Prof. Holly Ahern’s Lyme disease comments to Australian Senate
2/5/25
The Australian Senate has launched an inquiry into the access to diagnosis and treatment for people in Australia with tick-borne diseases. Professor Holly Ahern of the United States recently submitted the following written comments and was also asked to give verbal remarks. (See video at end of this article.)
Dear Committee Members:
I am a scientist, professor of microbiology, and co-founder of a Lyme disease advocacy organization in New York State. I am also the Scientific Advisor for the Focus on Lyme Foundation in Arizona, which has funded research on several projects directed at improving the state of diagnostic testing for Lyme disease and other tick-borne illnesses.
I have served on several state and federal committees convened to address the growing problem of tick-borne diseases in the United States, most recently the 2022 Dept. of Health and Human Services, Tick Borne Disease Working Group (TBDWG).
But most of all, I am mother of a daughter who went from a record setting collegiate All American swimmer to bed bound and disabled over the course of only a few weeks. She lost years of her life as a result of flawed medical guidelines that prioritize care for patients early in the infection, while providing only minimal guidance for the diagnosis and care of patients in later stages of the disease.
In my daughter’s case, we saw the tick bite but she developed no rash. Fever, profound fatigue, widespread pain, and other symptoms began months later, and were attributed to a viral illness. The difficulties we faced in getting her illness diagnosed and appropriately treated in 2010 match those of hundreds of thousands of other people with Lyme disease in the United States and Europe, and also in Australia.
Biologically complex organism
Lyme disease is a bacterial infection caused by a microbe with global distribution. They are transmitted to humans by several species of tick. The bacteria are biologically complex. They adapt and survive in environments that would kill most other bacteria.
During human infection, some subgroups (genospecies) of these bacteria linger in the bloodstream, while others disseminate to connective tissue-rich areas of the body. Regardless, infection triggers profound immune system and other physiological events, leading to a wide range of symptoms that vary significantly among patients and can be quite severe.
The standard medical definition implies that the overwhelming majority of Lyme borreliosis (Lyme disease) patients are infected with the same bacteria and have the same uniform disease presentation, which is straightforward to diagnose and treat. As defined, Lyme disease is caused by only a few specific genospecies of Borrelia (now named Borreliella). Several other genospecies of Borrelia are associated with diseases collectively referred to as “Relapsing Fever borreliosis.”
Differences between the two diseases are subtle. Relapsing Fever Borrelia fail to produce the skin manifestation (erythema migrans or “bull’s-eye” rash) that is noted in Lyme disease; however, other symptoms are very similar. Existing diagnostic tests for Lyme disease don’t detect infections caused by Relapsing Fever Borrelia.
Thus, a patient may be bitten by a tick and infected with a Relapsing Fever Borrelia, such as B. miyamatoi, show all the symptoms that a patient with Lyme disease would have, but may not be diagnosed or treated for the infection because the EM rash did not appear and/or the standard lab tests for Lyme disease were negative. (See link for article)
MEDICAL DETECTIVE: The complex role of Bartonella in chronic illness, part 1
This article was originally posted on Dr. Richard Horowitz’s Medical Detective Substack. It is Part 1 of a 5-part series. You can find more helpful content by subscribing here.
Bartonella is the third “B” of the triad found in the vast majority of my chronically ill patients who suffer from chronic Lyme disease/PTLDS, along with Borrelia and Babesia.
A gram-negative intracellular bacteria, it’s controversial and misunderstood and has been throwing a monkey wrench into my treatments for decades.
I barely remember learning about it in medical school, except when they were teaching me about cat scratch fever in children that would cause small, localized rashes (papules) at the site of the scratch with swollen lymph nodes and fevers.
It would be treated with a short course of antibiotics like azithromycin. These images show classical cat scratch disease before and after treatment when the lesions are starting to crust up.
[From: Mazur-Melewska K, Mania A, Kemnitz P, Figlerowicz M, Służewski W. Cat-scratch disease: a wide spectrum of clinical pictures. Postepy Dermatol Alergol. 2015 Jun;32(3):216-20. doi: 10.5114/pdia.2014.44014. Epub 2015 Jun 15. PMID: 26161064; PMCID: PMC4495109.]
Unfortunately, Bartonella infections rarely resemble this one particular manifestation, or the general medical community would be diagnosing and treating it a lot more often.
It is a very tricky bacteria, and, like Lyme disease, has found a way to not only avoid immune recognition, but change its clinical characteristics so it resembles a broad range of other diseases.
Immune Evasion by Bartonella
Bartonella is referred to as a “stealth bacteria” because it evades the immune system by living inside red blood cells (intraerythrocytic persistence), blood vessel walls (inflaming them, causing vasculitis), endothelial cells, fibroblasts, epithelial cells of the skin (causing the classic Bartonella rashes described below), macrophages (immune cells that play a critical role of initiating and maintaining an inflammatory response, as well as potentially resolving inflammation) and bone marrow cells.
