A very real U.S. Government laboratory shrouded in secrecy that existed at Plum Island (which has been moved to Kansas state University) was inspired by a Nazi bioweapons expert, and housed Fort Terry a biological warfare defense research facility. The lab had a mission to poison cattle in the Soviet Union during the Cold War and was also connected to an African Swine Fever outbreak in Cuba. It should come as no surprise that strange genetically mutated creatures have washed up on the shores of the mainland.
Tick experimentation by the government has been going on since at least the 60’s due to their ability to spread disease, with certain pathogens never showing up on testing. The “discoverer” of Lyme disease – Willy Burgdorfer, just happened to work at the NIH state of the art BSL- 4 biomedical research facility called the Rocky Mountain Lab (RML) in Montana force-feeding ticks various pathogens. There is also a record of dropping infected ticks from airplanes to study their distribution patterns.
It doesn’t take a rock-scientist to realize the implications of these actions.
https://rumble.com/v43vmkx-under-our-skin-part-1-and-2-both-lyme-disease-movies-in-one-video-is-lyme-d.html
Under Our Skin 1 & 2: Is Lyme Disease A Bioweapon?
https://amzn.to/48znBOJ
In the early 1970’s, a mysterious ailment was discovered among children living around the town of Lyme, CT. What was first diagnosed as isolated cases of juvenile arthritis, eventually became known as Lyme disease, an illness triggered by spiral-shaped bacteria, similar to the microorganisms that cause syphilis. Today, many of those untreated will suffer chronic debilitating illness. Some unknowingly will pass the disease onto their unborn children. Many will lose their livelihoods, and still others, their lives.
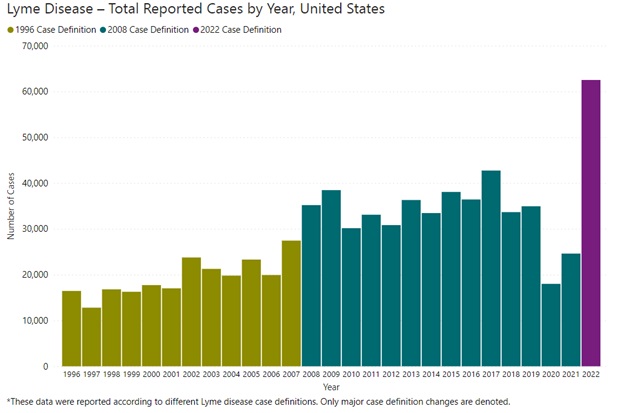
Yet Lyme disease is one of the most misunderstood and controversial illnesses of our time. Difficult to test accurately, tens of thousands of people go undiagnosed — or misdiagnosed with such conditions as fibromyalgia, chronic fatigue, autism, MS and ALS. The Centers for Disease Control estimates more than 300,000 people acquire Lyme disease each year, a number greater than breast cancers and AIDS combined. And yet, the medical establishment — with profound influence from the insurance industry — has stated that the disease is easily detectable and treatable, and that “chronic Lyme” is some other unrecognized syndrome or a completely psychosomatic disorder.
UNDER OUR SKIN is a powerful and often terrifying look not only at the science and politics of the disease, but also the personal stories of those whose lives have been affected and nearly destroyed. From a few brave doctors who risk their medical licenses, to patients who once led active lives but now can barely walk, the film uncovers a hidden world that will astound viewers. While exposing a broken health care and medical research system, the film also gives voice to those who believe that instead of a crisis, Lyme is simply a “disease du jour,” over diagnosed and contributing to another crisis: the looming resistance of microbes and ineffectuality of antibiotics. As suspenseful and hair-raising as any Hollywood thriller, UNDER OUR SKIN is sure to get under yours.
