When Lyme Changes Your Brain
https://www.lymedisease.org/lyme-related-brain-fog-is-real/
Advanced imaging shows Lyme-related brain fog is real
By Nancy Dougherty
Johns Hopkins Medicine Lyme Disease Research Center
There are approximately 476,000 people diagnosed with Lyme disease annually in the US. Of these, an estimated 10-20% suffer from impairing symptoms well beyond the acute phase of infection.
Persistent symptoms include severe fatigue, pain, and cognitive problems. Vexingly, these symptoms can be difficult to validate using current diagnostic tests.
Patients are often told by their health practitioners: “your tests are normal, it’s in your head” (aka psychosomatic).
Researchers have discovered, however, that by using more advanced imaging modalities, brain changes can be objectively detected in Lyme disease patients.
For example, clinical researchers at Johns Hopkins University School of Medicine have used novel PET imaging, functional MRI (fMRI), and diffusion tensor imaging (DTI) to identify inflammatory, functional, and structural abnormalities in the brains of Lyme disease patients as compared to healthy controls.
Their findings indicate that Lyme-disease-associated brain alterations are biologic and measurable, not psychosomatic. These discoveries are significant but not yet well known by the physician community or broadly available to clinicians.
What does “brain fog” mean?
Brain fog is a term used to describe difficulties with cognitive functions such as working memory, focusing, concentrating, planning, organizing, word recall, processing speed, and mental fatigue.
Working memory enables one to do tasks quickly or easily solve a problem without looking up information. This includes quickly learning a new computer program or using names or numbers for a routine task.
Mental fatigue is akin to how one feels after taking a long test that requires remembering detailed information or doing a complicated mental task when short on sleep.
What are the limitations of current clinical tests for Lyme-associated brain fog?
Brain fog is commonly experienced by Lyme disease patients but difficult to detect because cognitive deficits can be too subtle for standard diagnostic tests to uncover.
Usual blood tests appear normal in Lyme encephalopathy or brain fog (CBC; CMP: kidney, liver, glucose, thyroid; ESR, CRP).
Serum blood testing for 2-tier IgG Borrelia burgdorferi antibody seropositivity may be negative in patients, such as those with past antibiotic treatment.
Clinically available MRI imaging is usually normal or shows nonspecific changes. Cerebrospinal fluid examination findings are usually normal as well. In some cases, the CSF fluid may show evidence of a mild form of encephalomyelitis, but this is rare.
Formal cognitive testing with a neuropsychologist to characterize the type and severity of cognitive problems can be a more helpful approach. Working memory and processing speed have been shown to be impacted in Lyme disease patients using standardized neuropsychological measures.[i] However, patient-reported cognitive complaints are subjective, and objective measures of cognitive decline are sought after by patients and clinicians.
What does more advanced neuroimaging reveal?
Non-standard research-grade neuroimaging technologies have discovered marked biologic abnormalities in patients with Lyme disease as compared to healthy controls.
A Columbia University brain PET imaging study (2009) found hypometabolism in Lyme-disease-associated encephalopathy.[ii]
A Johns Hopkins University School of Medicine brain PET imaging study (2018) revealed increased inflammation and glial activation in patients with Lyme-disease-associated persistent symptoms.[iii]
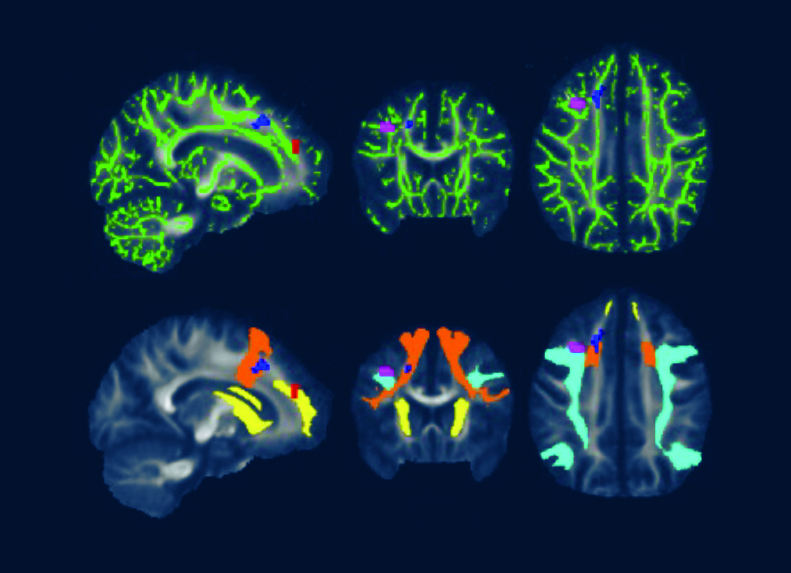
A 2022 Johns Hopkins University School of Medicine neuroimaging study utilized fMRI and DTI brain scans in conjunction with each other. These scans identified striking functional abnormalities as well as distinct structural changes in the white brain matter of Lyme disease patients.[iv]
What is the significance of these neuroimaging findings?
