
https://popularrationalism.substack.com/p/sars-cov-2-spike-protein-takes-the
SARS-CoV-2 Spike Protein Takes the Gloves Off and Causes Chronic Inflammation
Studies show the NLRP3 Inflammasome response is unleashed by the Spike protein. It’s around for 4 months. Aberrant NLRP3 inflammasome response leads to chronic illness and death. What you can do.
|
|
|
I enjoy doing research, but I hate it when the evidence is so depressing. Thank goodness for Dr. Levy. You’ll see why at the end.
This is the study that set me off:
Long-lived macrophage reprogramming drives spike protein-mediated inflammasome activation in COVID-19 https://www.embopress.org/doi/full/10.15252/emmm.202114150
The NLRP3 Inflammasome Response
The NLRP3 Inflammasome response is one of the myriad normal responses by which mammalian immune systems activate against viral infection. It’s supposed to be a short-term response than shuts down after the pathogen is defeated.
Good news: Spike protein primes the NLRP3 Inflammasome.
During infection, the NLRP3 Inflammasome response does its jobs.
Very bad news: Spike protein primes the NLRP3 Inflammasome, is systemic, and is found 4 months following injection.
After injection (and during Long-Haul COVID (LHC)), the NLRP3 Inflammasome response and must be doing chronic, systemic damage.
Spike Not Localized
The spike protein is not localized but is, per this Harvard study, systemic following injection
Circulating Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Vaccine Antigen Detected in the Plasma of mRNA-1273 Vaccine Recipients https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciab465/6279075
It is around for a lot longer than the virus:
While this Ogata study found the antigen up to15 days in 3/15 patients (20%),
This study found it in circulating exosomes up to 4 months(!)
Exosomes Cutting Edge: Circulating Exosomes with COVID Spike Protein Are Induced by BNT162b2 (Pfizer-BioNTech) Vaccination prior to Development of Antibodies: A Novel Mechanism for Immune Activation by mRNA Vaccines https://pubmed.ncbi.nlm.nih.gov/34654691/
Boosters Mean Repeated Chronic Inflammation
With never-ending boosters, we’re going to see chronic illness in the vaccinated at rates that are undeniable. None of it will be attributed to the vaccine.
More boosters means more chronic illness and death. Science tells us we can expect increased cancer, neurodegenerative disease, and a host of sublethal inflammation-mediated symptoms.
Here is a sample of articles that tell us this is necessarily so.
Aberrant NLRP3 Inflammasome Activation Ignites the Fire of Inflammation in Neuromuscular Diseases https://pubmed.ncbi.nlm.nih.gov/34199845/
NLRP3 Inflammasome Activation in Cancer: A Double-Edged Sword
https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC7360837/
Inflammasomes: An Emerging Mechanism Translating Environmental Toxicant Exposure Into Neuroinflammation in Parkinson’s Disease https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC6659017/
Be aware of SARS-CoV-2 spike protein: There is more than meets the eye https://pubmed.ncbi.nlm.nih.gov/34100279/
What You Can Do
Ok, so what’s the solution?
- Remove all other sources of toxins in your life. Thoroughly and urgently. You cannot afford these toxins. (I offer Environmental Toxicology in the Fall – email info@ipak-edu.org subject line “EnvTox” if you’d like me to offer access as pay-per-view (no instructor).
- Sign up for my new course in immunology. We start in the second week of January.
- And/Or sign up for Dr. Brownstein’s new course Wholistic Approaches to Human Health.
- Read this article by Dr. Levy – Canceling the Spike Protein Striking Visual Evidence Editorial by Thomas E. Levy, MD, JD http://orthomolecular.org/resources/omns/v17n24.shtml
- Fund the IPAK Spike Protein Oncogenic Potential Study (new in 2022) VISIT HERE.