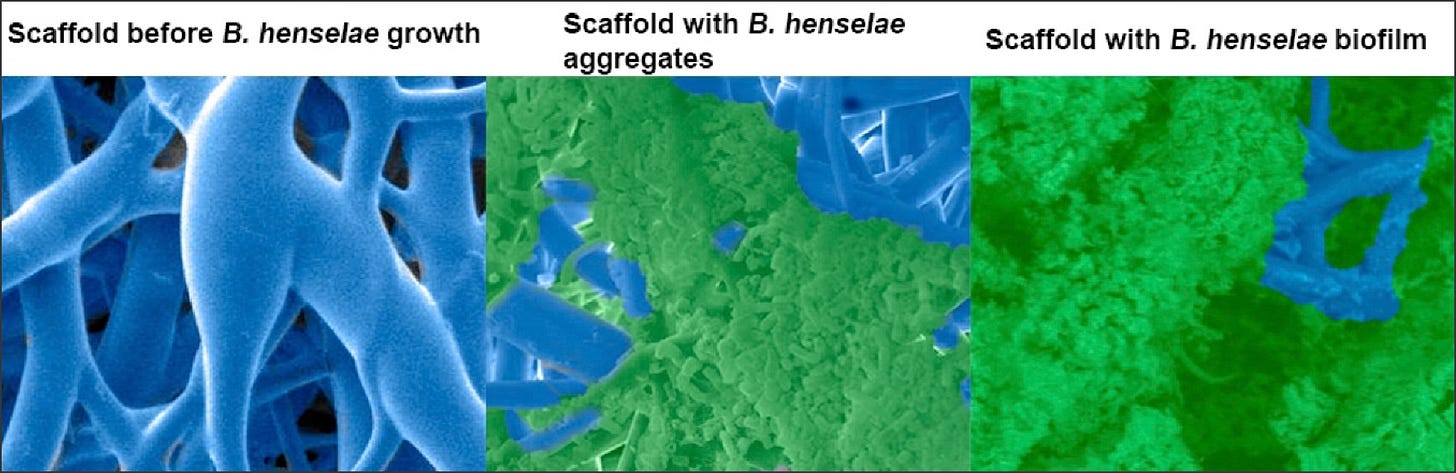
So it can hide throughout the body in areas where the immune system doesn’t easily penetrate and recognize the bacteria, not to mention, it can exist under biofilms in persister forms like Borrelia. Biofilms protect the bacteria from immune recognition and the effects of antibiotics.
Bartonella can manipulate host cell interactions to hide from immune detection by altering its surface proteins to avoid recognition (like Lyme disease), and possesses unique fat and sugar molecules (lipopolysaccharides) that minimize immune response activation; this often leads to prolonged, asymptomatic infections that can be difficult to diagnose with standard tests (it can hide in the body for years in some patients without symptoms), and then reactivate under certain conditions.
The patient below was in remission for one year after doing an 8-week course of double dose dapsone combination therapy (DDDCT), and then reactivated after being treated with antibiotics for a skin infection. This skin rash emerged when he got treated for cellulitis, which had nothing to do with his initial Lyme infection. You can see the classical Bartonella “stretch marks.”
[From: Horowitz, R.I.; Fallon, J.; Freeman, P.R. Comparison of the Efficacy of Longer versus Shorter Pulsed High Dose Dapsone Combination Therapy in the Treatment of Chronic Lyme Disease/Post Treatment Lyme Disease Syndrome with Bartonellosis and Associated Coinfections. Microorganisms 2023, 11, 2301. https://doi.org/10.3390/microorganisms11092301%5D
Reactivation often happens when the immune system is unable to control the infection, due in part to the immunosuppressive nature of the bacteria.
I’ve found multiple species of Bartonella in our sickest patients leading to chronic variable immune deficiency (CVID), just as I’ve found Borrelia causing immune suppression, along with mold toxicity and Long Covid affecting immune functioning.
The multisystemic nature of Bartonella infections
When we see patients with Bartonella, as I mentioned, it has no resemblance whatsoever with the classical cat-scratch disease I learned about in medical school. Bacteria like Bartonella cause similar symptoms to those seen in chronic Lyme disease, presenting as a “great imitator.”