……..
https://amzn.to/48znBOJ
In this dramatic follow-up to the widely acclaimed UNDER OUR SKIN, EMERGENCE takes the viewer on a journey from horror to hope. We witness the emerging epidemic of Lyme disease as infection and education spread globally. We watch as the truth emerges about the disease’s persistence and reach, about promising new research, and about medical collusion and conflicts of interest that continue to impede progress. We revisit the characters from UNDER OUR SKIN as they emerge into better health, reclaiming their lives and dignity, and offering hope to the legions now suffering. As Lyme disease surges, EMERGENCE shines a probing light on the issue and becomes a beacon in the dark.
By Kris Newby
https://amzn.to/3NKAUUq
Amazon Description:
A riveting thriller reminiscent of The Hot Zone, this true story dives into the mystery surrounding one of the most controversial and misdiagnosed conditions of our time — Lyme disease — and of Willy Burgdorfer, the man who discovered the microbe behind it, revealing his secret role in developing bug-borne biological weapons, and raising terrifying questions about the genesis of the epidemic of tick-borne diseases affecting millions of Americans today.
While on vacation on Martha’s Vineyard, Kris Newby was bitten by an unseen tick. That one bite changed her life forever, pulling her into the abyss of a devastating illness that took ten doctors to diagnose and years to recover: Newby had become one of the 300,000 Americans who are afflicted with Lyme disease each year.
As a science writer, she was driven to understand why this disease is so misunderstood, and its patients so mistreated. This quest led her to Willy Burgdorfer, the Lyme microbe’s discoverer, who revealed that he had developed bug-borne bioweapons during the Cold War, and believed that the Lyme epidemic was started by a military experiment gone wrong.
In a superb, meticulous work of narrative journalism, Bitten takes readers on a journey to investigate these claims, from biological weapons facilities to interviews with biosecurity experts and microbiologists doing cutting-edge research, all the while uncovering darker truths about Willy. It also leads her to uncomfortable questions about why Lyme can be so difficult to both diagnose and treat, and why the government is so reluctant to classify chronic Lyme as a disease.
A gripping, infectious page-turner, Bitten will shed a terrifying new light on an epidemic that is exacting an incalculable toll on us, upending much of what we believe we know about it.
…….
December 27, 2023
I just finished @krisnewby’s Bitten, which tells the history of the US government’s secret program in the 1950s and 1960s to weaponize ticks to deliver deadly bacteria to incapacitate unsuspecting populations.
Newby, a talented journalist and science writer, structures her history around a biography of Willy Burgdorfer, the Swiss-American scientist who discovered borellia burgdorferi, a spirochete bacteria often found in Lyme disease patients.
It’s an incredible, infuriating, well-written book worth your time.
A few lessons:
1. The mid-20th century US biomedical research establishment was psychopathic, whole-heartedly embracing reckless, deadly investigations in the name of developing vaccines and bioweapons.
2. It is possible (& perhaps likely, though not proven) that the emergence and spread of Lyme disease may have been caused by this research program, which included large open-air testing of intentionally infected ticks on US soil.
3. The bioweapons program used combinations of viruses and bacteria infecting the same tick to hide the body’s immune response to infection from detection by standard medical tests.
4. Lyme disease and related syndromes are likely caused by more than just borellia burgorferi. Newby makes a circumstantial case for a shadowy rickettsia bacteria that Willy Burgdorfer studied, which he called the “Swiss agent.”
5. The financial interests of biomedical researchers and testing companies peddling faulty tests — alongside their control over the official pronouncements and policy of the National Institute of Health and the US Infectious Disease Society of America — have frozen in place a diagnostic doctrine that has led to countless Lyme disease patients misdiagnosed and gaslit about the symptoms they are suffering.
Closing thought: similar tendencies in the biomedical research and medical establishments are still extant and may help explain many things about the covid pandemic. History does not repeat, but it rhymes.
Source: https://twitter.com/DrJBhattacharya/status/1740029782967148624
_______________
**Comment**
Please read these articles to get a bird’s-eye view of the topic: