What happens when everything adds up to a likely diagnosis of Lyme disease except the lab test results? It’s a question doctors face more often than many people realize.
Even if a patient has potentially been exposed to ticks and demonstrates symptoms that could be caused by Lyme disease, many doctors will still rely on laboratory tests to definitively determine whether a patient does or does not have the disease. And that can have serious, even deadly consequences for patients who have Lyme disease yet don’t start treatment because of negative lab test results.
So why would an infected patient test negative for Lyme disease? It turns out there are a number of reasons that could trigger false negative test results. The following article highlights some of the issues that may be at fault.
Be sure to share these potential concerns and considerations with your doctor when discussing diagnostic testing options for Lyme disease.
Why Your Lyme Disease Test Results May Be Negative Despite Persistent Symptoms
1. The test isn’t designed to detect the exact disease-causing bacteria you have.
A number of Lyme disease lab tests are designed to identify only a few species of the Borrelia bacteria that can cause Lyme disease. In the United States, for example, many tests are only designed to detect Borrelia burgdorferi, leaving out many other species that are less common yet still known to cause the disease in humans, including the recently discovered B. mayonii.
In fact, a recent internal study showed exactly how easily tests can miss infections from species other than B. burgdorferi. IGeneX researchers tested 43 samples – all positive on IGeneX Lyme ImmunoBlot tests – using the more limited Western blots prepared from the following species of Borrelia:
- burgdorferi B31
- burgdorferi B297
- mayonii
- californiensis
- afzelii
- garinii
- spielmanii
- valensiana
When only a B. burgdorferi B31 Western Blot was performed, only 14 of the 43 Lyme ImmunoBlot-positive samples were Western-Blot-positive. In other words, the B. burgdoferi Western Blot missed 29 of the 43 infections. However, when all eight Western Blots were performed, the remaining twenty-nine samples were detected.
This inability of many lab tests to cast a wide enough net of detection could result in false negative results for patients infected with different strains of disease-causing Borrelia.
2. Your test was not sensitive enough.
Many doctors and labs adhere diligently to the two-step tests – for Lyme disease that are approved by the FDA and recommended by the CDC, which involves an initial enzyme-linked immunosorbent assay (ELISA) followed by a Western blot test. Both tests are designed to detect antibodies in the patient’s blood to the B. burgdorferi bacteria and, according the CDC, both must be positive for a patient to be diagnosed with Lyme disease.
However, recent studies have raised concerns about the accuracy of these tests, particularly the ELISA, which has been found to have a poor sensitivity rate, or ability to detect antibodies in the blood. Recent studies, in fact, report that the ELISA and Western blot can miss up to 60 percent of well-defined Lyme disease cases.
3. Indirect testing can be more limited than direct testing.
Both tests used in the CDC recommended two-step process are indirect methods of diagnosis—meaning they do not detect the actual Lyme disease bacteria itself but, instead, measure the body’s immune-system response to the presence of disease-causing bacteria. However, a number of factors can prevent the body from producing antibodies, including the following:
- Timing: If conducted in the early stages of Lyme disease, a patient’s body may not have developed a sufficient enough number of antibodies to detect. This issue can be compounded by the lack of sensitivity of the ELISA test.
- Immunity Suppression: The saliva of infected ticks contains specific immune-suppressing components that can delay or prevent the activation of a person’s immune response. These components are designed to prevent the body from effectively “fighting off” the Lyme disease-causing bacteria so it has a chance to take hold.
- Antibiotics: If patients are taking antibiotics at the time of the Lyme disease test, they may not produce enough antibodies to be detected by the test.
- Modified Form of Borrelia: In some patients, the Borreliabacteria will transform into a cyst, which will prevent the body’s immune system from producing antibodies.
- Weakened Immune System: False negatives can also result in patients in whom the immune system is weakened or compromised due to coinfection with another illness.
- Seronegative patients: These patients do not produce antibodies.

Direct testing methods can eliminate some of these variables because they don’t rely on the body’s response to a pathogen but rather look for the presence of the disease-causing bacteria directly. Polymerase chain reaction (PCR) assays, for example, are used to identify Lyme bacteria in the patient’s blood or urine.
4. Different labs can produce different results.
When it comes to testing for Lyme disease, the quality of the lab conducting the test can also affect the reliability of the results. That’s because different labs use different protocols and techniques to perform each test. Those with more advanced procedures and capabilities provide higher levels of accuracy and precision across various types of tests.
By improving diagnostic precision, clinicians are not only able to more accurately detect Lyme infection but, in some cases, the specific stage of a patient’s Lyme disease infection.
5. Co-infections cause complexities.
Common Lyme disease co-infections include Babesiosis, Powassan, Bartonellosis, Ehrlichiosis, Anaplasmosis, and Rickettsiosis.
In some cases, they may not have Lyme disease at all, but one of these other illnesses instead. Depending on a patient’s symptoms, doctors should consider the potential of a co-infection as a factor when all symptoms point to Lyme disease but test results are negative.
