“The entire world simply claimed that there was no immunity…..that wasn’t science, but pure speculation based on a gut feeling that was then parroted by everyone.” Beda Stadler
It’s important to know that vaccines have been used at least 5 times (Africa, Brazil, Mexico, and India) in the past to reduce fertility, according to Dr. Hoffe.
Vaccine whistle-blower from Glaxo Smith Kline (GSK): New vaccine could well cause sterility in 97% of women… While also affecting men’s sexual organs too... (Clear medical explanation)…
Please listen to the entire thing but if you only want the part about sterility, fast-forward to 4:30 where you will learn that these various antigens can shrink testicles and prostates, lower testosterone levels, and make women infertile. According to the baboon experiment it showed that vaccinated men can make unvaccinated women infertile, so you don’t even need the vaccine to become infertile. Evidently there is a delayed reaction until 7-10 yrs later when there will be an explosion of infertility.
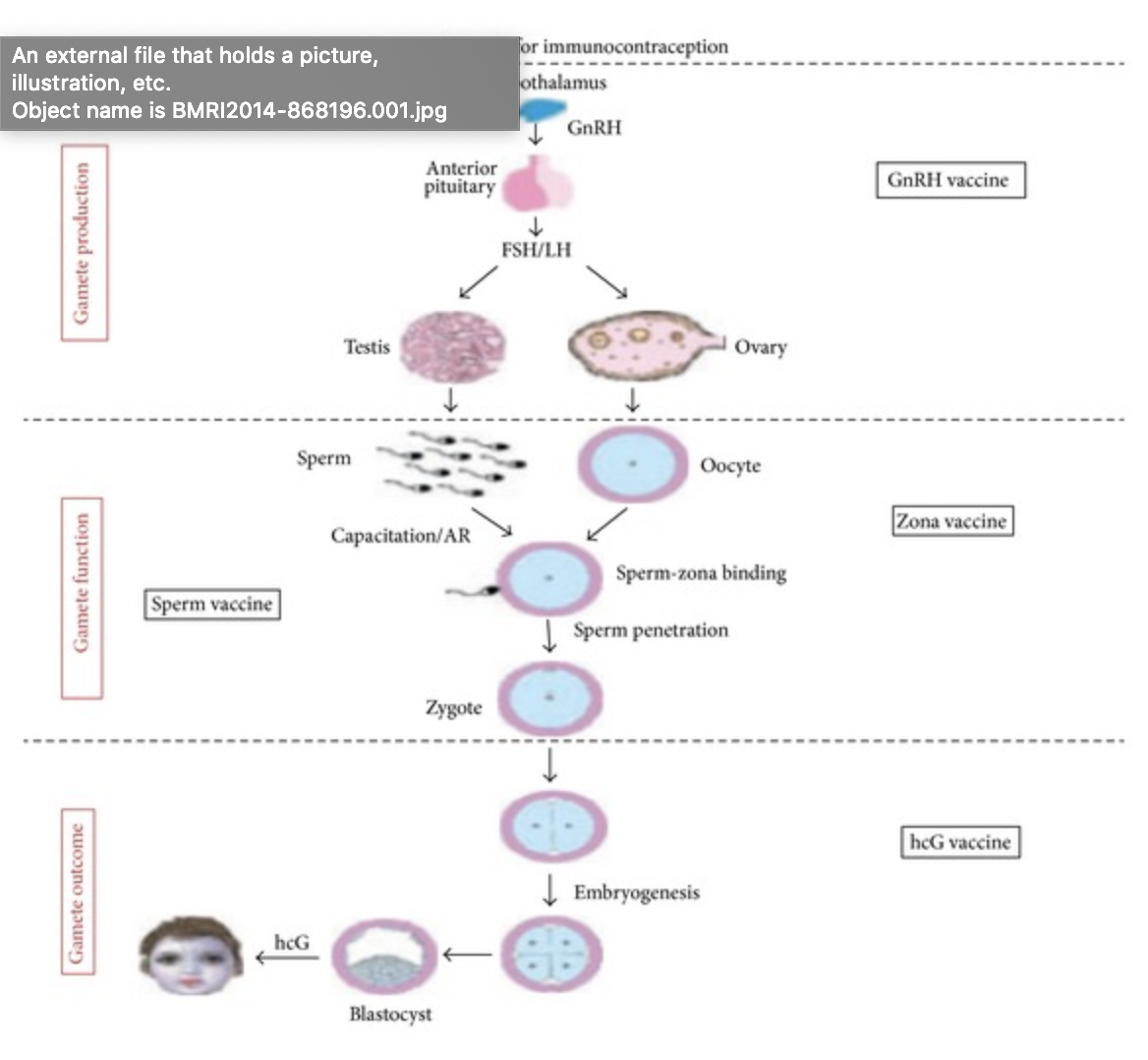
The rapidly increasing global population has bowed the attention of family planning and associated reproductive health programmes in the direction of providing a safe and reliable method which can be used to limit family size. The world population is estimated to exceed a phenomenal 10 billion by the year 2050 A.D., thus presenting a real jeopardy of overpopulation with severe implications for the future. Despite the availability of contraceptive methods, there are over one million elective abortions globally each year due to unintended pregnancies, having devastating impact on reproductive health of women worldwide. This highlights the need for the development of newer and improved contraceptive methods. A novel contraceptive approach that is gaining substantial attention is “immunocontraception” targeting gamete production, gamete outcome, or gamete function. Amongst these, use of sperm antigens (gamete function) seems to be an exciting and feasible approach. However, the variability of immune response and time lag to attain titer among vaccinated individuals after active immunization has highlighted the potential relevance of preformed antibodies in this league. This review is an attempt to analyze the current status and progress of immunocontraceptive approaches with respect to their establishment as a future fertility control agent.