For more:
- https://madisonarealymesupportgroup.com/2021/09/15/covid-19-mrna-shots-leading-to-cns-inflammation-a-case-series-on-ms-patients/
- https://madisonarealymesupportgroup.com/2021/07/06/heart-inflammation-linked-to-covid-vaccines-in-study-of-u-s-military-department-of-defense-confirms/
- https://madisonarealymesupportgroup.com/2021/06/11/cdc-admits-teens-injected-with-pfizer-or-moderna-at-higher-risk-of-heart-inflammation/
- https://madisonarealymesupportgroup.com/2020/09/11/astrazeneca-covid-19-vaccine-trial-put-on-hold-due-to-spinal-inflammation-in-participant/
- https://madisonarealymesupportgroup.com/2021/12/23/covid-jabs-reprogram-both-adaptive-innate-immune-responses/
- https://madisonarealymesupportgroup.com/2021/12/22/more-children-have-died-from-covid-shot-than-from-covid-cdc-walensky-lies-about-myocarditis/
__________________
https://popularrationalism.substack.com/p/studies-needed-on-the-oncogenic-potential?
Studies Needed on the Oncogenic Potential of COVID-19 Vaccinations
Fact Checkers deny it but present no new data. We’re doing Science – and taking deep dive into the question of plausibility using molecular evidence using Systems Biology
|
|
|
There has been some discussion on the oncogenic potential of SARS-CoV-2 vaccination – the ability of exposure to COVID-19 vaccines to increase the risk of cancers.
This study area is obviously high priority given the disease burden that could result from mass exposures. To assess plausibility, mechanisms of action (disease pathophysiology) studies are needed.
A little background, and some detail on our project:
Background
Autoimmunity or other molecular antagonism against important cellular processes can lead to cancer. Disruption of processes that mediate DNA replication and repair, for example, or regulate cell division can be oncogenic. Given the importance of immune surveillance in our bodies against new precancerous cells, autoimmunologic impairment of the immune proteins and cells would not only spell disaster for infections, but could also lead to unchecked cancer growth.
The evidence in support of these possibilities is diverse, but hard evidence is difficult to find.
In my April 2020 paper warning against pathogenic priming, I wrote:
Pathogenic Priming
“Remarkably, over 1/3 (11/27) of the immunogenic proteins in SARS-CoV-2 have potentially problematic homology to proteins that are key to the human adaptive immune system (emboldened in Table 1). Mapping of the overall gene list to Pathways via Reactome.org revealed that many functions of the human adaptive immune system might be impacted via autoimmunity against these proteins and their interactors, including MCH(sic) Class I and Class II antigen presentation, PD-1 signaling, cross-presentation of soluble exogenous antigens and the ER-Phagosome pathway.”
This sounds like an argument for vaccination, but it’s not. Subclinical mumps, measles and pertussis infections are well established in the vaccinated. Similarly, following vaccination, the repeated exposure to SARS-CoV-2 virus in the vaccinated might lead to silent, subclinical disease processes due to SARS-CoV-2 virus infection in spite of – or because of – vaccination. These chronic exposures may be more prevalent in the vaccinated than in those with natural immunity. Thus, the question is not merely “does vaccination increase the risk of cancer”, but is better posed as “does repeated exposure to SARS-CoV-2 infections in the vaccinated lead to increased risk of cancer”?.
Dr. Ryan Cole’s Observations
While pooh-poohed by so-called “Fact Checkers”, Dr. Ryan Cole of Idaho saw and in Aug, 2021 reported an uptick in uterine cancers in women who had been vaccinated.
Dr. Cole reported that he was seeing increases is herpes virus, mononucleosis, shingles, human papillomavirus, and uterine cancers: This doctor trained at the Mayo Clinic and runs the largest independent testing laboratory in Idaho. Listen to what his lab testing is showing:
Dr. Burkhardt reported that 93% of post-inoculation autopsies showed lymphocyte penetration in all organs and tissues, and Dr. Bhakdi commented on autopsy findings that cells in the lymph nodes being destroyed following vaccination.
Publications providing evidence of immune impairment
A number of publications support plausibility, and some have been dismissed without new evidence by so-called “Fact Checkers”. Important, the loss of CD8 cells in long-haul COVID was noted by Dr. Bruce Patterson (who I interview on Unbreaking Science on Jan 31, 2020). These are the natural killer cells Dr. Cole was concerned about.
We know that yes, loss of CD8 cells are associated with increased risk of cancer.
This study

is cited by these authors from the University of Texas MD Anderson Cancer Center, Houston, TX, who wrote:
“For instance, SARS CoV-2 proteins, can hijack the human immune response to pathogens and the DNA damage repair system, thereby damaging both innate and adaptive immunity”
The fact-checkers claim that Dr. Cole is mistaken, yet there it is.


