccination in immunocompromised patients and is funded by the Medical Research Council (MRC). OCTAVE is a collaborative research project involving groups in the Universities of Glasgow, Birmingham, Oxford, Liverpool, Imperial College London and Leeds Teaching Hospitals NHS Trust.
The study used a variety of state-of-the-art immune tests performed on blood samples taken before and/or after COVID-19 vaccination in around 600 people recruited across the UK. OCTAVE’s early data show that 40% of people in the patient groups studied mounted a low serological immune response after two SARS-CoV-2 vaccines.
In addition to this, the initial data shows that approximately 11% of immunocompromised patients fail to generate any antibodies 4 weeks after two vaccines. Failure to generate antibodies is found at higher proportion in some specific patient sub-groups; in particular, in patients with ANCA-Associated Vasculitis who have received Rituximab treatment. (See link for article)
_____________________
**Comment**
The proportion of patients with lower levels of antibody reactivity as per disease cohort compared to the baseline for healthy subjects:
- Those with Antineutrophil Cytoplasmic Antibody (ANCA)-Associated Vasculitis (AAV) (a group of diseases characterised by destruction and inflammation of small vessels) who are being treated with Rituximab – 90%
- Those with inflammatory arthritis – 54%
- Those undergoing Haemodialysis (the most common kind of dialysis – a procedure to remove waste products and excess fluid from the blood when kidneys stop working properly) – 21%
- Those on Haemodialysis receiving immunosuppressive therapy – 42%
- Those with Hepatic (liver) disease – 51%
- Those with solid cancer – 17%
- Those with Haematological malignancies (blood cancers) – 39%
- Those who have have undergone haemopoietic stem cell transplant (bone marrow transplant) – 33%
The article states there is no current agreed clinical cut off to measure COVID-19 vaccination response.
While Lyme/MSIDS isn’t stated specifically, please note the issues of inflammation, vasculitis, liver disease, and arthritis – ALL issues Lyme/MSIDS patients can suffer from.
https://www.medpagetoday.com/neurology/generalneurology/94151?
COVID Vaccines Linked to Functional Neurological Disorders
— These events may fuel vaccine hesitancy, experts say

Functional neurological disorders (FND) were found to be associated with COVID-19 vaccines, according to recent case reports.
Two cases of young women manifesting FND after COVID-19 vaccination were reported by Alfonso Fasano, MD, PhD, of the University of Toronto, and Antonio Daniele, MD, PhD, of Università Cattolica del Sacro Cuore in Rome, in a letter to the Journal of Neurology, Neurosurgery, and Psychiatry.
Two other published reports showed probable FND precipitated by COVID-19 vaccine administration, highlighting that FND should be considered when assessing post-vaccine neurologic symptoms, wrote Matthew Butler, MD, of Kings College London in England, and co-authors in the Journal of Neuropsychiatry and Clinical Neuroscience.
FND involves a disruption in normal brain mechanisms for controlling the body. It can be triggered by physical or emotional events including head injury, medical or surgical procedures, or vaccinations. People with FND may present with a range of neurological symptoms such as seizures, sensory abnormalities, gait or balance disturbance, or weakness. FND is distinct from feigning because patients perceive their symptoms as involuntary. (See link for article)
__________________
**Comment**
The authors predictably state, despite this seriously debilitating condition that will NOT be a rare phenomenon, that it “should not hamper ongoing vaccination efforts.”
Of course their big worry is the negative impact on vaccination campaigns. Remember, it’s all “for the greater good,” even if it isn’t good for you.
Important quote:
“In both patients, neurological symptoms were characterized by a sudden onset and overt inconsistency, as typically observed in patients with FND,” Fasano and Daniele wrote.
And of course they purposely bring in another doctor to strengthen their argument that,“correlation does not imply causation.” This of course is true; however, they must have missed the paper that shows patterns in VAERS data that provides evidence of causality.
And what about the fact the burden of proof of regarding “vaccine” safety should be upon the “vaccine” manufacturers and our public health authorities?
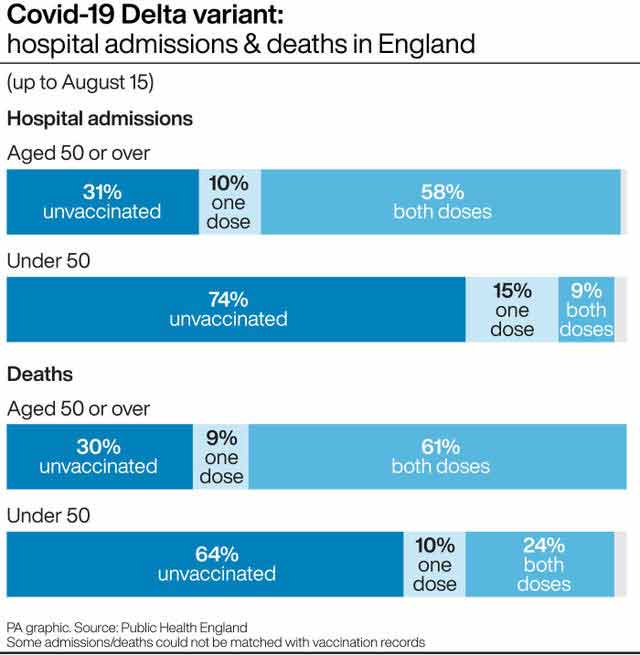
See the following graph which shows that as of August 15, 2021:
- 58% of COVID patients admitted to hospital who were over the age of 50 had received two doses of COVID injections
- 10% had received one dose
This means that partially or fully “vaccinated” individuals made up 68% of hospitalizations.
Regarding deaths in the over-50 group, the clear majority, 70%, are either partially or fully “vaccinated.”
Keep in mind that the author neglected to differentiate between age groups in the under-50 group.
A preprint published last month found waning immunity. People vaccinated in January had a 2.26 times greater risk for a breakthrough infection than those vaccinated in April.
“There are so many breakthrough infections that they dominate and most of the hospitalized patients are actually vaccinated,” says Uri Shalit, a bioinformatician at the Israel Institute of Technology (Technion) who has consulted on COVID-19 for the government.
Their answer? Boosters. However, Dvir Aran, a biomedical data scientist at Technion states “Boosters are unlikely to tame a Delta surge on their own”, and “Do not think that the boosters are the solution.”
Are you confused with the illogic yet?
The Medpage article also pointed out a paper in JAMA Neurology that discussed videos on social media showing people with severe neurological symptoms, such as convulsions and difficulty walking, after receiving a COVID-19 vaccine.
Their take-away: these videos could fuel vaccine hesitancy.
Ya think?!
Sadly, the elephant in the room that continually is ignored by mainstream medicine and the media is that there are frightening adverse reactions and deaths occurring remarkably close to injection time – minutes to months after injections. This should be cause for immediate alarm. Further, they fuel variants and don’t stop transmission or infection.