___________________
**Comment**
I’ve been told that antibodies to either hCG or GnRH will cause infertility. In the case of hCG, conception can still take place, but the developing embryo will abort. GnRH, a hypothalamic factor that acts on the pituitary, has also been found in seminal fluid and it appears to increase sperm interaction with the outer layer, or zona pellucida, of the egg. Antibodies to GnRH would prevent conception and may disrupt pituitary action of GnRH and extra pituitary action of GnRH in the gut. GnRH is involved in many other systems. hCG is also produced by cancer cells.
The video came out in May. I have not heard if it has been substantiated but feel this is a grave topic that needs recognition and investigation. The implications are very, very great and should concern us all.
UPDATE 2/1/24: In an effort to be balanced, please read this 48 page exposé on David Martin which shows he has served as an advisor to central banks, global economic forums, national governments, and the World Bank, and has connections to the WEF serving its interests through numerous companies he has worked with.
“The mark of an educated mind is to be able to entertain a thought without accepting it.” ~ Aristotle.
The United States blames China for the virus and China blames the U.S., but the truth is that both countries are engaged in a network of unethical coronavirus gain-of-function research that dates back twenty-one years.
The CDC controls the coronavirus patent and off-shored unethical gain-of-function research to China
National Intelligence Analyst David E. Martin, Ph.D, the developer of linguistic genomics, is an expert at understanding the intent of communication. For twenty-one years, David Martin studied biological weapon activity, and the timeline of events behind the race to control and profit from coronaviruses.
Martin’s operation maintained a series of inquiries into every individual and every company that is involved in anything related to biological and chemical weapons throughout 168 countries. The operation investigated over a million patents that were put into a digital searchable format provided by IBM.
Martin found that one third of all patents were functional forgeries,containing linguistic variations, but covering the same subject matter. Peculiarly, in 1999, patents on coronaviruses exploded onto the scene as the race to control and profit from pathogens accelerated into the 21st century. The coronavirus manipulation began in 1999 with Ralph Barrick, researcher at the University of North Carolina Chapel Hill. His manipulation of coronavirus led to chimeric discoveries that allowed the virus to have enhanced gain-of-function properties.
In 2003, a coronavirus outbreak occurred in Asia, and the CDC discovered just how profitable a coronavirus outbreak could be, from the way people can be manipulated through pandemic messaging, how they can be controlled by government mandates, and how sickness can be treated and used for vaccination experiments. That’s why in 2003, the CDC sought to patent coronavirus so they could control the proprietary rights to the disease, to the virus, and to its measurement and detection.
From 2003 to 2018, Dr. Anthony Fauci, Ralph Barrick, and the CDC, controlled 100 percent of the cash flow behind the industrial complex of coronavirus.
On April 25, 2003, the U.S. CDC filed a patent on coronavirus transmitted to humans. Granted, it is illegal to manufacture coronaviruses, for this violates laws and treaties on developing biological and chemical weapons. It is also illegal to patent nature such as naturally-occurring coronaviruses. The CDC had no choice but to make their research confidential so they could control who had access to their experiments so they could skirt the law.
This is why the CDC filed a petition with the patent office to make their patent confidential. The CDC made their patent on coronavirus, its detection, and a kit to measure it, a secretive, controllable endeavor. With this secretive patent, the CDC controlledwho was authorized to make inquiries about coronavirus. Their secret patent constrained anyone from using the virus — giving the CDC the means, the motive and the monetary gain that would ultimately be used to turn coronavirus from a naturally-occurring pathogen to a profitable weapon of sickness and societal control.