6. TBRF can cause a negative result.
The disease Tick-Borne Relapsing Fever is caused by a similar but totally separate species of Borrelia to the bacterium that causes Lyme disease, and also causes Lyme-like symptoms. However, if a patient with TBRF takes a Lyme disease test, the TBRF will not show up, causing the Lyme test to be negative even though the patient is still sick with an infection.
An early and accurate diagnosis is key
For patients and doctors, being aware of the many factors that can influence Lyme disease lab tests can better inform your perspective and reliance on the results. Doctors should consider multiple types of tests, a panel approach, to increase the chances of detecting the disease.
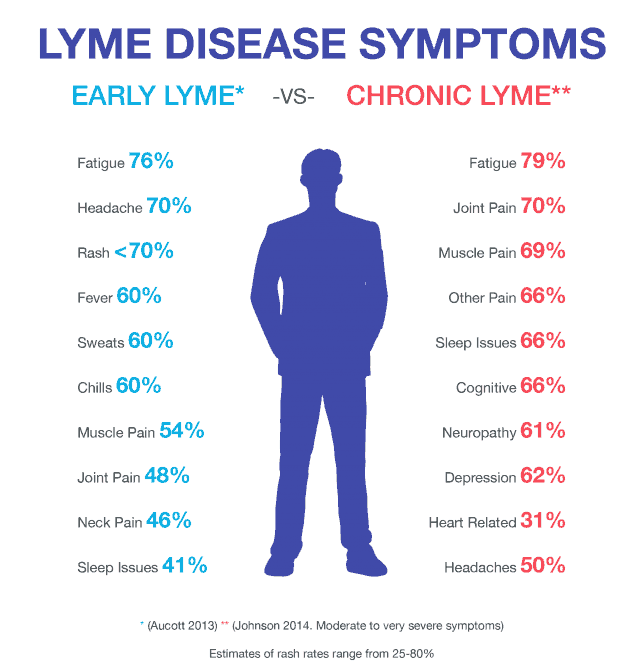
Additionally, they should always consider the patient’s Lyme disease test results in conjunction with their current or previously reported symptoms. Remember, Lyme disease causes symptoms such as fever, chills, headache, fatigue, muscle and joint aches, and swollen lymph nodes. (An erythema migrans or “EM” rash may also appear, but note – at least 20% of patients don’t experience this rash at all.)
Finally, doctors should also consider risk factors that heighten someone’s probability of exposure to ticks or regions where Lyme disease and other tick-borne diseases are prevalent.
For more information on getting the proper diagnosis and treatment for your tick-borne disease, read the IGeneX blogs The Importance of Getting the Right Diagnosis and How to Find Doctors Who Can Help with Your Tick-Borne Disease.
Additional Resources
_______________________
**Comment**
More great information here on why serology testing doesn’t work: https://madisonarealymesupportgroup.com/2020/12/15/lyme-disease-is-a-small-vessel-disease-dr-klemann/
The problems of Lyme/MSIDS testing have been the bane of patients for over 40 years and other studies have shown an even poorer outcome of current testing than what was mentioned in this article: https://madisonarealymesupportgroup.com/2020/03/01/study-cdcs-2-tier-lyme-testing-inaccurate-in-more-than-70-of-cases/
There is also a law-suit on current testing listed in the comment section of this article: https://madisonarealymesupportgroup.com/2020/05/27/letter-to-cdc-dr-beard-why-isnt-direct-detection-of-lyme-disease-a-priority/
There has been wide-spread suppression of direct testing for Lyme disease putting patients in a juggernaut of unbelievable proportions.
For more: https://madisonarealymesupportgroup.com/2020/05/06/more-cdc-lip-service-on-lyme-testing/
https://madisonarealymesupportgroup.com/2019/03/07/yet-another-worthless-study-showing-2-tiered-lyme-testing-can-not-rule-infection-out/


 Ever since the alleged pandemic erupted this past March the mainstream media has spewed a non-stop stream of misinformation that appears to be laser focused on generating maximum fear among the citizenry. But the facts and the science simply don’t support the grave picture painted of a deadly virus sweeping the land.Yes we do have a pandemic, but it’ a pandemic of ginned up pseudo-science masquerading as unbiased fact. Here are nine facts backed up with data, in many cases from the CDC itself that paints a very different picture from the fear and dread being relentlessly drummed into the brains of unsuspecting citizens.
Ever since the alleged pandemic erupted this past March the mainstream media has spewed a non-stop stream of misinformation that appears to be laser focused on generating maximum fear among the citizenry. But the facts and the science simply don’t support the grave picture painted of a deadly virus sweeping the land.Yes we do have a pandemic, but it’ a pandemic of ginned up pseudo-science masquerading as unbiased fact. Here are nine facts backed up with data, in many cases from the CDC itself that paints a very different picture from the fear and dread being relentlessly drummed into the brains of unsuspecting citizens.