Increase in All-Cause Mortality in the UK and Indiana

What We Should Expect in the Molecular and Epidemiologic Evidence
If vaccination sets forth a cascade of events that leads to increased cancer risk in the vaccinated, we should see biological pathways related to the specific cancer types being reported as elevated, including blood cancers and per Dr. Cole, uterine cancers.
In the epidemiologic data, there should be a pulse in the risk of cancer types that is not explained by the increased risk of cancer progression due to the cessation of cancer screening visits that occurred during the lockdown. Unlike the temporary pulse from lock-down related cancers, we should see a sustained increased in cancer rates over time in the vaccinated compared to the unvaccinated. This aspect of this question is not part of the current study, but will be part of another study we will launch later this year.
IPAK SARS-CoV-2 Spike Protein Oncogenic Potential Study
Most of the people vaccinated in the US received spike-only vaccines. Here’s what we intend to do
- Using the known and published immunogenic epitopes in the SARS-CoV-2 spike protein, identity homologies (similarities) with known oncogenic proteins that could lead to autoimmunity against key cancer-related proteins. For this, we’ll canvas the Human Protein Atlas for genes which if mutated confer cancer risk and use the methodology laid out in (Lyons-Weiler, 2020).
- Using pathway analyses, we will characterize which biological pathways are likely to be most influenced.
- We will write the results up for peer-reviewed publication.
- Our preliminary analysis tells us so far that yes, there appear to be impacted biological pathways (preliminary data):


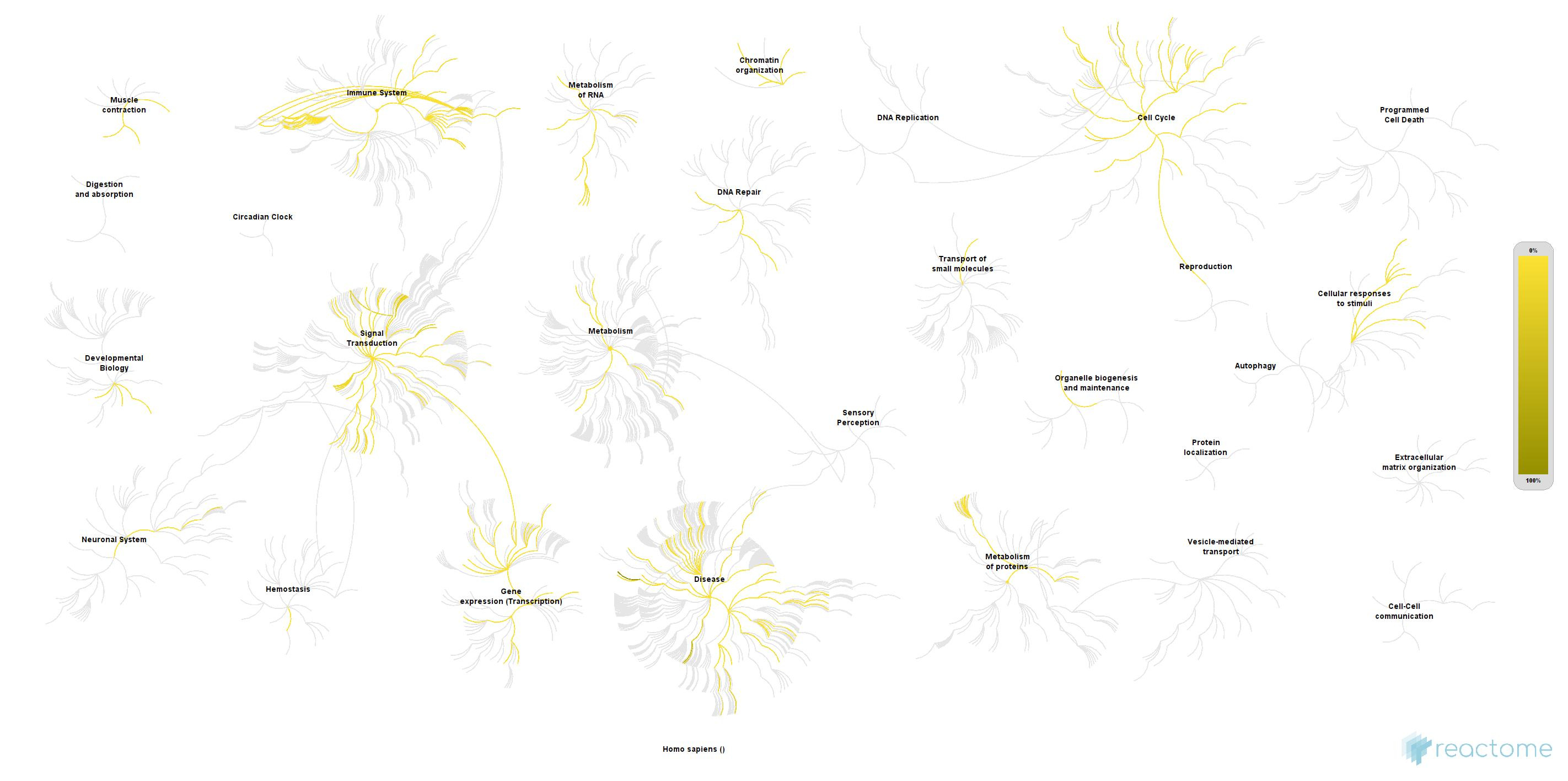
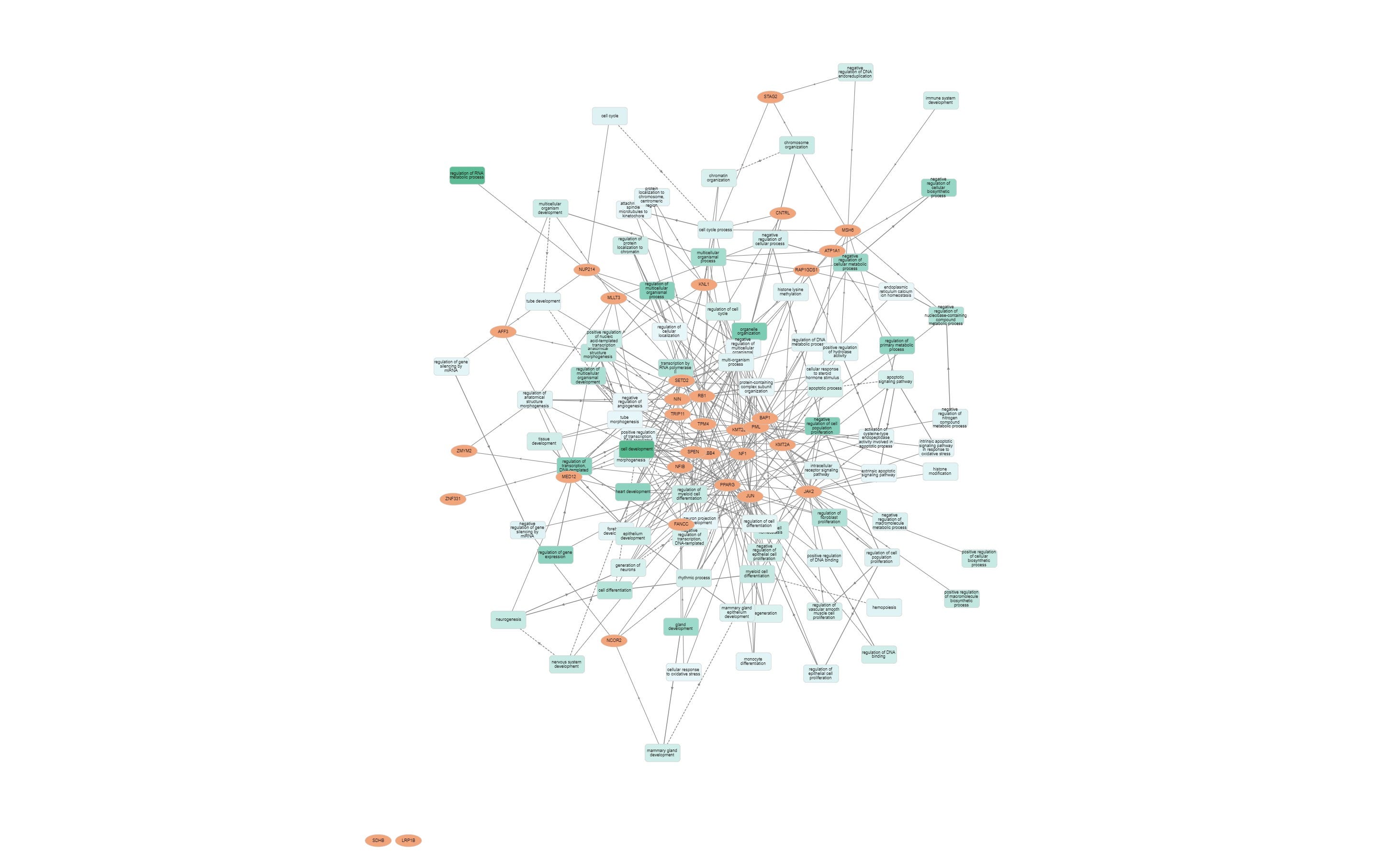
Obviously, I hope this hypothesis is wrong, so we will attempt to disprove it via statistical hypothesis testing using gene enrichment analysis, a statistical technique conducted at the biological pathway level.