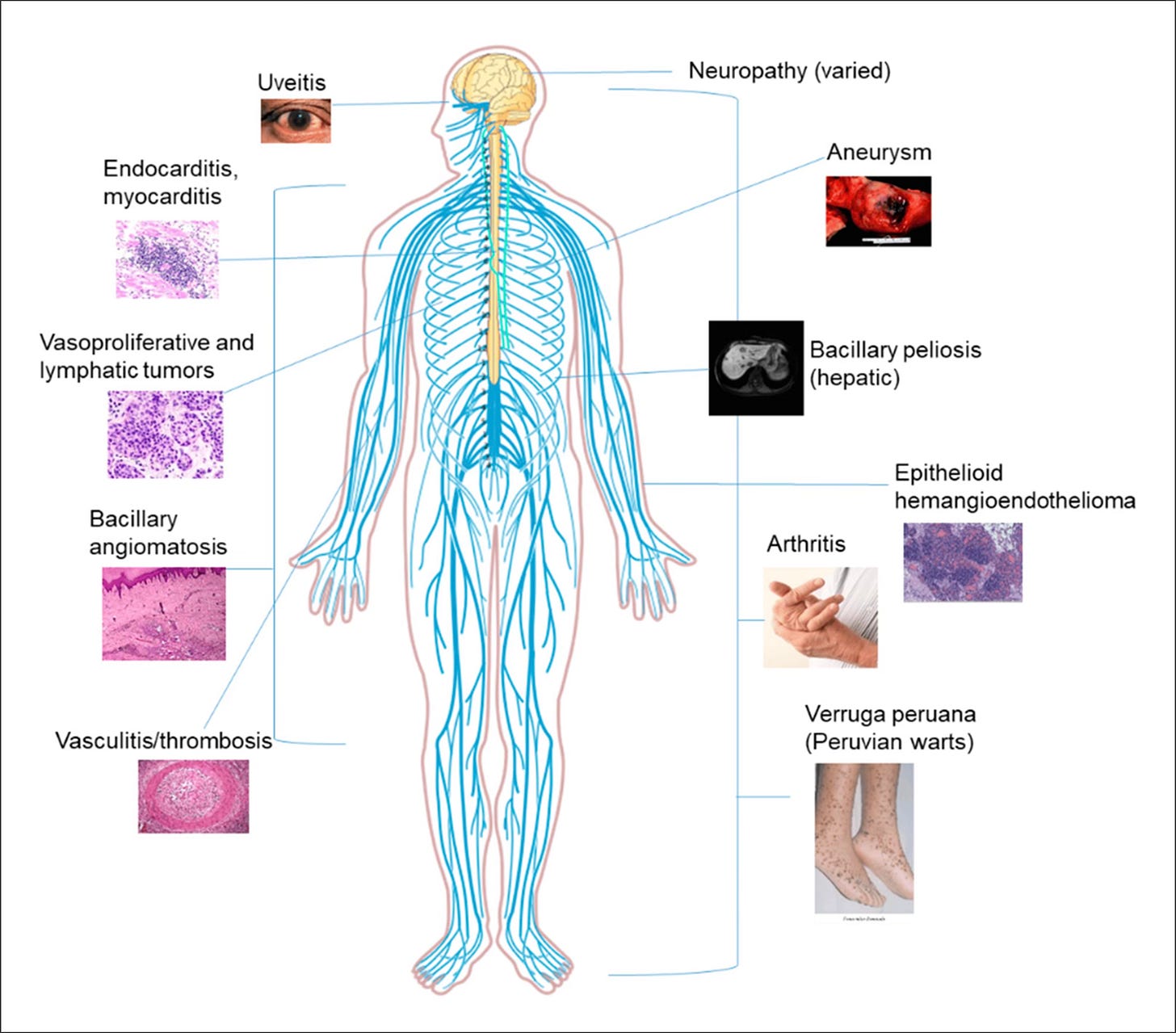
It can result in chronic fatiguing, musculoskeletal, cardiopulmonary, neuropsychiatric illness and can cause fevers, chills, fatigue, headaches, muscle/joint and nerve pain, cognitive difficulties, insomnia, depression, anxiety, and cause inflammation in every body system imaginable, just like Lyme disease, Borrelia burgdorferi, does.
There can also be inflammation in the eyes (optic neuritis, conjunctivitis, uveitis, arterial and venous occlusions); the brain, surrounding structures and spinal cord (meningitis, encephalitis, transverse myelitis, seizure disorders), with associated Bartonella “rage” and psychosis (Bartonella, like Lyme disease, can cause a broad range of psychiatric manifestations, including but not limited to severe depression, anxiety, Obsessive Compulsive Disorder, Bipolar disorder and schizophrenia with psychosis).
It also can cause inflammation in the muscles (myalgias), joints (arthritis, osteomyelitis), nerves (neuropathy) and blood vessels (vasculitis), as well as the heart valves (endocarditis, including culture negative endocarditis), heart muscle (myocarditis), and sac surrounding the heart (pericarditis) causing chest pain with masses in the chest (mediastinum) and lymph nodes resembling non-Hodgkins lymphoma.
Even the gastrointestinal tract can be affected (nausea, vomiting, weight loss, bleeding), as can the liver (hepatitis), spleen (splenitis, enlargement), and skin, which oftentimes shows signs of inflammation (stretch marks, i.e. striae; granulomas, hard fibrous areas over the knuckles, elbows, and Bacillary angiomatosis, which are tumor-like masses, raised dark areas, papules, nodules, and lesions in the skin, bones, and organs).
Bartonella is a frequently found infection in those suffering from chronic Lyme disease—I’ve seen it in up to 80-90% of all of my chronically ill patients these days and should be considered in any and all cases of FUO (fever of unknown origin).
[From: Cheslock, M.A.; Embers, M.E. Human Bartonellosis: An Underappreciated Public Health Problem? Trop. Med. Infect. Dis. 2019, 4, 69. https://doi.org/10.3390/tropicalmed4020069%5D
Transmission of Bartonella
Part of the reason Bartonella has been a controversial topic in the Lyme community–at least among certain physicians and researchers–is because there has only been one study to date regarding tick transmission of the bacteria, and this was in European species of deer ticks (Ixodes ricinus) with one species, called Bartonella birtlesii.
The bacteria is, however, being found in ticks throughout the world, and other studies have shown the bacteria in different ticks and in chronic Lyme disease patients.
When I was co-chair of the HHS Tick-borne Disease Working Group (TBDWG) back in 2018, I had to fight to get Bartonella included as a co-infection of importance; whether all species are able to be transmitted by ticks or not, makes no difference.