NIH subcontracts with China to continue unethical gain-of-function research
From 2012 and 2013, the National Institutes of Health came to the moral and ethical realization that their research efforts on coronavirus gain-of-function should be suspended. This is when federal funds to Harvard, Emory and the University of North Carolina Chapel Hill were suspended, as a moratorium was placed on coronavirus gain-of-function research in the U.S. This did not stop the research altogether. In 2014 and 2015, the research was off-shored to China, to the Wuhan Institute of Virology.
The NIH ran money through a series of cover organizations to subcontract with the Wuhan Institute of Virology — the site of the original covid-19 outbreaks in 2019. Because the CDC owns the secretive patent on coronavirus measurement and detection, they have the power to mislead the world with inaccurate testing protocols, while controlling economies and people’s lives until they are worn down enough to submit to upcoming inoculations.
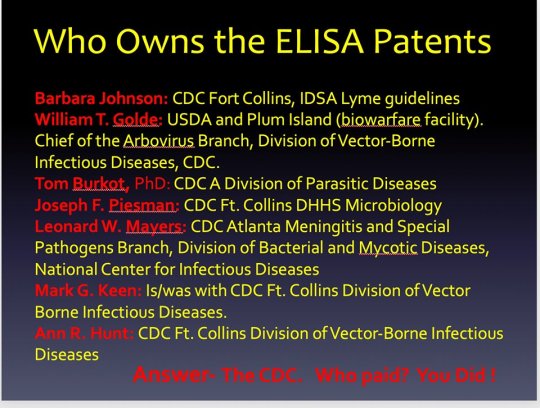
The information is important not just due to the mishandling of COVID but with other diseases including Lyme/MSIDS. The same CDC players have severe conflicts of interest and lie – regularly on nearly every aspect of these illnesses. They have lost ALL credibility and should be disbanded.
Until the Bayh-Dole Act is repealed, among other things, we will never have transparent work done that can be trusted. Too many people that are setting public policy and making decisions for patients have vested interests clouding their judgement.
The unprecedented global social and economic crisis triggered by the COVID-19 pandemic poses grave risks to the nutritional status and survival of young children in low-income and middle-income countries (LMICs). Of particular concern is an expected increase in child malnutrition, including wasting, due to steep declines in household incomes, changes in the availability and affordability of nutritious foods, and interruptions to health, nutrition, and social protection services.1
One in ten deaths among children younger than 5 years in LMICs is attributable to severe wasting because wasted children are at increased risk of mortality from infectious diseases.2
Before the COVID-19 pandemic, an estimated 47 million children younger than 5 years were moderately or severely wasted, most living in sub-Saharan Africa and south Asia.3
The economic, food, and health systems disruptions resulting from the COVID-19 pandemic are expected to continue to exacerbate all forms of malnutrition. Estimates from the International Food Policy Research Institute suggest that because of the pandemic an additional 140 million people will be thrown into living in extreme poverty on less than US$1·90 per day in 2020.4
According to the World Food Programme, the number of people in LMICs facing acute food insecurity will nearly double to 265 million by the end of 2020.5
Sharp declines are expected in access to child health and nutrition services, similar to those seen during the 2014–16 outbreak of Ebola virus disease in sub-Saharan Africa.6
Early in the COVID-19 pandemic, UNICEF estimated a 30% overall reduction in essential nutrition services coverage, reaching 75–100% in lockdown contexts, including in fragile countries where there are humanitarian crises.7
The accompanying call to action on child malnutrition and COVID-19 from leaders of four UN agencies8 in The Lancet is an important first step for the international community. Alongside these efforts, the Standing Together for Nutrition consortium, a multidisciplinary consortium of nutrition, economics, food, and health systems researchers, is working to estimate the scale and reach of nutrition challenges related to COVID-19. These efforts link three approaches to model the combined economic and health systems impacts from COVID-19 on malnutrition and mortality: MIRAGRODEP’s macroeconomic projections of impacts on per capita gross national income (GNI);4 microeconomic estimates of how predicted GNI shocks impact child wasting using data on 1·26 million children from 177 Demographic Health Surveys (DHS) conducted in 52 LMICs between 1990–2018;9 and the Lives Saved Tool (LiST), which links country-specific health services disruptions and predicted increases in wasting to child mortality.10
What do our initial analyses and estimates suggest?
First, the MIRAGRODEP projections suggest that even fairly short lockdown measures, combined with severe mobility disruptions and comparatively moderate food systems disruptions, result in most LMICs having an estimated average 7·9% (SD 2·4%) decrease in GNI per capita relative to pre-COVID-19 projections.4
Second, the microeconomic model projections indicate that decreases in GNI per capita are associated with large increases in child wasting.9
Our own analyses, based on these estimates applied to 118 LMICs, suggest there could be a 14·3% increase in the prevalence of moderate or severe wasting among children younger than 5 years due to COVID-19-related predicted country-specific losses in GNI per capita. We estimate this would translate to an additional estimated 6·7 million children with wasting in 2020 compared with projections for 2020 without COVID-19; an estimated 57·6% of these children are in south Asia and an estimated 21·8% in sub-Saharan Africa.
