A Strange Itch, Trouble Breathing, Then Anaphylactic Shock
By LISA SANDERS, M.D. JAN. 4, 2018
“I can’t breathe,” the woman panted, her voice a husky monotone. Her sister looked anxiously at the clerk at the triage desk at the University of Iowa hospital emergency room. The woman’s breath was rapid and coarse. Her chest heaved with the work of simply breathing. She pulled at the neck of her sweatshirt — suddenly it was too tight. She pulled it over her head and dropped it to the floor. She was naked beneath the top; she had been in bed when this attack came on.
The 54-year-old woman was helped into a wheelchair and whisked into the inner sanctum of the E.R. What followed was a blur of concerned faces, needles and medical data. Her blood pressure was dangerously low; her heart was racing. She was given epinephrine and steroids, but it was hours before she could explain what had happened that night.
She was staying at her mother’s house in rural Iowa, she told the doctors. Just as she was going to bed, she felt a sudden tingling in the palms of her hands. She recognized the sensation immediately: Twice in the past eight years, she had felt the same strange itch on her hands and sometimes her feet. Each time it was quickly followed by a terrifying sense of her throat closing.
Anaphylactic Shock
She had driven herself to her sister’s house, several miles away, and her sister drove her the rest of the way to the hospital. She opened the car window to let in the frigid winter night air. She struggled to breathe. Black spots swam before her eyes, but she willed herself not to pass out.
She had had this kind of allergic reaction twice before but never as severely. She knew from her own research that this was anaphylactic shock — a potentially deadly allergic reaction. After she got the medications, the woman’s symptoms resolved. She stayed in the hospital overnight, and when it was clear that the episode was over, she went back to her mother’s house. She made an appointment to see a local allergy specialist right away.
A Mystified Allergist
The specialist spent nearly two hours going over everything the woman had been exposed to — food, plants, toxins, anything that might have triggered this nearly fatal allergic reaction. There were no new exposures that day, nothing she hadn’t eaten or touched many times before and after this latest attack. The most common cause of severe allergic reactions in adults is food, but the allergist couldn’t identify any likely suspects. He was mystified. He asked her to share her diagnosis when she got one.
For months after returning to her home on Long Island, the woman was anxious about everything she ate, and she worried every night when she went to bed. She always kept a bottle of Benadryl and an EpiPen with her, but still she was terrified about what might happen if she was too far from a hospital the next time.
‘I Need a Nurse!’
When her next attack happened — just 10 months later — she was already in Brookhaven Memorial Hospital in East Patchogue, N.Y. She was being treated with antibiotics for a devastating case of gastroenteritis due to salmonella. Her first meal, after days of nothing but clear liquids, was beef brisket with potatoes and carrots. It smelled good, but she had no appetite. She made herself eat a few bites anyway, knowing it was her first step toward going home.
A couple of hours later, she felt a strange itch on the top of her head. She scratched reflexively. Then the recognition hit her like a slap: Not now, she thought. She grabbed the IV pole, still dripping fluids into her system, and ran out into the hallway. “I need a nurse,” she shouted. Her heart was pounding, and she knew what was coming next. Hospital staffers in scrubs descended on her. Was she having a panic attack? No, an allergy attack, she told them.
They helped her back into bed and gave her oxygen, Benadryl and steroids. “What happened?” someone asked. She told the whole story, plus something she now realized — every one of her attacks seemed to come a few hours after she ate beef. She didn’t go through this every time she had a hamburger or steak; meat was a regular and much-loved part of her diet. But she was pretty sure that she had steak — or beef brisket, this time — before each episode.
Her doctors were dubious. New food allergies — especially severe ones like hers — are uncommon in adults. This was much more likely to be an allergic response to one of the antibiotics they were giving her. The patient, though, found that theory hard to swallow. It might explain this episode, but what about the earlier ones? She hadn’t been on antibiotics then. The doctors had no answer.