Why? To date, the number of species able to transmit Bartonella keeps increasing over the years, and most of us are exposed to these vectors on a regular basis. The most common vectors transmitting the bacteria are fleas, mites, lice, keds (not the sneakers!), spiders, red ants, ticks (probable), sand flies, black and yellow flies, and mosquitoes.
Bartonella is showing up in a broad range of vectors, so it’s possible to get exposed from many different sources. That is why the vast majority of my sick patients are testing positive for it. In fact, for most of us living on this planet, I daresay we’ll all likely be exposed to Bartonella at some point during our lives. How we handle it, and whether we get symptoms, will depend on how our immune system is functioning.
Testing for multiple Bartonella species
The table below shows some of the most common species of Bartonella seen in human disease. This is not comprehensive, as there are now at least 45 species of Bartonella, and 18 of them or more are pathogenic [capable of causing disease].
Some of the most common ones are: B. henselae (Cat scratch disease, CSD; endocarditis, neuroretinitis, lymphadenopathy), B. quintana (Trench fever, endocarditis, bacillary angiomatosis [BA]), B. clarridgeiae (bacteremia, endocarditis, CSD, chest wall abscess), B. elizabethae (endocarditis, neuroretinitis), B. bacilliformis (Carrion’s disease), B. koehlerae (endocarditis, including culture negative endocarditis), B. vinsonii subsp (bacteremia, endocarditis, fevers, neurological symptoms), B. berkhoffi (endocarditis, bacteremia, neurological symptoms), and B. grahamii (neuroretinitis).
[From: Rebekah L. Bullard, Emily L. Olsen, Mercedes A. Cheslock, Monica E. Embers, Evaluation of the available animal models for Bartonella infections, One Health, Volume 18, 2024,100665, ISSN 2352-7714, https://doi.org/10.1016/j.onehlt.2023.100665.%5D
How do we test for Bartonella?
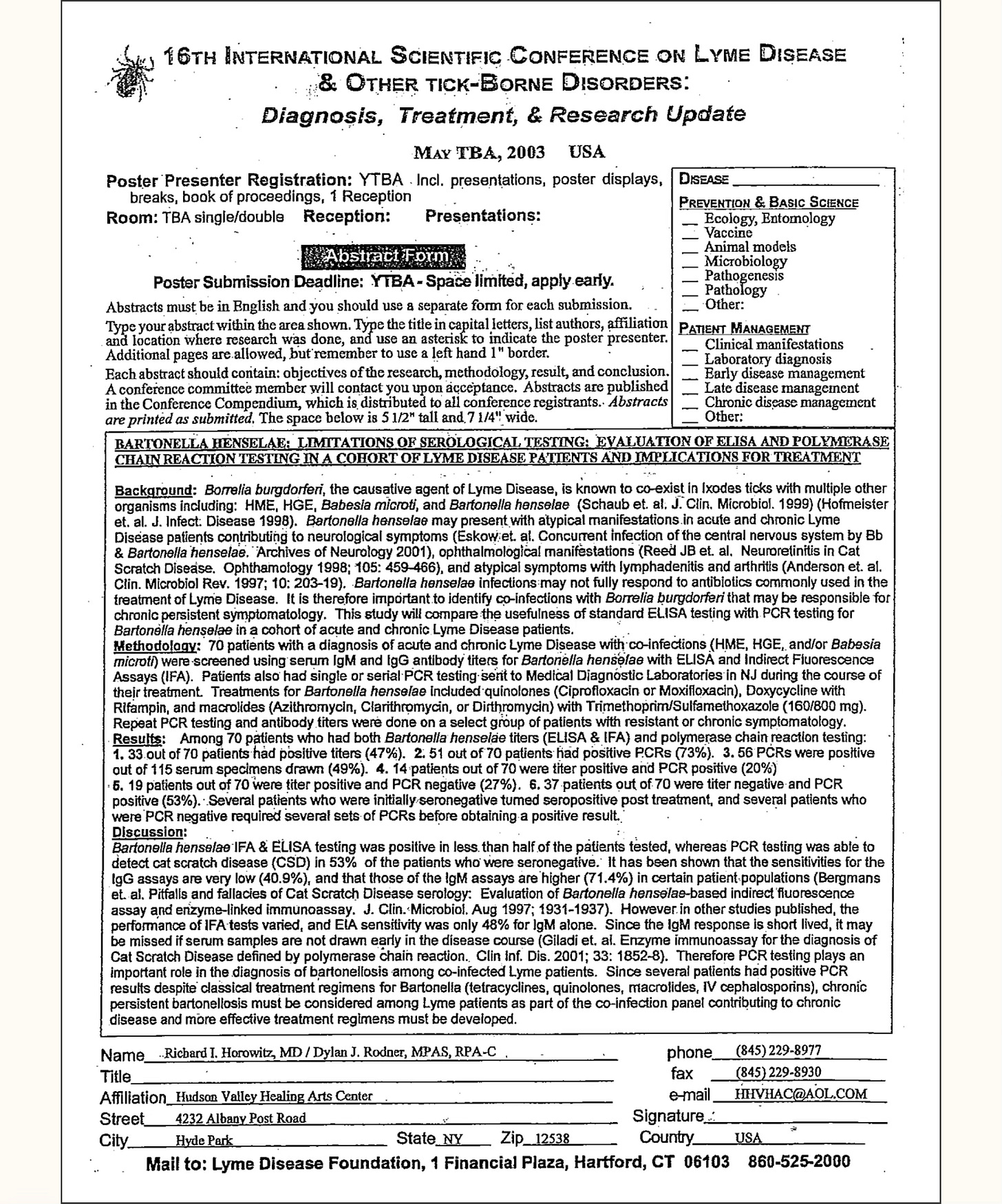
As you can see from the above table, testing for just one species makes no sense, because we can be exposed to a broad range of Bartonella species during our lifetime. I started to test for Bartonella over two decades ago. This is from an abstract I presented at the 16th International Scientific Conference on Lyme disease in 2003:
You can see from this abstract, even 22 years ago, by just testing for Bartonella henselae, one of the most common species, we found that using an ELISA and IFA (Immunofluorescent Assay) was positive in less than 50% of patients–but using DNA analysis with a PCR (Polymerase Chain Reaction) in the blood, we found 53% were positive when standard antibody assays were negative.
Which means the rule of thumb when testing for Bartonella is go as broad as you can. It is fine to start with local lab testing.
Level 1 testing
Using local labs like Quest, Labcorp, or Bioreference, you can send off antibody titers to B. henselae, B. quintana and B. bacilliformis, as well as PCRs and even a VEGF (vascular endothelial growth factor), an indirect marker of Bartonella exposure, indicating inflammation in the blood vessels (vasculitis). Often, however, you’ll want to use several specialty labs to prove infection.
Level 2 testing
If the above testing is negative, as it usually is, but you clinically suspect Bartonella, move on to the next level of tests. The three specialty labs include IgeneX laboratory (Bartonella IgM/IgG Immunoblots, Bartonella FISH [Fluorescent In-Situ-Hybridization test, an RNA test], T Labs (Bartonella FISH) with confocal microscopy, and Galaxy Laboratories, using their 4 species IFA antibody panel (for the most common species), and their ddPCR (direct droplet PCR) tests. The Bartonella Digital ePCR™ platform combines highly sensitive ddPCR technology with culture enrichment (BAPGM™).
I usually start with IgeneX laboratory and find that most of my patients have indeterminate or positive Immunoblots. Many times a negative Bartonella FISH test will turn positive later on during treatment, after the bacteria has been flushed out from the intracellular compartments where it’s been hiding.
I follow VEGF levels over time, as an indirect marker of Bartonella, when reactivation of infection is suspected. Keep in mind VEGF can be positive for other reasons (including Long Covid or cancer with metastases).
Level 3 testing
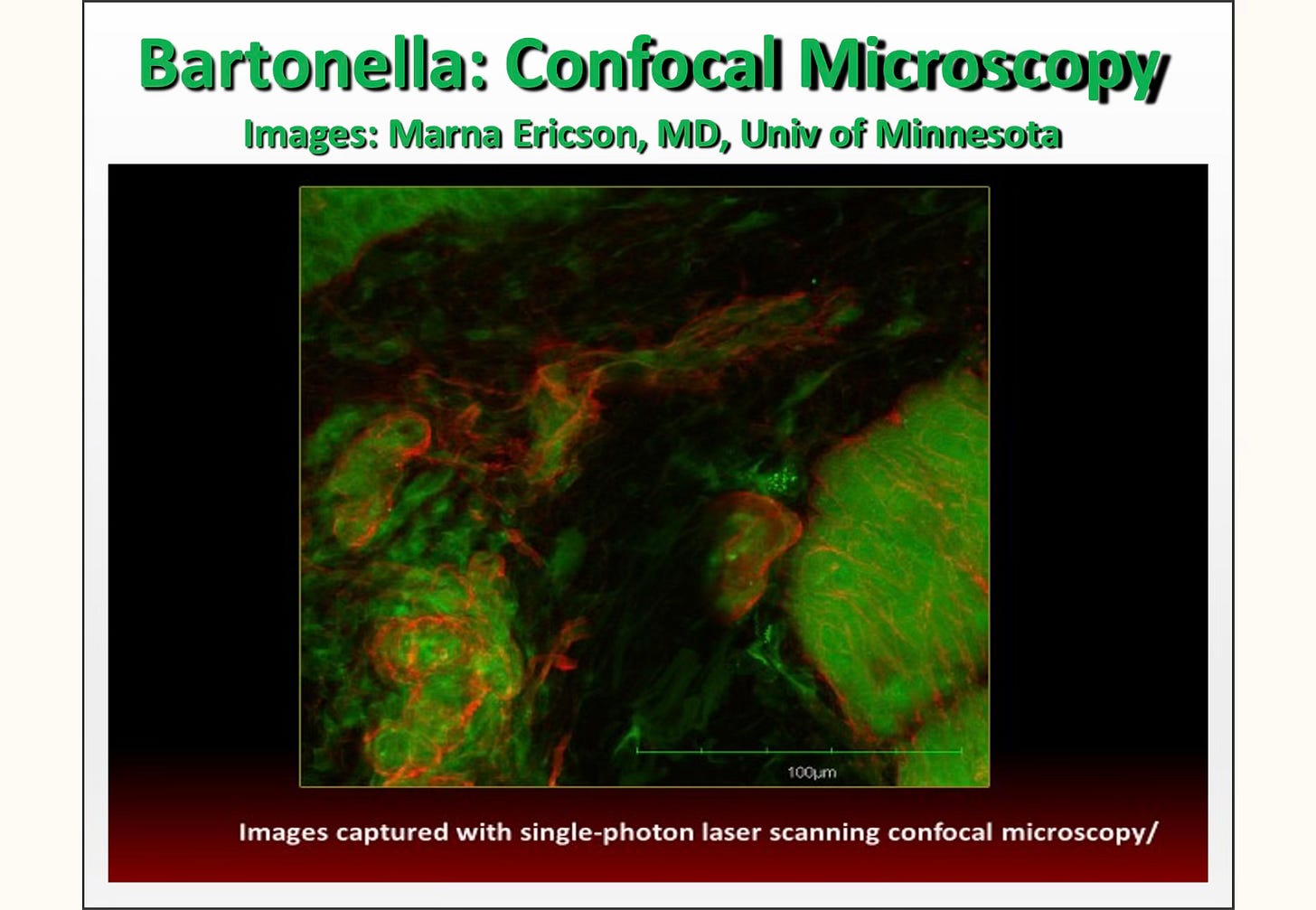
Skin biopsies can be done of the classical Bartonella rashes. Dr. Marna Ericson from T Labs has done this for me several times, and she found positive Bartonella in the skin, under biofilms, when it couldn’t be found through other methods.
