Lyme disease in an African American child with Down’s syndrome
Welcome to another Inside Lyme Podcast with your host Dr. Daniel Cameron. In this episode, Dr. Cameron discusses the case of a 3-year-old African American child with Down’s syndrome, developmental delays and disseminated Lyme disease.
“A case of disseminated Lyme disease in a child with skin of color” was published by Bax and colleagues in the journal Pediatric Dermatology.¹ The child, who had trisomy 21 (Down’s syndrome) and developmental delays, had a history of playing outside in an area where ticks were observed.
According to the authors, the young girl had experienced a high fever for 9 days and had a 5-day history of rashes. The rashes were asymptomatic and would wax and wane. They consisted of “scattered ill-defined 2-5 cm erythematous patches on the back, abdomen, and upper and lower extremities,” a pattern consistent with disseminated Lyme disease.
There were other manifestations of Lyme disease, as well. “While the patient could not verbalize pain, her mother noted that she was walking less and was not tolerating her leg braces or shoes,” wrote the authors. “She also appeared increasingly fatigued and agitated.”
The doctors ruled out COVID-19, inflammatory syndrome (MIS-C), and Incomplete Kawasaki’s syndrome. “Incomplete Kawasaki’s syndrome was also considered given her hand/foot erythema, skin lesions, fingertip desquamation, and elevated CRP.”
Laboratory tests supported the diagnosis of Lyme disease. The child showed “significant improvement” with 14 days of amoxicillin.
“African Americans in Borrelia burgdorferi-endemic regions have been reported to have higher rates of extracutaneous sequelae, such as arthritis, and lower rates of erythema migrans compared with Caucasians, suggesting that the characteristic rash in skin of color may go unrecognized until more severe symptoms manifest,” the authors wrote.
They did not address the challenges in diagnosing Lyme disease in people with Down’s syndrome and development delays. Fortunately, the 3-year-old toddler presented with a disseminate Lyme disease rash, symptoms, and functional problems, which led to an accurate diagnosis. This would have undoubtedly been more difficult without these findings.
Treatment
The authors did not discuss long-term outcomes or treatment concerns. In some cases, Lyme disease patients may have a co-infection which would require different types of treatment. For instance, amoxicillin would not be effective in treating Anaplasmosis and Babesia.
The following questions are addressed in this Podcast episode:
Have you treated children with Down’s syndrome and developmental delays for Lyme disease?
What were the diagnostic and treatment challenges in working with this child?
Have you also treated children and adults of color? If so, what diagnostic and treatment challenges do they pose?
Tell me about your experience with Lyme disease in children on the autism spectrum.
Thanks for listening to another Inside Lyme Podcast. Please remember that the advice given is general and not intended as specific advice to any particular patient. If you require specific advice, please seek that advice from an experienced professional.
Inside Lyme Podcast Series
This Inside Lyme case series will be discussed on my Facebook page and made available on podcast and YouTube. As always, it is your likes, comments, and shares that help spread the word about this series and our work. If you can, please leave a review on iTunes or wherever else you get your podcasts.
References:
Bax CE, Clark AK, Oboite M, Treat JR. A case of disseminated Lyme disease in a child with skin of color. Pediatr Dermatol. Sep 13 2021;doi:10.1111/pde.14770
Fix AD, Pena CA, Strickland GT. Racial differences in reported Lyme disease incidence. Am J Epidemiol. Oct 15 2000;152(8):756-9. doi:10.1093/aje/152.8.756
Potential barriers to accepting a Lyme disease vaccine
Welcome to another Inside Lyme Podcast with your host Dr. Daniel Cameron. In this episode, Dr. Cameron discusses the potential barriers to the public’s acceptance and utilization of a Lyme disease vaccine.
It has been two decades since the LYMErix vaccine for Lyme disease was withdrawn from the market by the manufacturer, GlaxoSmithKline Pharmaceuticals after poor sales.