Was a Tick to Blame?
A nurse had a different theory about what happened, one the patient had heard before but never believed. There was some kind of tick, the nurse told her, whose bite could make you allergic to meat. She didn’t know much about it. But, the nurse suggested, she should check it out.
The woman had been bitten by ticks before — who on Long Island hasn’t? But was it really possible for a bite to produce this crazy reaction? Indeed it was, she discovered, when she got home and began doing some research. The bite of the lone star tick — named for a white spot shaped like Texas on the arachnid’s back — could cause an allergic reaction to mammalian meat. The trigger was a sugar, identified as galactose-α-1,3-galactose and more casually known as alpha-gal, a carbohydrate found in the flesh of all nonprimate mammals.
How the tick bite triggers this allergy is not yet known. The link between the tick — whose range extends from southern Florida to Maine and as far west as Iowa — and the resulting alpha-gal allergy was first described in 2009 by Thomas Platts-Mills, a professor at the University of Virginia, who himself developed the disorder. Unlike most food allergies, in which symptoms occur within minutes of consuming the allergen, the alpha-gal reaction is delayed. The symptoms — ranging from a rash to nausea to shortness of breath and even anaphylaxis — can appear four to six hours after a meal containing meat. Stranger still, the reaction doesn’t occur after every exposure.
A Diet Changed Forever
The diagnosis of mammalian meat allergy (M.M.A.) can be confirmed with a blood test that identifies antibodies to alpha-gal. The patient contacted Diane Cymerman, an allergist she had seen years earlier for seasonal allergies. Cymerman asked her to list all the foods she consumed before her last episode in the hospital and had her blood tested for antibodies to everything on the list, down to the black pepper and parsley seasoning. And to alpha-gal.
The first results came back the following week: She had a moderate allergy to beef, but everything else was normal. The following month, the test results for alpha-gal antibodies came back. She was wildly allergic to galactose-α-1,3-galactose. Cymerman called the patient with the news. She had to avoid eating meat from mammals — and everything derived from them, including Jell-O and other foods and medications made from gelatin. Even safe foods cooked on a grill that has also been used for meat can be contaminated with enough alpha-gal to trigger a reaction.
The patient contacted the allergist back in Iowa and told him what she had. He was amazed. He had only recently heard a lecture on this phenomenon. He had never seen it before her case.
It hasn’t been easy for this Iowa transplant to give up beef and other meat that comes from mammals. Some days, she tells me, just thinking about a juicy hamburger or steak makes her stomach growl. But she remembers her terror and that long drive to the Iowa hospital and sticks to chicken, fish and vegetables.
Lisa Sanders, M.D., is a contributing writer for the magazine and the author of “Every Patient Tells a Story: Medical Mysteries and the Art of Diagnosis.” If you have a solved case to share with Dr. Sanders, write her at Lisa.Sandersmd@gmail.com.
Great video by Dr. Greger at nutritionfacts.org on tick bites, meat allergies, and chronic urticaria
https://madisonarealymesupportgroup.com/2016/02/05/paralysis-tick-the-immune-system/ Australian allergy specialist Sheryl van Nunen got her red meat allergy mystery solved when there was a surge in allergic reactions in the U.S. to a drug, Cetuximab, used to treat colorectal cancer developed using a mouse cell line, also containing alpha-gal.
Epstein-Barr Virus: A Key Player in Chronic Illness
by Dr. Bill Rawls
Posted 11/3/17
So, you’re experiencing symptoms of tiredness, achiness, sore throat, and possibly swollen lymph nodes and low-grade fever that just won’t go away.
You’ve Googled your symptoms, and mononucleosis pops up as a likely possibility. But if you’re well beyond college age, mononucleosis isn’t very common.
Chronic fatigue syndrome, fibromyalgia, and even Lyme disease are other possibilities you might have entertained, especially if you have symptoms beyond those mentioned above. But then you came across something called reactivated Epstein-Barr virus, which fits your symptoms to a tee.
