Tick-borne agents of disease continue to emerge and subsequently expand their geographic distribution. The threat to blood safety by tick-borne agents is ever increasing and requires constant surveillance concomitant with implementation of appropriate intervention methods. In April 2017, the Food and Drug Administration organized a public workshop on emerging tick-borne pathogens (excluding Babesia microti and Lyme disease) designed to provide updates on the current understanding of emerging tick-borne diseases, thereby allowing for extended discussions to determine if decisions regarding mitigation strategies need to be made proactively. Subject matter experts and other stakeholders participated in this workshop to discuss issues of biology, epidemiology, and clinical burden of tick-borne agents, risk of transfusion-transmission, surveillance, and considerations for decision making in implementing safety interventions. Herein, we summarize the scientific presentations, panel discussions, and considerations going forward.
Interestingly, according to the abstract, they excluded Babesia and Lyme, which are arguably two of the largest problems. It was pointed out that 200 cases of Babesia were transmitted through blood transfusions at the time of the workshop and that Anaplasma is next with increasing clinical cases.
Evidently there have been no reported cases of Lyme transmitted through the blood supply.
Other tick-borne pathogens have been transmitted through donated blood, but these occurrences are rare. (Or rarely reported)
11 cases: A. phagocytophilum, responsible for Anaplasmosis (transmitted by the Ixodes ticks)
2 cases: Tick-borne encephalitis virus complex (TBEV, Powassan virus, DTV), (transmitted by the Ixodes ticks)
1 case: Rickettsia rickettsii, the agent of Rocky Mountain Spotted Fever (transmitted by the Lone Star tick)
1 case:Ehrlichia ewingii(transmitted by the Lone Star tick)
In addition, “two emerging [tick-borne agents] − B. miyamotoi and Powassan virus were discussed − for B. miyamotoi,cases have steadily increased since 2014.”
The Ability of the Invasive Asian Longhorned Tick Haemaphysalis Longicornis (Acari: Ixodidae) to Acquire and Transmit Rickettsia Rickettsii (Rickettsiales: Rickettsiaceae), the Agent of Rocky Mountain Spotted Fever, Under Laboratory Conditions
The invasive Asian longhorned tick, Haemaphysalis longicornis Neumann, was first detected in the United States in 2017. It has since been found in 12 states, and there is concern that the tick’s parthenogenetic ability and wide variety of host species may allow for broader dissemination. Of the tick-borne diseases endemic to the United States, Rocky Mountain spotted fever (RMSF), a rapidly progressive and potentially fatal disease caused by Rickettsia rickettsii, is the most severe. There is considerable geographical overlap between spotted fever rickettsioses cases, which include RMSF, and the currently known distribution of H. longicornis, providing the potential for this tick to encounter this pathogen.
We have evaluated the ability of H. longicornis to acquire and transmit R. rickettsii under laboratory conditions. Haemaphysalis longicornis as larvae and nymphs acquired the pathogen while feeding on infected guinea pigs. The infection persisted through every life stage, all of which were able to transmit R. rickettsii to naïve hosts. The pathogen was also transmitted at a low frequency between generations of H. longicornis through the ova. While H. longicornis was demonstrated to be a competent vector for R. rickettsii under laboratory conditions, the probability of its involvement in the maintenance and transmission of this pathogen in nature, as well as its potential impact on human health, requires further study.
___________________
**Comment**
The Asian Long-horned tick used to be known as pretty much just a livestock pest. Obviously, researchers are changing their tune. What makes this tick particularly unique and equally terrifying is its ability to reproduce through cloning – making a literal infestation very quickly. It is traipsing through the entire U.S. – having been found in at least 12 states.
The pressing question is what all do they transmit? We know this so far:
It spreads SFTS (sever fever with thrombocytopenia syndrome), “an emerging hemorrhagic fever,” causing fever, fatigue, headache, nausea, muscle pain, diarrhea, vomiting, abdominal pain, disease of the lymph nodes, and conjunctival congestion, but the potential impact of this tick on tickborne illness is not yet known. In other parts of the world, this Longhorned tick, also called the East Asian or bush tick, has been associated with several tickborne diseases, such as spotted fever rickettsioses, Anaplasma, Ehrlichia, and Borrelia, the causative agent of Lyme Disease. https://madisonarealymesupportgroup.com/2018/06/12/first-longhorned-tick-confirmed-in-arkansas/
For a 2016 literature review on SFTS:http://infectious-diseases-and-treatment.imedpub.com/research-advances-on-epidemiology-of-severefever-with-thrombocytopenia-syndrome-asystematic-review-of-the-literature.php?aid=17986 Although the clinical symptoms of SFTS and HGA are similar to each other, but the treatment methods of the two diseases are totally different. Doctors notice that the biggest difference between the clinical symptom of SFTS and HGA is that SFTS patients generally without skin rash, the dermorrhagia is also not seriously, and few massive hemorrhage cases were reported [23]. It is also reported that SFTS patients had gastrointestinal symptoms, such as nausea, vomiting, and diarrhea, which are rarely observed in HGA patients [2]. So these differences can be used as the auxiliary basis of differential diagnosis. At present, there is still no specific vaccine or antiviral therapy for SFTSV infection. Supportive treatment, including plasma, platelet, granulocyte colony stimulating factor (GCSF), recombinant human interleukin 11, and gamma globulin is the most essential part of case treatment [44]. Meanwhile, some measures were taken to maintain water, electrolyte balance and treat complications are also very important. Ribavirin is reported to be effective for treating Crimean-Congo Hemorrhagic Fever (CCHF) infections and hemorrhagic fever with renal syndrome, but it is still inadequate to judge the effect of ribavirin on SFTS patients because of the study limitation without adequate parameters were investigated [45]. Host immune responses play an important role in determining the severity and clinical outcome in patients with infection by SFTSV. For Viral treatment options: https://madisonarealymesupportgroup.com/2016/03/28/combating-viruses/
And lastly, please know ticks parasitize one another, potentially spreading all manner of diseases to humans. This fact also shoots holes in the regurgitated mantra that only certain ticks carry certain pathogens. If they are feasting on one another, they can potentially infect each other and then us: https://madisonarealymesupportgroup.com/2018/03/07/tick-bites-tick-hyperparasitism/
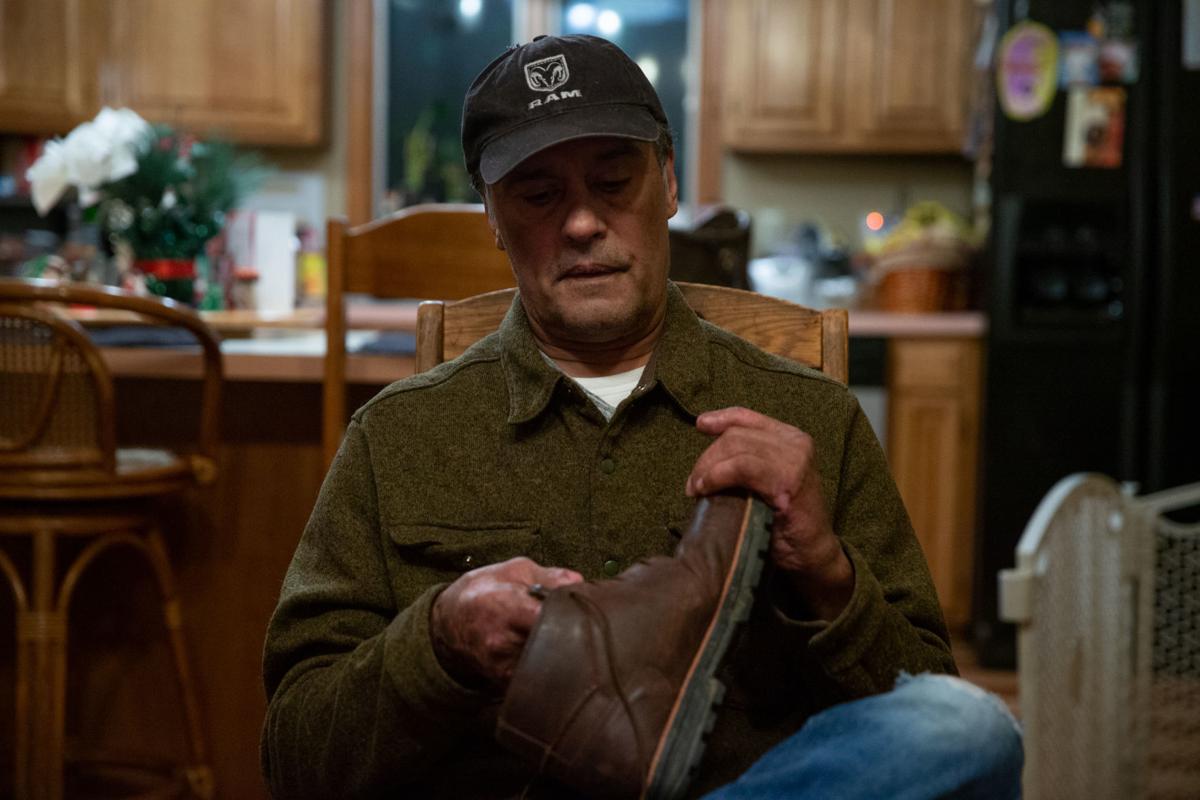
Beltran has one pair of shoes that accommodate his custom-made orthopedic spacers, which give him even footing after all his toes and a 2 1/2-inch portion of his left foot were amputated.
Photos by Mike Morones / The Free Lance–Star
Quintin Beltran enters the room at a good clip, proudly showing off how well he’s walking.
He holds onto a cane for support because he’s still not used to this new version of himself. The 60-year-old lost all the toes on both feet, and another 2 1/2 inches of flesh and bone from his left foot, after an insect no bigger than a pinhead changed every aspect of his life.
Beltran contracted Rocky Mountain Spotted Fever after a bite from a common American dog tick in April. The devastation caused by the deadly disease and the side effects of powerful drugs—given when his organs started shutting down and death loomed—resulted in a loss of blood to his extremities…. (See link for article)
Rickettsial diseases or rickettsioses are infections caused by various bacteria belonging to the genus Rickettsia. These bacteria are transmitted through the bites of certain hard-bodied ticks and some other arthropods. Rickettsial diseases are not to be confused with rickets, which is a condition affecting the bones and resulting from vitamin D deficiency.
The infections caused by Rickettsia bacteria have traditionally been classified into two groups: spotted fever and typhus. However, they’re sometimes divided into further categories. Either way, all groups include species of pathogens that can infect humans. Although Rickettsia bacteria can be found worldwide, the most common rickettsial illnesses are normally contracted in Africa and Asia.
Lyme disease is also transmitted to humans by ticks. It’s the most common tick-borne illness in the northern hemisphere. However, Lyme isn’t a rickettsial disease, since it’s caused by a bacterium of a different genus: Borrelia burgdorferi.
However, the same tick that carries Rickettsia bacteria might also be infected with Borrelia burgdorferi. Therefore, it’s possible to contract both illnesses via one tick bite. Therefore, the answer to question ‘is Rickettsia a Lyme co-infection?’ is that yes – rickettsiosis can be a potential co-infection of Lyme disease.
What Are The Symptoms of Rickettsia Diseases?
Some of the most common rickettsial diseases are Rocky Mountain spotted fever, anaplasmosis, ehrlichiosis and typhus. All of these are generally difficult to diagnose. Some of them rarely cause symptoms, and most of them only cause moderate illness even when symptomatic. However, certain forms of spotted fever and typhus may be fatal if left unrecognised and untreated. The sooner these illnesses are diagnosed, the easier they are to treat using antibiotics.
The clinical presentation of rickettsial diseases varies greatly. Even infections caused by the same species of bacteria may produce different symptoms in different patients. Nonetheless, the most common symptoms include
fever
headache
fatigue
malaise
nausea
vomiting
rashes and eschar (a piece of dry and dark dead skin at the site of the bite). These tend to develop within two weeks after the bacteria have entered the body.
African tick bite fever is one of the mildest forms of rickettsiosis. Patients usually present with fever, headache, muscle pain and an eschar shortly after contracting the disease during a visit to southern Africa.
Fever is a common symptom of all rickettsial diseases.
Mediterranean spotted fever is a serious and potentially life-threatening illness. It’s prevalent in the Mediterranean region, including northern Africa. In addition to fever, rashes and an eschar are typical signs of the illness.
Patients with Rocky Mountain spotted fever often experience fever, headache, nausea, and stomach pain. A rash at the site of the bite is also commonly seen, but eschars aren’t usually present.
The only common symptom of murine or endemic typhus is fever. About half of all patients also develop a rash. Scrub typhus can be contracted in Asia, and it’s characterised by a severe fever, headache and muscle pain. An eschar, cough, enlarged lymph nodes and encephalitis (inflammation of the brain) may also occur in some patients.