Why is it taking so long for another vaccine to become available? Several factors have been mentioned including: complex recommendations for the use of the vaccine; the lack of approval for the use of the vaccine in children, the group at highest risk; unvalidated claims of the vaccine causing Lyme arthritis and the coincident rise of general anti-vaccination sentiment among the public.”
CLICK HERE TO WATCH A VIDEO DISCUSSING POTENTIAL BARRIERS TO A LYME DISEASE VACCINE
The authors conducted 9 online focus groups which included consumers and 30 in-depth interviews among clinician groups.
The LYMErix vaccine was effective at preventing a rash but only 50% effective at preventing chronic manifestations of Lyme disease.
“Individuals who strongly disagreed with the importance of vaccines in general were excluded from the study to minimize skewed opinions that may not reflect the opinions of the general population,” the authors wrote.
They point out that their findings may not be generalizable. Nevertheless, the participants in the survey raised several potential barriers to accepting a Lyme disease vaccine.
Several of the clinicians’ concerns included:
“A quarter of the clinicians argued that a Lyme disease vaccine would be less important than other routine vaccines because Lyme disease can be prevented through other measures, cannot be transmitted person-to-person, is not widespread throughout the United States and has a lower disease burden than other vaccine-preventable diseases.”
“The most commonly presumed barriers to vaccine uptake were patient concerns about cost and safety and anti-vaccine sentiment.”
“Five clinicians expressed concern that a vaccine might promote a false sense of security against Lyme disease and other vector-borne diseases.”
The consumers also raised several potential barriers to accepting a Lyme disease vaccine. Below are a few of the consumers’ concerns:
“Four consumers expressed concerns about side effects, with most others assuming it would have minimal risks. Three consumers suggested that potential side effects may make a vaccine more risky than other preventive behaviors.”
“Four consumers shared that they prefer to avoid vaccines in general. Two consumers also mentioned generally that anti-vaccine sentiment in their communities might be a barrier for vaccine acceptance more broadly.”
“Two consumers mentioned that the vaccine could create a false sense of security among recipients if the vaccine was not completely protective against Lyme disease.”
One in three of the consumers were undecided about getting a Lyme disease vaccine for either themselves or a family member.
Survey Limitations
The participants were not asked to review the safety and efficacy of the LYMErix vaccine or a future vaccine. The LYMErix vaccine was effective at preventing a rash but only 50% effective at preventing chronic manifestations of Lyme disease, according to the LYMErix package insert.
It is not clear from the survey whether the clinician and consumer participants reviewed what they referred to as “unvalidated claims of the vaccine causing Lyme arthritis.” It is also unclear how to generalize their results, as the investigators excluded “Individuals who strongly disagreed with the importance of vaccines in general.” Finally, it is unclear whether the authors informed the participants that a Lyme disease vaccine would not protect a person from a co-infection.
The following questions are addressed in this Podcast episode:
1. What was the LYMErix vaccine based on?
2. What were the benefits and problems with the LYMErix vaccine?
3. What was your experience with the LYMErix vaccine?
4. Why would a Lyme disease vaccine be helpful?
5. What new vaccines have been introduced?
6. Do you agree with the participants concerns with a Lyme disease vaccine?
7. Is there a vaccine for co-infections?
8. How important would it have been to include participants who strongly disagreed with the importance of vaccines?
Thanks for listening to another Inside Lyme Podcast. Please remember that the advice given is general and not intended as specific advice to any particular patient. If you require specific advice, please seek that advice from an experienced professional.
Inside Lyme Podcast Series
This Inside Lyme case series will be discussed on my Facebook page and made available on podcast and YouTube. As always, it is your likes, comments, and shares that help spread the word about this series and our work. If you can, please leave a review on iTunes or wherever else you get your podcasts.
References:
Devchand R, Koehler L, Hook S, et al. Understanding consumer and clinician perceptions of a potential Lyme disease vaccine. Health Educ Res. Sep 16 2021;doi:10.1093/her/cyab032
__________________
**Comment**
The elephant in the room of course is WHY should we trust these people at all when they’ve never come clean over Lymerix or anything else in Lymeland including the faulty testing and Lyme “guidelines” which have ruled like an Iron Curtain. They’ve never admitted to persistent/chronic infection or that people were severely damaged from the first vaccine.