I suspected Bartonella in two of my patients, but despite all classical testing, couldn’t prove exposure. The Bartonella fluoresces red under the microscope with this technique. I don’t suggest it as first level testing, but it can be very useful if you have looked for Bartonella using any and all of the above laboratories and methodologies.
Stay tuned for parts 2, 3, 4 and 5
In Part 2, I’ll discuss more about establishing a diagnosis as well as an overview of how other co-infections may overlap and affect Bartonella symptoms. Part 3 will discuss effective treatments, and Parts 4 and 5 go into more detail about these treatments.
Dr. Richard Horowitz has treated 13,000 Lyme and tick-borne disease patients over the last 40 years and is the best-selling author of How Can I Get Better? and Why Can’t I Get Better? You can subscribe to read more of his work on Substack or join his Lyme-based newsletter for regular insights, tips, and advice
I enjoyed answering your questions on Wednesday night.
We discussed:
Introduction and Webinar Format. Dr. Marty Ross explained the structure of his Lyme disease webinar, outlining guidelines for participation, including the use of the chat box for submitting questions, and detailed plans to provide session recordings and summaries.
Addressing Sleep Jerks and Neurological Symptoms. Severe sleep jerks occurring when falling asleep were attributed to neurological irritation caused by infections like Bartonella, Borrelia, or mold toxicity, and potential remedies including curcumin, glutathione, and GABA-boosting supplements were discussed.
Managing Nervous System Agitation. Strategies to calm the nervous system included treating infections, detoxifying mold, using anti-inflammatory supplements like curcumin and glutathione, and calming nerves directly via GABA enhancers such as L-theanine.
Ozone and IV Vitamin C may Cause Nerve Damage. The use of oxidizing agents like IV vitamin C and UV ozone can worsen oxidation injury in tick-borne infection patients, with Dr. Ross warning against their potential nerve-damaging effects.
Role of Hyperbaric Oxygen Therapy. While hyperbaric oxygen therapy (HBOT) may aid in neurological healing and support mitochondria, it is often ineffective for directly killing infections based on clinical experiences.
Exploring White Blood Cell Counts in Tick-Borne Infections. Chronic infections like Borrelia, Bartonella, or Babesia often cause reduced neutrophil counts, which may normalize over time with effective treatment.
Pregnancy Considerations and Tick-Borne Disease Testing. Pregnancy planning was addressed with recommendations for comprehensive infection testing, symptom-tracking, and considerations for treatment strategies that align with maternal and fetal health.
Re-testing for Infections to See Where Your Are Is Not Accurate. Retesting for tick-borne infections was deemed unreliable as antibodies can fluctuate; instead, tracking symptoms was suggested as a better measure of disease progression.
Indirect vs Direct Testing for Borrelia. Dr. Ross explained the differences in sensitivity between indirect (antibody-based) and direct (PCR or culture) testing methods, emphasizing the limitations of direct tests in chronic infections.
Babesia Treatment Length before Pregnancy. Recommendations for treating Babesia included maintaining a five-month treatment course, balanced with probiotics and potential yeast management, to optimize health before pregnancy.
Addressing Gastrointestinal Symptoms during Treatment. GI symptoms during antimicrobial treatment were linked to gut flora disturbance and potential yeast overgrowth, calling for probiotics and antifungal options like Nystatin or CapriPlus.
Management of Cytokines and Herx Reactions. Elevated cytokines causing inflammation and herx reactions were addressed with anti-inflammatory interventions, including quercetin or curcumin, and glutathione supplementation.
Best Ways to Lower Cytokines and to Control Herx. Suggestions to lessen herx reactions included increasing glutathione levels and using quercetin for both anti-inflammatory and mast cell-stabilizing effects.
Meaning of a Single White Brain Lesion on MRI. A single white lesion on MRI is typically attributed to aging or limited blood flow rather than Lyme disease, which usually exhibits diffuse demyelination patterns.
You Don’t Have to Herx to Make Progress. Not all patients experience herx reactions during treatment, yet progress is still possible, particularly as the germ load decreases over time.
Methylene Blue and Its Uses. Methylene blue was recognized as a therapy for both Borrelia and Bartonella due to its efficacy against persister cells, as well as for its FDA-approved use in addressing methemoglobinemia. Go here for a sound warning of methylene blue, which is a man-made monoamine oxidase inhibitor. Animal and human studies have shown that when monoamine neurotransmitters are over-activated it eventually makes those taking it subdued, apathetic and disengaged from their own feelings, those around them, and life itself.
Methylene Blue for Improved Thinking and Mitochondria Function. Beyond pathogen-killing properties, methylene blue improves mitochondrial function, aids ATP production, and has shown promise for reducing brain fog and increasing energy.
Potential Risks and Side Effects of Methylene Blue. Risks of methylene blue include bladder irritation, intestinal discomfort, and staining issues, though real-world human risks are minimal when dosed properly.
Mitochondrial Function and Repair. Recommendations for repairing mitochondrial damage included supplements like glutathione and ATP 360 to enhance cellular energy production.
Exploring Histamine Reactions. Unusual reactions like hives or hyperactive histamine levels during treatment were linked to mast cell activation, which can be managed with stabilizers and antihistamines.
Taking Enzymes and EDTA. Potential interactions between enzymes and EDTA supplements were addressed, with Dr. Ross advising additional research to confirm compatibility.
Impact of Biocidin on Direct Testing Results. Biocidin, containing antimicrobial ingredients like oregano oil and garlic, may reduce the accuracy of direct tests like PCR by lowering pathogen levels in the blood.
Causes of Visual Issues. Neuropathic visual challenges like light sensitivity and convergence insufficiency were discussed as possible symptoms of Bartonella, Borrelia, or mold toxicity.
Causes of Air Hunger. Air hunger, frequently caused by Babesia or Bartonella, results from disrupted oxygen delivery due to inflamed red blood cells or reduced red blood cell quantity.
Muscle Contractions and Spasms. Severe muscle spasms were linked to magnesium deficiency or neurological irritation, with treatment approaches including supplements and anti-inflammatory support.
Thoughts on Steps if You Are Not Getting Better. Persistent illness despite treatment prompted considerations for comprehensive reviews of treatment history and potential alternative strategies like addressing limbic system dysregulation.
Role of Limbic System Retraining for Chronic Symptoms. Limbic system retraining methods such as dynamic neural retraining (DNRS) were recommended for addressing chronic illness patterns after addressing active infections.
Senescent Cells may Cause Ongoing Inflammation and Chronic Symptoms. Cell senescence caused by infections may perpetuate inflammation, with solutions including senolytics, fasting mimicking diets, and autophagy-promoting supplements.
Timing of Limbic System Retraining and Physical Medicine. Brain retraining exercises and somatic therapies are best initiated after active infections are controlled to avoid exacerbating symptoms.
Evaluating ZenMen for Bartonella. The herbal formula ZenMen showed promise in addressing Bartonella but lacked sufficient evidence on effectiveness or ingredient concentrations for strong recommendations.
Role of Ketotifen for Mast Cell Activation. Ketotifen was highlighted as an effective option for calming histamine-driven nervous system agitation by blocking histamines and stabilizing mast cells
Sign Up for the January Lyme Q&A Series Through LymeUNITED
We’ve Moved. Conversations with Marty Ross MD is located inside the LymeUNITED membership support community. LymeUNITED is now FREE. But you will need to join LymeUNITED and then RSVP to participate in the Wednesday webinar.
Step 1. Join LymeUNITED for Free
Step 2. Click “Dr. Ross Q&A Webinar” in the left column navigation menu
Step 3. Click on the title of the event you want to attend to RSVP and to learn all about Conversations with Marty Ross MD using the live Zoom Room through LymeUNITED.
You have two options to watch Conversations with Marty Ross, MD Recordings.
With Recording Headings and Time Stamp. In LymeUNITED you can watch the recording which includes time stamps and headings to find what you are looking for more easily. Once you are in LymeUNITED go to the “Zoom Event Recordings” located in the left hand navigation menu. Watch on LymeUNITED.(Note:if you are not a member, you will need to join first to watch from the video link above. Join LymeUNITED Now.)
No Headings or Time Stamps. Watch on YouTube. This version does not require you sign up for a Free LymeUNITED membership. But, it does not include time stamps or section headings. Watch on YouTube.
Get Help and Support
If you have questions, there are three ways that we can help you.
Join LymeUNITED: A Community Powering Health for FREE. This is our online support community hosted by Marty Ross, MD with an active group of supporting members. You don’t have to do it alone.
I’ve never heard of ozone and IV C causing nerve damage. Ever. My LLMD uses this as a mainstay in treatment and would never use them if they in fact caused nerve damage. Of course the toxin is always in the dose.
The current medical system is failing those suffering from Long COVID and vaccine injuries—patients are gaslit, dismissed, and left to deteriorate without real solutions. The reason? Our healthcare model is built around randomized controlled trials (RCTs), which were never designed for individualized treatment.
What Is an N-of-1 Trial?