The symptoms of ehrlichiosis and anaplasmosis are similar to those of other rickettsial diseases. However, they’re also known to significantly reduce white blood cell count in affected people.
Is Rickettsia The Same As Lyme Disease?
Rickettsiosis and Lyme disease share several symptoms in their early stages, such as fever, headache, fatigue, malaise and muscle pain. Moreover, all of these symptoms also overlap with those of the flu and other non-specific viral infections, making diagnosis even more challenging.
The only distinctive sign of Lyme disease is the circular bull’s eye rash that develops around the tick bite within a few weeks. However, the rash can also appear elsewhere on the body, and in 20-30% of patients it’s not seen at all.
The diagnosis of Lyme and rickettsial diseases is usually based on a combination of factors, including signs, symptoms, patient history and laboratory tests. Unfortunately, currently there aren’t any completely reliable diagnostic tests available for Lyme disease: in the first weeks after infection, there’s a 60% rate of false negative results. Serological assays for rickettsiosis are more reliable, but these can take 10–12 days to provide a decisive result.
Tests such as serological assays are required to identify rickettsiosis.
What To Do If You Think You’ve Been Infected With Rickettsia
Ticks are very tiny, and their bites aren’t painful. Many people don’t even realise they’ve been bitten.
It’s important to note that being bitten by a tick doesn’t mean you’ve contracted an illness. In fact, out of the approximately 800 different tick species in the world, less than 60 can transmit infections to humans and animals. Most types of tick also have to be attached to the host’s body for an extended period of time in order to pass on any bacteria.
Nevertheless, you must see your doctor if you have a fever and any other flu-like symptoms or a rash shortly after being bitten by a tick. You should also arrange a medical appointment if you don’t recall being bitten but you do experience some suspicious symptoms within a few weeks of returning from a high-risk area. Be sure to tell your doctor about your recent travels, so that they can evaluate the probability of a tick-borne infection and order any appropriate diagnostic tests.
_______________
**Comment**
According to information written in Carl Tuttle’s petition against the IDSA, he mentions an article that indicates the persistent form of Lyme disease might be caused by another organism altogether.
“The STAT article reports that both Jorge Benach and Allen Steere now say it is time to take a closer look at Rickettsia helvetica’s role in Lyme disease. Benach says the research “should be done” because public health concerns warrant a closer look.”
“Dr. Willy Burgdorfer reviewed and tested patient blood samples from Dr. Anderson for C9P09, which is a rickettsial helical Mycoplasma; P09 being a Rickettsia bellii and C9 being a Mycoplasma (FIG. 2).35 This is further supported by the theory that an endosymbiotic infection produces spirochetes that are uncultivable Mycoplasmas, which are also called spirochetes. 1, 22, 31, 32
The “Swiss Agent” is documented by Dr. Willy Burgdorfer (FIG. 3),25 who also wrote a speech on “Pandora’s Box”.5 Although the Swiss Agent paper is associated with the suspected African Swine Flu, Dr. Willy Burgdorfer appears to be famous for leaving clues throughout his work regarding Lyme disease. Upon reviewing the structure of the Lyme disease “Swiss Agent” and the “Pandora Giant Virus”, there is a striking resemblance that deserves further examination.”
I don’t think we actually know precisely what the agent(s) causing Lyme disease is. This would explain why it can’t be picked up in current testing and why many fail treatment.
While it’s true that the early stages can often yield unspecific symptoms, an experienced eye will be able to diagnose a patient with tick borne illness. Also, please remember that in some patients their only symptoms are psychological: https://madisonarealymesupportgroup.com/2015/10/18/psychiatric-lymemsids/Any acute onset behavior changes should be suspect. Please don’t mess around with mainstream medicine should this occur. Get to an experienced and recommended ILADS practitioner who understands the mental illness aspect of tick borne disease.
The article’s statement that 20-30% of patients don’t get the rash must be taken from the inaccurate CDC count which is always abysmally low. No one I work with gets the rash. No one!
Please read this well written article on why we need to stop treating tick-borne illness like a typical infectious disease:
Seventeen (6.8%) samples were seropositive for antibodies against at least one pathogen: five for A. phagocytophilum, eight for B. burgdorferi, and four for Rickettsia spp.