Interesting they left out those with anti-vaccine beliefs. Just erase people. Sure. Makes sense. Nothing to see here.
But that doesn’t stop those who care more about profits than people and more “vaccines” are in the works, but they haven’t dealt with the previous problems or come clean in any way, shape, or form:
Unfortunately, people still get infected. Some are infected congenitally, others aren’t fortunate enough to be diagnosed and treated early. And some researchers state you can become infected via other routes.
None of these “vaccines” deal with coinfections and most of us are infected with numerous pathogens.
Back in December 2020, a GSK whistleblower stated that the mRNA injections cause sterility in 97% of women, and negatively impact men’s sexual organs as well. Then in June 2021, a vaccine researcher admitted that the toxic spike protein in the injections do not stay in the arm muscle as believed, but goes systemically throughout the body and is found circulating in the blood and accumulating in the ovaries,testes, liver, spleen, bone marrow, adrenal glands and crosses the blood brain barrier. It can bind to receptors that are on our platelets & the cells that line our blood vessels. This can cause platelets to clump, leading to clotting, or bleeding.
Now, a toxicologist is also warning about the COVID shots causing sterility.
**Note**
The article below states more than 300 between ages 12-18 have died of myocarditis due to COVID shots. It doesn’t mention the fact there have been 2,809 fetal deaths in the past 11 months compared to 2,168 fetal deaths following ALL FDA-approved vaccines for the past 30+ years. This is an 80% increase in fetal deaths recorded in VAERS, and yet the CDC & FDA continue to recommend them to pregnant women and nursing mothers. Hello? Go here for an excellent article and video on the topic. And yesterday, Vietnam province HALTS Pfizer injections after 120 students are hospitalized for nausea, high fever, and breathing difficulties. Of the 120, 17 experienced even more severe reactions that require a greater level of medical care and monitoring.
Janci Chunn Lindsay, Ph.D., a molecular biologist and toxicologist, has called for an immediate halt to COVID-19 mRNA and DNA vaccines due to multiple safety concerns
There’s credible concern that the COVID jabs will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may impair fertility and reproductive outcomes
In the case of the COVID shots, important animal studies that help ascertain toxic and systemic effects were not done. We’re now seeing danger signals that are not being heeded. Preliminary safety results of mRNA COVID shots used in pregnant women, published in April 2021, revealed an 82% miscarriage rate when the jab was administered during the first 20 weeks of pregnancy
CDC data reveal more than 300 children between the ages of 12 and 18 have died from myocarditis, a now-recognized side effect of the COVID jab, yet the shot is now authorized for children as young as 5
Since the COVID gene therapies do not prevent infection, but only lessen symptoms, they are actually a treatment, not a prevention. And there are far safer and more effective treatment available, including nebulized peroxide, ozone therapy, and hydroxychloroquine and ivermectin regimens
Janci Chunn Lindsay, Ph.D., is a molecular biologist and toxicologist and director of toxicology and molecular biology for Toxicology Support Services LLC. April 23, 2021, she delivered a three-minute public comment to the U.S. Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices (ACIP).
Her expertise is analysis of pharmacological dose-responses, mechanistic biology and complex toxicity dynamics. In her ACIP comment (see video below), Lindsay described how she aided the development of a contraceptive vaccine in the 1990s that ended up causing unintended autoimmune destruction and sterility in animals which, despite careful pre-analysis, had not been predicted. She explains:
“We were developing what was meant to be a temporary contraceptive vaccine, which was very attractive because it prevented fertilization rather than preventing implantation — or it should have; that was the idea.
Unfortunately, even though quite a bit of analysis was done in different animal models to make sure that it did not have an autoimmune action, it did end up having an autoimmune action and caused complete ovarian destruction.
Now it’s used in that manner [for permanent sterilization] in dogs, cats and other animals. So, that’s a cautionary tale of how animal studies can help us avoid mistakes in humans when they’re used properly, and when proper animal studies are done.”