John Aucott, MD, Director of the Johns Hopkins Medicine Lyme Disease Research Center and Associate Professor of Medicine at Johns Hopkins University School of Medicine, explains, “The cause of Lyme-disease-associated persistent symptoms typically cannot be identified with regular MRIs, CT scans, or blood tests. However, in a research setting, more sophisticated PET, fMRI, and DTI imaging approaches have found significant objective abnormalities in the brains of Lyme disease patients compared with healthy controls.”
Cherie Marvel, PhD, lead author of the fMRI/DTI study and Associate Professor, Departments of Neurology & Psychiatry at Johns Hopkins University School of Medicine, describes fMRI as “a quantitative ‘brain stress test’ that measures brain function during cognitive tasks.”
Dr. Marvel explains that “the brain scans indicate Lyme disease patients’ brains work harder than normal and unexpectedly by activating white matter in the frontal lobe to try to maintain normal function.”
DTI, a measure of structural brain integrity, confirms abnormalities in the same white matter regions as observed in the fMRI scans.
These novel neuroimaging results provide new objective validation of a biologic basis for the brain fog reported by Lyme disease patients, including working memory impairment and slower processing speed.
The findings indicate Lyme-disease-associated brain fog is real and likely due to ongoing neuroinflammation driving brain dysfunction. More research is needed to better understand the diagnostic and therapeutic implications of these notable discoveries and to bring new insights and more advanced tools into the clinic to help patients.
Big picture
The Lyme-disease-associated advanced neuroimaging brain findings may be relevant to other infection-associated chronic illnesses where neuroinflammation is also significant, including Long COVID and ME/CFS. On June 29-30, 2023, a National Academies of Sciences, Engineering and Medicine workshop will “examine common biological and clinical factors associated with infection-associated chronic illnesses.” Infection-associated brain fog is one topic this workshop can hopefully shine additional light on to help accelerate knowledge and solutions for patients.
Nancy Dougherty is an Education and Communications Consultant for Johns Hopkins Medicine Lyme Disease Research Center. Follow her on Twitter: @NancyNDougherty.
References
[i] Touradji P, Aucott JN, Yang T, Rebman AW, Bechtold KT. Cognitive Decline in Post-treatment Lyme Disease Syndrome. Arch Clin Neuropsychol. 2019 Jun 1;34(4):455-465. doi: 10.1093/arclin/acy051. PMID: 29945190. https://pubmed.ncbi.nlm.nih.gov/29945190/
[ii] Fallon BA, Lipkin RB, Corbera KM, Yu S, Nobler MS, Keilp JG, Petkova E, Lisanby SH, Moeller JR, Slavov I, Van Heertum R, Mensh BD, Sackeim HA. Regional cerebral blood flow and metabolic rate in persistent Lyme encephalopathy. Arch Gen Psychiatry. 2009 May;66(5):554-63. doi: 10.1001/archgenpsychiatry.2009.29. PMID: 19414715. https://pubmed.ncbi.nlm.nih.gov/19414715/
[iii] Coughlin JM, Yang T, Rebman AW, Bechtold KT, Du Y, Mathews WB, Lesniak WG, Mihm EA, Frey SM, Marshall ES, Rosenthal HB, Reekie TA, Kassiou M, Dannals RF, Soloski MJ, Aucott JN, Pomper MG. Imaging glial activation in patients with post-treatment Lyme disease symptoms: a pilot study using [11C]DPA-713 PET. J Neuroinflammation. 2018 Dec 19;15(1):346. doi: 10.1186/s12974-018-1381-4. PMID: 30567544; PMCID: PMC6299943. https://pubmed.ncbi.nlm.nih.gov/30567544/
[iv] Marvel CL, Alm KH, Bhattacharya D, Rebman AW, Bakker A, Morgan OP, et al. (2022) A multimodal neuroimaging study of brain abnormalities and clinical correlates in post treatment Lyme disease. PLoS ONE 17(10): e0271425. https://doi.org/10.1371/journal.pone.0271425
Caption for featured photo: DTI brain images from a 2022 Johns Hopkins University School of Medicine study show white matter changes associated with post treatment Lyme disease.