An N-of-1 trial is a personalized, single-patient clinical study that aligns treatment based on the individual’s unique biomolecular response. Instead of relying on population-based statistics, this method uses real-time molecular surveillance, patient-specific peptide therapeutics, and adaptive treatment adjustments to achieve true precision medicine.
Unlike traditional one-size-fits-all drug development, N-of-1 trials are built around the patient—tracking their unique exome, transcriptome, and proteome to correct faulty molecular signaling at the source.
We do not have time to wait for mass-scale trials designed for bureaucratic approval pipelines rather than real-world recovery. Lives are deteriorating daily, careers are lost, and families are crumbling. The answer is clear: we need a personalized, adaptive medical model that responds to the patient in real-time—not a slow-moving, industry-driven system.
A Stark Illustration:
Recent breakthroughs in gene-based therapies have demonstrated impressive success in conditions like spinal muscular atrophy, sparking renewed hope for addressing complex neurogenetic diseases. However, many of these interventions are designed to target specific genetic variations, and the rigid structure of traditional clinical trials has created a severe bottleneck in innovation.
Economic and bureaucratic barriers ensure that commercial development is prioritized only for high-prevalence druggable genetic variants— those deemed profitable and feasible for large-scale trials. As a result, countless patients with rare or individualized molecular disruptions are left without viable treatment options, reinforcing the urgent need for N-of-1 trials that bypass these restrictive models and deliver precision-driven solutions in real-time.
Unfortunately, this progress has not extended to Long COVID and vaccine-related injuries, where patients are suffering from Spike-protein-induced immune dysregulation, severe cardiac damage, neuroinflammation, and persistent spike-related organ damage with no viable path to treatment.
The reason is clear: traditional clinical trial models prioritize druggable conditions with large, commercially profitable patient populations while existing N-of-1 trials are still shackled by the same flawed system, failing to deliver the personalized, compassionate care that patients with complex, individualized needs urgently require. The solution is simple: individualized N-of-1 trials must operate independently, untainted by the dysfunction of the current medical research model.
The Catastrophic Failure of RCTs in Chronic Disease
RCTs were designed for standardized drug testing, not complex, multi-systemic conditions like Long COVID and vaccine injuries. These illnesses vary drastically between individuals, yet the medical system continues to force them into rigid study parameters that discard individualized responses.
Why the System Is Broken:
• Deliberate Exclusion of the Suffering – Long COVID and vaccine-injured patients don’t fit neatly into RCT parameters, so they are ignored.
• Slow, Bureaucratic Approval Processes – Years-long trials mean patients deteriorate while waiting for an answer.
• Generalized Data Over Personalized Care – RCTs focus on “majority response,” discarding those who don’t fit the mold.
This isn’t science—it’s systemic neglect.
A System Rigged Against Individualized Care
We don’t see this approach in mainstream medicine because it threatens the financial strength of the pharmaceutical industry.
• Precision-targeted treatments mean fewer mass-produced drugs—which cuts into Big Pharma’s profit margins.
• A truly individualized medical system means fewer hospitalizations, fewer unnecessary interventions, and fewer chronic patients dependent on expensive lifelong medications.
• RCT-based gatekeeping ensures only patented, billion-dollar drugs get approval—while peptide and precision small molecule therapeutics remain buried under regulatory red tape.
This system is not designed to heal people—it is designed to sustain an industry. We Can’t Afford to Wait—Patients Are Deteriorating Now (See link for article)
John Drake is a professor at the University of Georgia
Blacklegged tick (Ixodes pacificus) on a leaf, carrier of the Lyme disease, 2005. Image courtesy … [+]
Getty Images
Tens of thousands of Lyme disease cases are reported in the United States each year, according to the Centers for Disease Control and Prevention. However, the actual number of infections is likely several times higher. In fact, Lyme disease is now the most common vector-borne illness in the country. But nobody actually knows how common it is.
Recent studies by the CDC are beginning to shed light on why that is.
I asked Dr. Alison Hinckley, a CDC epidemiologist, what the significance of these studies is for the ordinary person.
“The bottom line,” she said, “is there are different data sources used to answer questions about Lyme disease epidemiology and trends. Taken together, the data demonstrate that Lyme disease is a significant and growing public health threat. The numbers indicate a large burden on the health care system, a threat to public health, and the need for more effective prevention measures.”
Lyme disease is a tick-borne illness primarily transmitted by black-legged ticks of the Ixodes genus. First identified in 1975 in Lyme, Connecticut, it has since spread geographically across the United States. People contract Lyme disease after being bitten by a tick infected with the bacterium Borrelia burgdorferi. Early symptoms often include fever, chills, a characteristic rash known as erythema migrans and muscle or joint pain. If left untreated, Lyme disease can lead to more severe complications, such as facial paralysis, heart rhythm disturbances, arthritis and inflammation of the brain and spinal cord.
Understanding the gap between reported cases and the true disease burden requires distinguishing between surveillance data and the broader scope of undiagnosed or unreported cases. (See link for article)
_____________
**Comment**
Thankfully the article mentions that surveillance is a problem due to the fact there must be laboratory evidence of infection as well as clinical information to confirm diagnosis. How can a test that misses up to 90% of cases be seriously used to determine cases of infection?
Rather than pulling out all the stops to fix this long held problem, the CDC would rather estimate that cases are three to 12 times higher than the number reported through surveillance.