We May Be Sterilizing an Entire Generation
At the time, she called for an immediate halt to COVID-19 mRNA and DNA vaccines due to safety concerns on multiple fronts. In particular, she noted there is credible concern that they will cross-react with syncytin (a retroviral envelope protein) and reproductive genes in sperm, ova and placenta in ways that may “impair fertility and reproductive outcomes.”
Not a single study has disproven this hypothesis, she noted. Another theory of how these injections might impair fertility can be found in a 2006 study,1 which showed sperm can take up foreign mRNA, convert it into DNA, and release it as little pellets (plasmids) in the medium around the fertilized egg.
The embryo then takes up these plasmids and carries them (sustains and clones them into many of the daughter cells) throughout its life, even passing them on to future generations. It’s possible that the pseudo-exosomes that are the mRNA contents would be perfect for supplying the sperm with mRNA for the spike protein.
So, potentially, a vaccinated woman who gets pregnant with an embryo that can (via the sperms’ plasmids) synthesize the spike protein according to the instructions in the vaccine, would have an immune capacity to attack that embryo because of the “foreign” protein it displays on its cells. This then would cause a miscarriage.
“We could potentially be sterilizing an entire generation,” Lindsey warned. The fact that there have been live births following COVID-19 vaccination is not proof that these injections do not have a reproductive effect, she said.
Lindsay also pointed out that reports of menstrual irregularities and vaginal hemorrhaging in women who have received the injections number in the thousands,2,3,4 and this too hints at reproductive effects. In this interview, we dive deeper into these mechanisms.
Something Has Gone Horribly Wrong
When asked how she ended up getting so passionately involved in this controversial topic, Lindsay replies:
“I became interested in the issue because science was not making sense anymore. For instance, herd immunity was being redefined. Herd immunity has always been defined by a combination of the natural infection with vaccination practices that work.
Suddenly, herd immunity was changed to only being attained through vaccination, and I knew that that was horribly wrong, yet it was being touted everywhere. It was certainly being touted by [Dr. Anthony] Fauci and others who know better.
Other things were also happening within the scientific world. Two of our top tier journals, The New England Journal of Medicine and The Lancet, published fraudulent hydroxychloroquine studies.
Ostensibly they had gone through peer review, and it should’ve been easy to catch the errors in these studies — as well as many other studies that allow for the emergency use authorization of these gene therapies — and they weren’t caught.
Hydroxychloroquine and ivermectin are very safe. They’ve been used safely in pregnant women and children for decades, and suddenly they were being vilified as if they were not safe. As a toxicologist, I know they are safe.
So, these types of things really piqued my attention along with all of the stuff going on in the background with respect to the New World Order and the agenda set by the World Economic Forum, and our joining into this, along with so many other countries, despite their intent, their materials, which claim life will be changed as we know it.
We will ‘own nothing and be happy [about it]’ in just a few years. All of these things converged for me into a sense that something had gone horribly wrong, that our regulatory institutes were captured, and that our scientific journals were not being honest anymore …
There’s a paper that came out in 2006 called ‘Disease Mitigation Measures in the Control of Pandemic Influenza.’5 This paper is wonderful. It goes through World Health Organization and CDC guidelines on how to react during a pandemic, what works and what doesn’t work, and it clearly points out that masks don’t work.
They knew at that point they don’t work. Travel lockdowns don’t work. It’s a wonderful paper to basically go through everything we have done in response to this pandemic, and say that’s an inappropriate way to respond, and we have scientific data that proves it. So, I encourage everybody to go back to that paper … to really see how crazy we’ve gotten in the mandates that make no scientific sense at all.”
Massive Danger Signal Is Being Ignored
As noted by Lindsay, in the case of the COVID shots, important animal studies that help ascertain toxic and systemic effects were not done. But we’re still seeing danger signals that need to be heeded.