Third, when the projected increase in wasting in each country is combined with a projected year average of 25% reduction in coverage of nutrition and health services, we estimate there would be 128 605 (ranging from 111 193 to 178 510 for best and worst case scenarios) additional deaths in children younger than 5 years during 2020, with an estimated 52% of these deaths in sub-Saharan Africa. The range reflects coverage scenarios, as previously described by Roberton and colleagues,10 using a low of 15% and high of 50% disruption in vitamin A supplementation, treatment of severe wasting, promotion of improved young child feeding, and provision of micronutrient supplements to pregnant women.
Our projections emphasise the crucial need for the actions to protect child nutrition that are urged by the UN leaders in the accompanying Comment.8 These actions require rapid mobilisation of domestic and donor resources at a time when most national economies are reeling from COVID-19-related losses. In 2017, the Word Bank estimated that $7 billion per year over 10 years is needed to reach the global Sustainable Development Goal nutrition targets.11 These estimates need to be revised upwards to overcome COVID-19-related setbacks.
The COVID-19 pandemic is expected to increase the risk of all forms of malnutrition. The wasting-focused estimates we present here are likely to be conservative, given that the duration of this crisis is unknown, and its full impacts on food, health, and social protection systems are yet to be realised. The disruption of other health services during lockdowns will further compromise maternal and child health and mortality,10 and with the deepening of economic and food systems crises, other forms of malnutrition, including child stunting, micronutrient malnutrition, and maternal nutrition, are expected to increase.1
Without adequate action, the profound impact of the COVID-19 pandemic on early life nutrition could have intergenerational consequences for child growth and development and life-long impacts on education, chronic disease risks, and overall human capital formation.12
Forthcoming analyses by this consortium will examine a range of diet and nutrition outcomes in women and young children and provide consensus advice on multisectoral actions and resources needed to recover and support optimal nutrition now and into the future.
The work on this study was supported by a grant from the Children’s Investment Fund Foundation (CIFF). The funders were not involved in the writing of this Comment. RH and MS report grants from the Bill & Melinda Gates Foundation unrelated to the topic of this Comment. We declare no other competing interests.
______________________
**Comment**
Others are suffering due to the continuing over-arching actions of governments shuttering businesses and stopping life.
“Nationwide, federal and local officials are reporting alarming spikes in drug overdoses — a hidden epidemic within the coronavirus pandemic,” the Washington Post article reads.
In their editorial Greenhalgh et al advise that surgical masks should be worn in public to prevent some transmission of covid-19,1 adding that we should sometimes act without definitive evidence, just in case. Two side effects of wearing face masks in public have already been highlighted:
Wearing a mask may give a false sense of security and make people adopt a reduction in compliance with other important infection control measures1
People must avoid touching their masks and adopt other management measures, otherwise masks are counterproductive23
Other potential side effects that we must consider, however, are:
The quality and volume of speech between people wearing masks is considerably compromised and they may unconsciously come closer
Wearing a mask makes the exhaled air go into the eyes. This generates an impulse to touch the eyes. If your hands are contaminated, you are infecting yourself
Face masks make breathing more difficult.4 Moreover, a fraction of carbon dioxide previously exhaled is inhaled at each respiratory cycle. Those phenomena increase breathing frequency and deepness, and they may worsen the burden of covid-19 if infected people wearing masks spread more contaminated air. This may also worsen the clinical condition of infected people if the enhanced breathing pushes the viral load down into their lungs
The innate immunity’s efficacy is highly dependent on the viral load.5 If masks determine a humid habitat where SARS-CoV-2 can remain active because of the water vapour continuously provided by breathing and captured by the mask fabric, they determine an increase in viral load (by re-inhaling exhaled viruses) and therefore they can cause a defeat of the innate immunity and an increase in infections.
The context of the current covid-19 pandemic is very different from that of the “parachutes for jumping out of aeroplanes.”16 It is necessary to quantify the complex interactions that may well be operating between positive and negative effects of wearing surgical masks at population level. It is not time to act without evidence.
“In order to use those special masks the medical staff are trained and educated, so it is important that the masks are worn properly,” Azap said. “I see people wearing the N95 in planes and airports and I have never seen a single person wearing it right!”
Azap said due to the lack of masks, they are often reused for a few days and in some cases washed and worn again, which is the biggest invitation for infections.