If you are aware that Epstein-Barr virus (EBV) is the cause of mononucleosis, you may be wondering: What’s the difference between chronic reactivated EBV and mononucleosis? And beyond that, what makes chronic reactivated EBV chronic — and how does it play into other chronic illnesses?
To find out, read on to learn more about this complex and convoluted microbe called Epstein-Barr virus and what can make it a long-term troublemaker.
Almost Everyone Has EBV
Let’s start with the fact that EBV is much more common than you might imagine: >95% of world’s population has been infected with it.
Another interesting fact is that it’s a herpes-type virus. Yep, you read that right: EBV is a close relative of genital herpes. Known technically as Human Herpesvirus 4 (HHV-4), it’s #4 on the list of nine different herpes-type viruses that can infect humans.
Herpesviruses are composed of strands of DNA inside an envelope. After initial infection, they stay dormant in tissues indefinitely, but can reactivate if immune system functions become depressed.
In other words, if you’ve ever been infected with a herpesvirus like EBV, you will always carry it in your tissues.
EBV Can Spread Like Wildfire
The majority of people become infected with EBV as infants or young children. The virus spreads primarily by oral route via saliva. To enter the body, it infects mucous membranes lining the mouth, throat, and stomach. From there, the virus infects B cells, the type of white blood cell that produces antibodies. It also infects T cells and natural killer cells, but to a lesser extent. Infected white blood cells transport EBV throughout the body.
In this active phase, called the lytic phase, the virus takes over the machinery of infected cells to generate new viruses. This is when people are most symptomatic and contagious.
The virus spreads remarkably easily, especially in children. It is most typically spread by people who are infectious, but don’t know it — daycare workers, babysitters, grandmothers with big wet kisses. Following that, infected children rapidly pass it along to other children.
Which is a really good thing — because if you get it as an infant or young child (remember to thank your grandmother), you typically don’t get very sick at all. In fact, it’s unlikely that you would even remember the infection.
It’s only if you don’t get EBV at a young age and then get exposed later in life when your immune system is suppressed that you’re at risk for developing the form of EBV called mononucleosis.
Known as kissing disease, infectious mononucleosis (IM) is spread by intimate contact with someone shedding the virus. It typically occurs in young adults who haven’t been exposed early in life. It usually catches the person off guard when immune system functions are depressed, such as during the stress of high school or college.
Compared to EBV occurring in childhood, IM is much more severe: Common symptoms include sore throat, fever, severe fatigue, and swollen lymph nodes. It can drag on for months and be quite debilitating.25
Whether the initial encounter with EBV occurs as an innocuous infection as a child or as debilitating mononucleosis as a young adult, the host’s immune system eventually gains ground and the infection is contained.
The virus, however, is not eradicated. It persists inside memory B cells, a type of white blood cell that retains “memory” of an infection for future reference — except in this case, the cells are sabotaged into storing the actual virus. Memory B cells infected with EBV accumulate in lymphoid tissue and nerve tissue, and stay there for a lifetime.
This dormant state is referred to as the latent phase.9, 6, 12, 23Traditionally, people in the latent phase weren’t considered noninfectious. But with all the daycare workers, teachers, grandmas, and college students actively shedding the virus without knowing it, it’s become clear that someone can be very infectious without being ill. In fact, recent evidence supports that people often actively shed virus from tonsillar tissues without having significant symptoms.23
Either way, whether EBV is completely dormant or infectious without symptoms, the virus generally doesn’t cause any significant problems as long as immune system functions are robust. You can carry it for a whole lifetime and not know it — as most people do.
However, allow the immune system to become disrupted — by stress, poor diet, and other key factors I’ll explore below — and EBV can reactivate, causing symptoms similar to the mononucleosis, but much worse.4
Reactivated EBV Can Become Chronic
Chronic reactivated EBV is like mononucleosis from hell.
Symptoms of reactivated EBV include severe chronic fatigue, chronic achiness, chronic sore throat and irritation of mucous membranes, swollen lymph nodes, and a range of debilitating neurological symptoms. Symptoms can wax and wane for years. Severe cases can include evidence of liver dysfunction, immune suppression, and anemia.1
The most plausible explanation for why chronic reactivated EBV is so severe and unrelenting is that it’s not just EBV that’s at play.
This is where things get both interesting and complicated.
People often carry other herpesviruses in addition to EBV. The list includes Herpes simplex types 1 and 2 (oral and genital herpes), varicella-zoster virus (causing both chickenpox and shingles), cytomegalovirus (CMV), HHV-6 types a and b, HHV-7, and HHV-8.
Though they are all related, each of these viruses infects the body in a different way — therefore they cause slightly different symptom profiles. In important ways, they are all are remarkably common:
They stay dormant in tissues and can be reactivated just like EBV.
If disruption of a person’s immune functions allows reactivation of multiple herpesviruses at once, symptoms can be severe and highly variable.
But that isn’t the end of the story.
Many people with chronic Lyme disease, fibromyalgia, and chronic fatigue syndrome are found to have reactivation of EBV, along with other herpesviruses and a list of other microbes including Mycoplasma, Bartonella, Chlamydia, and new microbes added to the list every day.
This strongly suggests that reactivation of EBV is likely not EBV alone.
The Connections Between EBV and Chronic Illnesses Are Many
Scientists are just beginning to explore the link between chronic EBV and other chronic illnesses, but one of the most well-researched is EBV’s relationship with multiple sclerosis (MS). Many studies have defined a variety of different mechanisms by which the virus could initiate and perpetuate MS — not enough to define EBV as the sole cause of MS, but highly suggestive that it does play a role in the illness.10
Similarly, studies have shown high viral loads of active EBV in a high proportion of patients with a variety of autoimmune diseases, including rheumatoid arthritis, systemic lupus erythematosus, Sjögren’s syndrome, and autoimmune thyroiditis.14 Again, a strong link, but not enough to suggest absolute cause of EBV alone.
And that’s not the end of the multi-microbe connections.
Recent evidence has suggested that EBV and HHV-6a might together play a role in MS.29 MS has also been linked to a variety of different microbes including, but not limited to, Chlamydia pneumoniae,35, 37 Mycoplasma sp., Spherula insularis, and paramyxovirus.14, 36
Autoimmune diseases have also been linked to a variety of microbes, including EBV, but also additional herpesviruses; other viruses including Parvovirus; a protozoan called Toxoplasmosis; and bacteria including Mycoplasma, Yersinia, and others commonly associated with chronic Lyme disease.14
Often referred to as stealth pathogens, the microbes mentioned and many others share similar stealthy characteristics:
They have the ability to live inside cells.
They infect white blood cells and are carried throughout the body, especially to areas of inflammation.
They can persist in a dormant state.
They are master manipulators of the immune system.
They can exist in healthy people without causing illness.
They are present in all populations of the world.
The deeper you dig, the more connections you find between chronic illnesses and stealth microbes. But after a while, you begin to appreciate that it’s not as much the microbes causing problems as it is disruption of the host’s immune functions that allows those microbes to flourish.
In other words, a person could be harboring a variety of stealth microbes — EBV, CMV, HHV-7, Borrelia, Bartonella, Mycoplasma, Chlamydia, and others — and not be ill as long as their immune system functions are robust.
Let immune system functions falter, however, and like a pot boiling over on the stove, the microbes erupt and cause illness.
Chronic Immune Dysfunction Is Triggered by the Perfect Storm
My experience taught me that the microbes are always there — I had likely harbored mine since childhood. It’s not until a perfect storm of factors comes together to disrupt immune functions that a person becomes ill. For me, that perfect storm was caused primarily by years of chronic sleep deprivation associated with every-other-night obstetrics on-call-duty and eating a poor diet on the run, but there were other minor stress factors as well.
As I shifted my practice toward caring for individuals with chronic illness, I began to see similar patterns in my patients — not necessarily the same stress factors that I had experienced, but stress factors that disrupt immune functions just the same. I began cataloging them and, interestingly, I reached a limit of just 7 categories of stress factors that are associated with chronic illness.
As astounding as it may sound, I came to the conclusion that the causes of all chronic illnesses can be traced back to these 7 factors that I came to call System Disruptors. I’ve been testing this theory for more than 10 years and always find it to be reliable. I’ve also discovered solid scientific support for my theory.
The 7 System Disruptors are:
1. Poor diet. We live in a world saturated with artificially manipulated foods. Regular consumption of these foods disrupts all systems of the body.
2. Toxins. The modern world is saturated with artificial toxins. Toxins disrupt all healing systems of the body.
3. Emotional stress. Continually running from the proverbial tiger inhibits digestion, suppresses immune function, disrupts sleep, and sets the stage for chronic illness.
4. Physical stress. Cumulative trauma, excessive heat or cold causes damage to the body, but living a sedentary life can be just as harmful.
5. Oxidative stress. Every cell in the body is continually generating free radicals as a byproduct of energy production. Free radicals damage internal components of cells. Inflammation is also a type of free radical damage.
6. Artificial radiation. Normal background radiation from the sun, solar system, and the earth itself are now amplified sources of radiation that saturate the modern world.
7. Microbes. The effects from this system disruptor set the stage for chronic illness.
For every patient with chronic illness, I can always trace back to a perfect storm of factors that came together to cause the person’s illness. What type of chronic illness they ended up with depends on three factors:
The person’s genetics — which determines risk, but not whether an illness will occur
The variety of different low-grade stealth pathogens the person has collected through life
How System Disruptors contribute to immune dysfunction, which allows low grade pathogens with stealthy characteristics to flourish and upset the balance of the microbiome and homeostasis in the body
Diagnosing and Treating Chronic EBV Isn’t Black and White
To help identify chronic EBV, start by trying to rule out infectious mononucleosis. By definition, IM is an acute infection with EBV alone, and there are antiviral agents (such as acyclovir, ganciclovir, and vidarabine) that work extremely well for IM and other acute infections of herpes-type viruses, so it’s worth doing testing to define IM over reactivated EBV.
Testing for IM looks for antibodies to the virus; the presence of different types of antibodies can distinguish between IM and reactivated EBV. But testing for IM isn’t always straight-forward — mononucleosis-like syndromes can also occur with other herpesviruses (CMV, HHV-6), other viruses (typically adenoviruses), and a protozoan called Toxoplasma gondii.26 In other words, many different viruses can cause viral syndromes similar to EBV.
If you have all the symptoms of chronic reactivated EBV, then the likelihood of EBV being present is quite high, along with other microbes.
As for treating chronic reactivated EBV, because there are antiviral agents that work well for IM, you might expect that chronic EBV would also respond to antivirals.
Unfortunately, antivirals don’t work for chronic EBV.
Scientists have sorted out the technical reason for this. Antiviral agents work by blocking DNA polymerase, an enzyme the virus uses to replicate inside cells. Latent or chronic EBV infection, however, does not require DNA polymerase for the virus to replicate — therefore, current antiviral agents are ineffective against chronic EBV infection.1
Other conventional therapies, including steroid therapy (prednisone) and immunosuppressive drugs, have been used to treat chronic EBV infection, but success has been limited.1These therapies can inhibit the destructive processes of a disrupted immune function, but they have no capacity to restore normal immune function.
Lots of researchers are also looking at vaccines against EBV. The problem is that characteristics of the virus vary greatly across different geographical areas, making it difficult to create a single vaccine.8
Other methods of eradicating EBV being contemplated by conventional medical science include: B-cell depletion with monoclonal antibodies (targeting EBV-infected B cells with immunoglobulins) and new types of antiviral drugs.11, 16, 20
Focusing all efforts on eradicating EBV, however, is short-sighted. The bottom line: The underlying problem is chronic immune dysfunction, and you will not start getting well until normal immune system functions are restored.
There’s A More Practical Approach to Regaining Wellness
Remember, EBV doesn’t cause problems unless immune system functions have been disrupted.1, 14, 20, 23 Therefore, any solution must address restoring normal immune system functions in order to suppress whatever microbes may be present and flourishing.
First and foremost is minimizing the 7 System Disruptors. Following an optimal diet and making some lifestyle modifications to promote a healing environment in the body is essential for overcoming chronic EBV or any other chronic illness.
Modern herbal therapy should be the cornerstone of any restorative approach. Herbal extracts have incredible abilities, including:
Reducing destructive inflammation
Enhancing natural killer cells and other aspects of the immune system necessary to control microbes like EBV
Balancing hormone systems in the body that have been disrupted by chronic illness
Suppressing stealth microbes directly to restore balance in the microbiome
While many herbs have been found to suppress EBV, EBV is rarely found in isolation — chronic immune dysfunction always allows a variety of low-grade stealth pathogens to flourish. Therefore, a comprehensive regimen of herbal extracts is necessary.
Some effective herbal extracts for restoring immune function, balancing the microbiome, and suppressing viruses such as EBV include:
Generally most people will respond to restorative solutions alone. Drug therapy is only necessary if severe or extreme illness is not responding to the restorative therapies. It is, however, important to maintain an ongoing working relationship with your medical provider during your entire recovery.
Ultimately, all of this is great news for those with chronic reactivated EBV: It means the power to take back control of your health and feel better is in your hands. By learning how to limit the System Disruptors in your life, you’ll start to strengthen your immune function so you can live in harmony with microbes like EBV.
The Sleeping Giant – Tips to Treat Reactivation of Epstein-Barr Virus
Jill C. Carnahan, MD
Did you know, you probably have virus lurking in the shadows? It’s called the Epstein-Barr virus (EBV) and an estimated 90 percent of us have it. Fortunately, for most of us it lies dormant, like a sleeping giant. Only when something triggers a reactivation of EBV does this virus rear its ugly head.
Epstein-Barr virus is part of the herpes family and also known as human herpesvirus 4. Usually passed through saliva, EBV is the cause of infectious mononucleosis – also known as “mono” or “kissing disease.” Typically, teenagers come down with this condition and first notice there’s a problem when they experience extreme fatigue. Interestingly, extreme fatigue can also cause a reactivation of Epstein-Barr virus.
Though there are many conditions where EBV is the cause or a trigger, extreme fatigue is a unifying symptom that occurs in most cases. Symptoms of an active Epstein-Barr virus, include:
Autoimmune conditions are caused when an overactive immune system begins attacking healthy tissue. We are learning more and more, what often sets off the immune system response in the first place can be a variety of infections, including EBV.
CD8+T cells are types of white blood cells your body uses to keep the EBV virus in check. When there’s an impairment or a deficiency of these cells, the EBV virus is free to run rampant. The amount of CD8+T cells you have can be negatively impacted by age, estrogen levels, and vitamin D deficiency, certain medications and treatments, and poor immune system function. This is important because autoimmunity is on the rise and we need a better understanding of its underlying causes.
So, what can be done to treat Epstein-Barr? If it’s so common, surely there’s a simple explanation or cure? Actually, the best way to tackle Epstein-Barr is similar to how we deal with an imbalance of gut microbes – manipulate the environment so balance is restored. The most important thing I find is to support the natural immunity and decrease exposures to environmental toxins and other infections. Let’s take a closer look.