Preliminary safety results of mRNA COVID shots used in pregnant women, based on data from the V-Safe Registry, were published in The New England Journal of Medicine (NEJM) in April 2021.6
According to this paper, the miscarriage rate within the first 20 weeks of pregnancy was 12.5%, which is only slightly above the normal average of 10%. (Looking at statistical data, the risk of miscarriage drops from an overall, average risk rate of 21.3% for the duration of the pregnancy as a whole, to just 5% between Weeks 6 and 7, all the way down to 1% between Weeks 14 and 20.7)
However, there’s a distinct problem with this calculation, as highlighted by Drs. Ira Bernstein and Sanja Jovanovic, and Deann McLeod, HBSc, of Toronto. In a May 28, 2021, letter to the editor, they pointed out that:8
“In table 4, the authors report a rate of spontaneous abortions <20 weeks (SA) of 12.5% (104 abortions/827 completed pregnancies). However, this rate should be based on the number of women who were at risk of an SA due to vaccine receipt and should exclude the 700 women who were vaccinated in their third-trimester (104/127 = 82%).”
In other words, when you exclude women who got the shot in their third trimester (since the third trimester is AFTER week 20 and therefore should not be counted when determining miscarriage rate among those injected BEFORE week 20), the miscarriage rate is a whopping 82%.
Of those 104 miscarriages, 96 of them occurred before 13 weeks of gestation, which strongly suggests that getting a COVID shot during the first trimester is an absolute recipe for disaster.
“They concluded, very fraudulently, in my estimation, that it was safe to vaccinate in the third trimester, and said nothing about the clear safety signal in the first trimester,” Lindsay says. “It’s just so dishonest, so purposefully manipulative.”
As for the women who get the shot in their third trimester, there’s still no telling what the ramifications might be in the long term.
“We just don’t know, and that’s the problem,” Lindsay says. “There are all kinds of things that can go wrong with these types of therapies, and have gone wrong in animal models. We don’t know what will happen in the future for these women or for their children. This could be passed on.
We’re seeing now a lot of mention of constitutive expression, whether that’s failure of the mRNA to degrade or integration into the genome. That’s still being investigated.”
Children Are Dying From COVID Jab-Induced Myocarditis
Lindsay goes on to cite a CDC report that shows more than 300 children between the ages of 12 and 18 have died from myocarditis, a now-recognized side effect of the COVID jab.
We also know, based in part on whistleblower testimony, that more than 50,000 Americans have died within three days of these shots,9,10 and that’s just from one database (the Vaccine Adverse Event Reporting System or VAERS). There are 10 other databases that feed into the CDC that the public does not have access to.
“This many deaths, it’s appalling and alarming,” Lindsay says. “Dr. Peter McCullough says the safety signal for typical vaccines, other than this gene therapy, would’ve been around 186 total. We’re now up to [17,128 reported deaths in VAERS, as of October 15, 202111], but they haven’t paused this in children.
They have not paused this while they’re investigating the myocarditis. Instead, they’re pushing it even more. Has this ever happened before? I mean, does this happen in a scenario where the population is at essentially zero risk for the disease? …
The cardiac deaths alone in perfectly healthy kids, and pulmonary embolism deaths in kids, should’ve stopped this. They are at no risk [from COVID-19]. There is no reason to vaccinate them, absolutely zero reason to give them these gene therapies because they’re at no risk [from the infection] …
You know [the shot] is causing heart failure, pulmonary emboli, cardiac arrest in healthy teenagers, and you’re not pausing to investigate the risk versus reward scenario? Something is horribly wrong.
Unfortunately, our regulatory institutions are not going to stop this. They’ve clearly been captured. It’s something that we’re going to have to do. Vaccinated and non-vaccinated must stand together to say, ‘No, you’re not going to experiment on my children’ …
With the RSV vaccines and the dengue fever vaccines, we had deaths in children that were much fewer in number that stopped those campaigns as well. It’s very, very clear — if you don’t get anything else out of this interview with me, understand that our regulatory and safety agencies have been captured.