All of our studies are funded by the public. We have set up a dedicated donation portal for small monthly donations to IPAK, The Institute for Pure and Applied Knowledge, a not-for-profit in the Commonwealth of Pennsylvania, dedicated to this project. Funds used underwrite the costs of the study as well as any publication fees if we opt for open-access publication (an added step that we prefer to increase distribution).
All knowledge generated by IPAK via research is public domain – none of the knowledge can be used by IPAK for profitable ventures.
So, let’s see whether the hypothesis of increased oncogenic potential is plausible.
https://www.medpagetoday.com/special-reports/exclusives/96412
COVID Vaccine Booster Efficacy Against Infection May Fade Quickly
— New U.K. data suggest steep drop-off in protection, potentially giving Omicron more power

Real-world data from the U.K. showed that efficacy of a third dose of a COVID-19 vaccine waned significantly at the 10-week mark, leaving boosted individuals at risk of infection with Omicron.
In a December 23 U.K. Health Security Agency (HSA) technical briefing, vaccine efficacy against symptomatic infection generally fell to around 40% some 2.5 months after a booster dose. (See link for article)
_________________
Summary:
- HSA assessed 147,597 Delta and 68,489 Omicron cases from November 27 to December 17.
- The Pfizer primary series & booster, showed efficacy against symptomatic disease was 70% immediately after the third dose but fell to 45% at 10 weeks or longer.
- Having a Pfizer primary series but a Moderna booster saw protection against symptomatic disease hover around 70% to 75% for up to 9 weeks post-boost.
- Having a primary series of AstraZeneca, efficacy peaked at 60%, 2 to 4 weeks after either a Pfizer or Moderna booster, then fell to 35% with Pfizer and 45% with Moderna by around 10 weeks.
- They omitted efficacy against severe disease, hospitalization, and death because there weren’t enough Omicron cases admitted to the hospital.
- Data from Israel also suggests waning efficacy after boosters, but the ‘powers that be’ still illogically recommend more boosters despite the fact.
- Data from Israel also showed a doubling in the rate of infection with Delta in ages 60 & up within 4-5 months after a 3rd shot and no indication of reduced efficacy against severe disease. (But remember, they are not looking at absolute risk reduction so it’s all skewed to make the jabs appear efficacious).
- Yet the vaccine cultists keep recommending more jabs. Peter Hotez, MD, PhD, is pushing a 4th shot for healthcare workers due to exposure to Omicron (despite there not being enough Omicron hospitalizations to even use for the study). Hotez is worried about instability in the health system but never stops to ponder the instability caused by the jabs themselves. This one-sided thinking is prolific regarding these shots.
- The article then delves into the oft repeated mantra that these jabs somehow “reduce illness” and proceeds to rattle off all sorts of numbers which you can read for yourself. They end the litany with the following caution: “the findings have low confidence because these are early analyses with small numbers of hospitalizations, limited follow-up time, minimal adjustment for previous infection, and limited spread into the most vulnerable age group.“