Treating the Epstein Barr Virus
There is no known cure for the Epstein-Barr virus, and therefore treatments should focus on returning the creature back to it’s sleeping or dormant state. So, in order to treat EBV the approach needs to focus on getting the virus back in check, not killing it. This means manipulating the condition of your body – the environment where the Epstein-Barr virus lives.
When I discover a patient of mine has Epstein-Barr virus, here are the things I consider:
Clean diet and proper nutrition – This reduces inflammation and immune system burden. We eliminate gluten, dairy, allergens, and start a plant-based Paleo diet. Sugar is one of the most powerful immunosuppressives so that must be eliminated at all costs.
Heal the gut – Healing the gut is a priority for anyone dealing with EBV. Toxins can leak through damaged gastrointestinal lining and cause the immune system to overreact. This process is also known as endotoxemia, driven by LPS.
Eliminate any infections – Check for any coexisting infections and work to treat these. I often think of it as “infectious burden” and work to decrease the load on the immune system.
Reduce toxic burden – We are bombarded by tens of thousands of chemicals everyday, find out how to Reduce Your Daily Toxin Exposure. It is critical also to decrease total toxic load by eliminating any toxic exposures.
Optimize detox pathways – This includes supporting the liver, kidneys, and colon and may be supported by various nutritional supplements and other homeopathic drainage remedies.
Improving sleep habits – This is essential because so many repairing and detoxification processes occur during the deepest stages of sleep. I advise no less than 8 hours per night or as much sleep as required to wake up refreshed without an alarm clock.
Reduce stress – Stress is a major cause of immune system dysfunction, it could even be what awakened your EBV in the first place. You must work to reduce stress – your health depends on it. Try prayer, meditation or spending time in nature. Self care must be a priority.
Herbal supplements – Herbs such as Ashwagandha, licorice, St. John’s wort, lemon balm, ginseng, and holy basil may be used for immune system support and for their antiviral and adaptogenic properties.
Supplements – I use these for suppressing EBV reactivation
Monolauren: 1800 mg twice daily
Olive Leaf: 1000-1500 mg twice daily
L-Lysine: 1000-1500 mg twice daily
Cat’s Claw tincture: 30-60 drops twice daily
When viruses diminish due to these treatments it isn’t because any of these things attack the virus, but instead they help put your body in a state that isn’t ideal for the virus to reproduce. Hopefully, this strengthens your immune system and returns this typically harmless virus back to it’s benign state.
Other more extreme therapies have have been tried in a few cases, with some success and include:
Antiviral medication, Acyclovir or valcyclovir
Immune cell therapy when used in a person after a transplant.
Bone marrow transplant is an extreme therapy that has been documented in two life threatening cases.
Though I prefer to offer solutions to health conditions, I want to briefly touch on some treatments of EBV are not effective because there’s a lot of misunderstanding surrounding this virus. In general, the follow treatments only temporarily stop symptoms and only in some people:
Antiviral therapy such as ganciclovir and vidarabine.
Immunosuppressive agents such as cyclosporine and corticosteroids.
Immunomodulatory therapy such as interferon alpha and interferon gamma.
Cytotoxic chemotherapy such as anthracyclines, etoposide, cyclophosphamide, vincristine, and prednisone.
Infusions of cytotoxic T and lymphokine-activated lymphocytes.
This isn’t to suggest that your doctor shouldn’t temporarily recommend some of these, however, none of these are by any means a cure for Epstein-Barr virus and you should proceed with extreme caution.
Find a Functional Medicine Doctor with Experience in Epstein-Barr Treatments
The science surrounding the Epstein-Barr virus is developing daily. If you think you might have a condition due to EBV, it’s important to find a doctor who’s experienced in conditions related to the reactivation of this virus. If you need help finding a functional medicine doctor, I’ve made a helpful guide to get you started – How to Choose a Good Integrative and Functional Medicine Doctor.
The Epstein-Barr virus is a significant condition I wish more people knew about – Share this article to spread awareness of this sleeping giant.