They’re not doing their job to protect you or your children. You must not trust them, because they are not doing anything according to practices that used to be adhered to. It’s clear that they’ve been captured and compromised, and I hate to say that. I really hate to say that, but that’s the only logical answer …
We have all these breakthrough cases too. If you look at Michigan, and I’ve actually been privy to some other databases of true death numbers in different states [comparing] those who are vaccinated and those who don’t, and I can tell you that the media is lying with respect to the unvaccinated making up 99% of hospitalizations. They’re absolutely lying.”
How the Jab Can Sabotage Fertility
Getting back to the fertility issue, Lindsay cites a Singaporean study that examined the COVID jab’s ability to interfere with fertility by triggering anti-syncytin-1. The study included 15 women, two of whom were pregnant. She explains:
“They did something that I had asked to be done a long time ago, which was to measure anti-syncytin antibodies in an ELISA test. The syncytins are conformationally and genetically similar to the [SARS-CoV-2] spike protein, this fusogenic spike protein.
The thought by several experts was that you could have an autoimmune reaction to the syncytins by developing an immune reaction to the spike protein, and then that would prevent successful pregnancy.
But the syncytins are also important in a number of psychological diseases, such as bipolar depression. They’re important on autoimmune disease, lupus and multiple sclerosis. They are present in skeletal muscle. There’s some association with breast cancer. They’re really important ancient retroviral elements.
What this study found was extremely interesting. It found that every single one of these women who had been vaccinated developed autoantibodies to syncytin-1. Now, the authors kind of dismissed this and said, ‘Oh, but we don’t think that those antibodies were high enough to mean anything.’
But there was a clear difference between the pre-gene therapy sera [blood sample] and the post-therapy sera … What it shows is that there is an antibody response, and the significance of it, we don’t really know. But every single one of the women developed an antibody response that was different from the baseline … and I think that’s probably what’s causing some of these pregnancy losses.”
Are COVID Jabs a Population-Wide Immunocontraceptive?
When asked what she thinks the motive behind this mass injection campaign might be, considering the clear danger signals, she replies:
“I certainly think that to discount that it is a form of population-wide contraceptive would be naïve. There’s a paper that came out in 2005. It’s called ‘Evaluation of Fusogenic Trophoblast Surface Epitopes as Targets for Immune Contraception.’12
This paper tried to find contraceptive peptides in persons that had infertility problems already that were isolated to placentation. So, it was taking a backwards approach, getting the sera from people who had fertility problems and trying to see what they had antibodies to that was causing the fertility problems …
This work was sponsored by the WHO and the Rockefeller Foundation [and the National Institutes of Health]. No surprise there. It was then picked up by a company called AplaGen that took it to patent in 2007.
These are 12-mer peptides, and there’s a series of eight of them that can be used to induce sterility. When they patented it, they also said that it could be used to ameliorate sterility. Interestingly, it was also associated with all of the things that we know syncytin is associated with, — lupus, skeletal muscle disorders, bipolar depression [and] a number of other things.
Even though they don’t name syncytin proteins as the proteins that are targeted, they worked backwards from these peptides, and then said they were a series of other proteins. Sometimes we know that proteins can be called the same thing in different discovery realms. So, that’s going to take more research, but it was certainly interesting to me.
What it really points out is that there were efforts to use peptides or immunocontraceptive means at the placental trophoblast interface to cause sterilization … So, it would be naïve to think that this was not on the plate for future use.”
How Long Will Effects Last?
An obvious question is, how long might these effects last? Are they lifelong? Of course, any answer we come up with here will be hypothetical only, as the studies simply haven’t been done. That said, with her background in molecular biology, Lindsay is at least qualified to theorize.
The mRNA is extremely fragile, which is why a nanolipid with polyethylene glycol delivery system is used. In addition, about 30% of the mRNA has been genetically modified to decrease degradation. As a result, the mRNA being injected is magnitudes sturdier than natural mRNA.
What’s more, the nanoliposomes allow for superior penetration into tissues, and we now know it spreads throughout your body. It doesn’t stay in your deltoid. How long this modified and stabilized mRNA remains viable is still unknown, however. A corollary question is whether this mRNA might be integrated into your genome to become a permanent fixture.