_________________
**Comment**
What’s important is what will they do with this information and what will they attribute the brain changes to. For instance, currently, and for the entire history of Lyme/MSIDS, these issues have been blamed upon PTLDS – an autoimmune/inflammatory type of condition that will be treated with things like steroids when the very real underlying problem could be persistent infection(s). This has become highly politicalized, causing polarity in research and medicine.
Unfortunately, this article, like so many others before it emphasizes and pushes the accepted narrative about the consequences or supposed failure of prolonged antibiotics for Lyme/MSIDS. Everyone understands that prolonged antibiotic use is not without risks; however, nobody seems to care when it’s for acne, salmonella, endocarditis, sickle cell, or rheumatic fever. Further, this report states there is significant information that supports the safety of prolonged antibiotic use regarding penicillin and its derivatives.
Again it’s about benefit vs risk.
When you are faced with death or a life of misery, all of a sudden the risk of prolonged antibiotics falls on the priority list. Further, many, including myself and my husband have achieved our health back after this therapy.
Of course antibiotics aren’t the only tool in the tool kit needed for treating Lyme/MSIDS. It truly is a complicated illness and one must learn all they can about diet, supplements, herbs, immune modulators, etc., but that doesn’t mean antimicrobials don’t have a very important role.
Lastly, there are good reasons why extended antibiotics haven’t appeared successful in many NIH funded studies. This is because:
- typically a monotherapy is utilized, which frankly often isn’t enough with Lyme/MSIDS, plus there’s the concern of antibiotic resistance with this myopic approach
- often the wrong antibiotic is used
- often the wrong dosage of antibiotic is used
- often, individual differences are not taken into account for example, symptoms must be monitored carefully and antibiotics changed when patients hit a plateau. This approach doesn’t fit into the current research paradigm.
- many other research design flaws such as only accepting those who test positive on 2-tiered CDC testing which is known to miss more than 70% of all cases, as well accepting patients that have the EM rash which is highly variable
For a fantastic overview on treatment nuances listen to Dr. Burrascano on the history of Lyme which I highlight here.
In brief:
- Treat ALL forms of Bb
- Treat coinfections
- Treat long enough (Bb is slow-growing and persistent)
- Make sure blood levels of antibiotics are high enough as people vary. He discusses amoxicillin and how they found that increasing the dosage to 1,000mg 3X/day and adding probenecid to increase the antibiotic in the blood, people did even better. He goes on to tell of an unpublished study with Stoneybook where there was a failure rate of 100% of patients taking 300mg of doxycycline a day for 21 days. Yet, how many people are given this exact treatment?
- Cycle treatment. This means, once you are symptom-free for 2-4 months, stop treatment. If symptoms return, treat again. Burrascano has found that it typically takes 3-4 Cycles before a person remains symptom-free. The 3rd cycle often yields the worst herx in his experience.
https://madisonarealymesupportgroup.com/2018/04/13/chronic-lyme-post-mortem-study-needed-to-end-the-lyme-wars/ In this astute editorial, Microbiologist Tom Greer states:
From the very beginning, treatment failures were seen in virtually every antibiotic study done. The longer the patient follow up, the higher the incidence of treatment failure. The medical community blamed early treatment failures on the older antibiotics erythromycin, tetracycline, and penicillin, and determined that these antibiotics were not very effective at curing Lyme disease. Ignored was the fact that the newer antibiotics were also consistently failing to prevent relapses of active infection. Since these early treatment studies, the concept that two weeks of antibiotic therapy is adequate treatment for Lyme disease has remained ingrained in the medical community’s collective consciousness. [The Long-Term Follow-up of Lyme Disease: A Population-Based Retrospective Cohort Study. Authors: Shadick NA; Phillips CB; Sangha O et al. Ann Intern Med 1999 Dec 21;131(12):919-26]
*Data presented by Dr. Nancy Shadick at an International Lyme Symposia showed that patients in the Nantucket Island study followed for up to 5.2 years after initial antibiotic treatment had ever-climbing relapse rates. Relapse rates in patients receiving two weeks of IV Rocephin (ceftriaxone) could expect a relapse rate to exceed 50% after five years.
There is a smart way to treat this, yet few are nuanced in this skill. We desperately need post-mortem studies to determine what is keeping people ill. We need current transmission studies. We need doctor education on the polymicrobial aspect of this disease. And, we need the stigma & polarization to go away so insurance companies will cover Lyme/MSIDS medical expenses, patients will be believed and supported and the bullying will end.