“The answer is, we don’t know for sure,” Lindsay says. “Of course, with the adenoviral vector vaccines [Janssen and AstraZeneca], they’re more prone to integration into the genome. We know that from animal studies and past experiments.
With the mRNA technology, we’ve never stabilized something like this in this manner. What we do know is that recent studies have come out — Bruce Patterson’s group and another group — both came out with the finding that the spike protein is being expressed, [it’s] present on monocytes, as far out as from the time that the people were given the gene therapy.
So, that gives us an indication that it is resistant, for sure, to degradation. The longer it stays around, and is resistant to degradation, the more likely that genomic integration events can occur. But I don’t know the answer to whether or not it will become a permanent feature.”
Make a Rational Choice
As explained by Lindsay, no coronavirus vaccine has ever been successfully brought to market, despite 20 years of effort. All have failed due to antibody dependent enhancement, where the vaccination facilitates infection rather than protects against it.
Now, we’re to believe a safe and effective coronavirus “vaccine” has been developed in mere months. She also makes another important point. Since the COVID gene therapies do not prevent infection, but only lessen symptoms, they are actually a treatment, not a prevention.
And there are far safer and more effective treatments available, including nebulized peroxide, ozone therapy, and hydroxychloroquine and ivermectin regimens.
“If all these gene therapies do is lessen the diseases, then they’re not a vaccine, they are a treatment,” she says. “They are a treatment that you don’t know the mid- or long-term consequences of, that have already caused a number of adverse events. You have to use your common sense to say, why wouldn’t I use a treatment that has been known to be safe over 70 years as opposed to one that is brand-new, that is experimental?”
Other Safety Signals
Aside from fertility issues, heart inflammation and blood clots, another side effect seen among the fully “vaccinated” is de novo Type 1 diabetes in adults. This makes sense considering Pfizer’s biodistribution study showed the spike protein accumulates in the pancreas. The natural SARS-CoV infection can also have this effect.
Type 1 diabetes is a serious problem, as it leaves you metabolically handicapped for the rest of your life, dependent on extremely costly insulin injections. Doctors are also reporting an increase in pancreatic cancer and acute myeloid leukemia.
Where Do We Go From Here?
“Many scientists and physicians feel as I do, and are trying to figure out where we go from here,” Lindsay says, “because our typical safety and regulatory agencies have been compromised.” She believes we need to continue sharing the data and facts that mainstream media refuse to discuss, and continue urging those who have received the jab to at least protect their children.
“We need to stand together as one people and say we’re not going to accept this, especially not for our children, and try to get to the bottom of this and see what’s really behind all these efforts. Is it really about a virus, or is it more about other political motivations and campaigns, as it seems to be?”
I’m less optimistic about the idea of breaking through the brainwashing to get people to not sacrifice their children. So many have their minds set in cement with the wrong information. They could have their brother, sister, mother or father get the shot and die with the needle still on their arm, and they’d still go out to get a booster the next day.
I’ve seen it so many times. My friends, their parents, their siblings and loved ones — there’s this barrier that prevents any openness to new information. They’ve made their decision.Mark Twain said, “It’s far easier to fool someone than to convince them they’ve been fooled.” And it’s true.
So, while I agree that we must keep trying, and have faith that truth will prevail, I also think it’s important to have realistic expectations. We’re up against the most effective propaganda campaign in modern history. It’s psychological warfare at its best.
From my perspective, being a pragmatic realist, I believe the best strategy is to reinforce and support those who didn’t buy into the propaganda narrative to begin with, because they don’t struggle with that cognitive dissonance. If we stick together and support each other, so none of us get sucked into the lunacy, then we can at least preserve the control group.
Ultimately, the truth will come out, as long as we can preserve the control group. In a year or two, or three, we will clearly be able to tell how devastating this intervention was simply by comparing the two groups. I suspect those who got the shot will be severely crippled in various ways, and those who didn’t get the shot will have far better health in comparison.
“I absolutely agree that we have to preserve a control group. We also have to think of ways that we can help those that have been injured. I brought this out in a letter I recently wrote, advocating for Dr. McCullough.
People who have gotten this inoculation, if they have mid- to long-term effects, if you deny that any adverse effects are really going on, then the efforts going into those treatments for people who are having side effects are not going to be there. We have to accept that these [side effects] are real in order to help people who have already taken the inoculations, and I believe we have to try.”
Powassan virus lineage 2 (deer tick virus) is an emergent threat to American public health, causing severe neurologic disease. Its life cycle in nature remains poorly understood. We use a host-specific retrotransposon-targeted real time PCR assay to test the hypothesis that white-footed mice, considered the main eastern U.S. reservoir of the coinfecting agent of Lyme disease, is the reservoir for deer tick virus. Of 20 virus-infected host-seeking nymphal black-legged ticks 65% fed on shrews and none on mice. The proportion of ticks feeding on shrews at a site is positively associated with prevalence of viral infection, but not the Lyme disease agent. Viral RNA is detected in the brain of one shrew. We conclude that shrews are a likely reservoir host for deer tick virus and that host bloodmeal analysis can provide direct evidence to incriminate reservoir hosts, thereby promoting our understanding of the ecology of tick-borne infections.
Borrelia miyamotoi in Human-Biting Ticks, United States, 2013–2019
Guang Xu , Chu-Yuan Luo, Fumiko Ribbe, Patrick Pearson, Michel Ledizet, and Stephen M. Rich
Author affiliations: University of Massachusetts–Amherst, Amherst, Massachusetts USA (G. Xu, C.-Y. Luo, F. Ribbe, P. Pearson, S.M. Rich); L2 Diagnostics, New Haven, Connecticut, USA (M. Ledizet)
Abstract
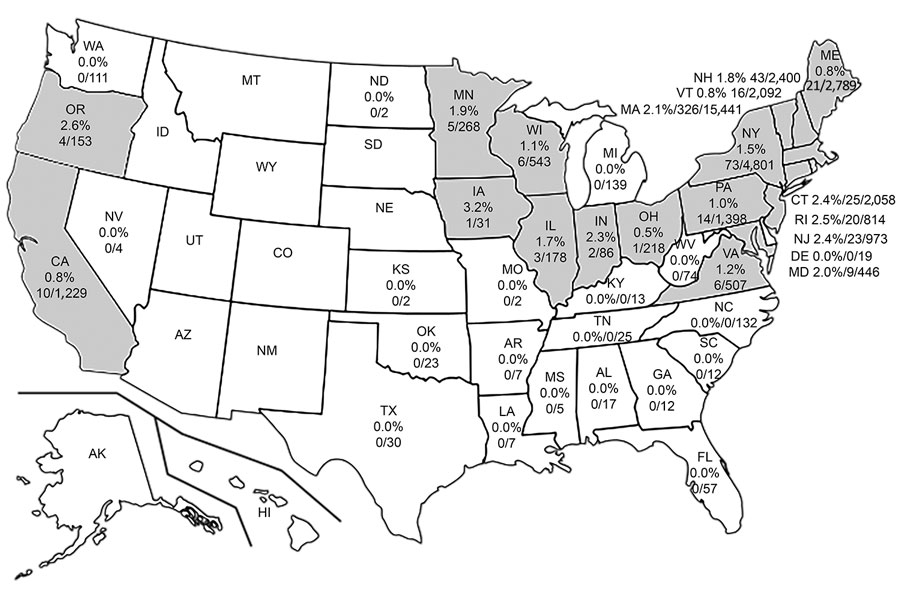
During 2013–2019, Borrelia miyamotoi infection was detected in 19 US states. Infection rate was 0.5%–3.2%; of B. miyamotoi–positive ticks, 59.09% had concurrent infections.B. miyamotoi is homogeneous with 1 genotype from Ixodes scapularis ticks in northeastern and midwestern states and 1 from I. pacificus in western states.
Since Borrelia miyamotoi is NOT a reportable illness to the CDC, no one has any clue about prevalence, but reports are coming in continually that it’s highly likely to be a much bigger problem than ‘authorities’ believe.