Being in Wisconsin, an epicenter for Lyme, our LLMD is also who we take our children to – just in case, God forbid, they should become infected. Our LLMD believes, as Dr. Rawls, that immunoconfusion, or a perfect storm of events overwhelming the immune system, is behind many chronic diseases. Retraining the immune system to recognize friend vs foe is behind LDA/LDI treatment and can often help many chronic conditions. It certainly has helped my daughter, who is also hypothyroid, hypoglycemic, and suffers from severe endometriosis. EBV nearly destroyed her liver.
I can attest to having to learn the importance of diet, hormones, stress, environmental toxins, and microbes. It is crucial to find a practitioner(s) who is versed in this approach to tease out your imbalances through proper testing and clinical diagnosis. As with Lyme, much testing isn’t helpful and requires an experienced eye and listening ear to help you uncover your personal pitfalls. Most doctors are not trained in hormone therapy and with the chemically laden environment we live in, this is most unfortunate as many suffer from serious hormonal imbalances and mineral/vitamin deficiencies. Doctors are taught to fear hormones when they are naturally occurring substances in the body that often need supplementing due to environmental factors. I’m of course advocating for bioidential hormones – as close to nature as possible; however, for those of you suffering with endometriosis that makes your life unbearable, please read this unique approach which gave my daughter her life back: https://www.theendocure.com/
REFERENCES For Dr. Rawl’s article:
1. Cohen J. Optimal Treatment for Chronic Active Epstein-Barr Virus Disease. Pediatr Transplant. 2009 Jun; 13(4): 393–396.
2. Joo E et al. An Adult Case of Chronic Active Epstein-Barr Virus Infection with Interstitial Pneumonitis. Korean J Intern Med. 2011 Dec; 26(4): 466–469.
3. Kang M, Kief E. Epstein–Barr virus latent genes. Exp Mol Med. 2015 Jan; 47(1): e131.
4. Jha H, Pei Y, Robertson E. Epstein–Barr Virus: Diseases Linked to Infection and Transformation. Front Microbiol. 2016; 7: 1602.
5. Tsao S et al. The role of Epstein–Barr virus in epithelial malignancies. J Pathol. 2015 Jan; 235(2): 323–333.
6. Paschale M and Clerici P. Serological diagnosis of Epstein-Barr virus infection: Problems and solutions. World J Virol. 2012 Feb 12; 1(1): 31–43.
7. Shen Y et al. Understanding the interplay between host immunity and Epstein-Barr virus in NPC patients. Emerg Microbes Infect. 2015 Mar; 4(3): e20.
8. Tzellos S and Farrell P. Epstein-Barr Virus Sequence Variation—Biology and Disease. Pathogens. 2012 Dec; 1(2): 156–175.
9. Iizasa H et al. Epstein-Barr Virus (EBV)-associated Gastric Carcinoma. Viruses. 2012 Dec; 4(12): 3420–3439.
10. Lassmann H et al. Epstein–Barr virus in the multiple sclerosis brain: a controversial issue—report on a focused workshop held in the Centre for Brain Research of the Medical University of Vienna, Austria. Brain. 2011 Sep; 134(9): 2772–2786.
11. Pender M and Burrows S. Epstein–Barr virus and multiple sclerosis: potential opportunities for immunotherapy. Clin Transl Immunology. 2014 Oct; 3(10): e27.
12. Stanfield B and Luftig M. Recent advances in understanding Epstein-Barr virus. Version 1. F1000Res. 2017; 6: 386.
13. Gru A et al. The Epstein-Barr Virus (EBV) in T Cell and NK Cell Lymphomas: Time for a Reassessment. Curr Hematol Malig Rep. 2015 Dec; 10(4): 456–467.
14. Lossius A et al. Epstein-Barr Virus in Systemic Lupus Erythematosus, Rheumatoid Arthritis and Multiple Sclerosis—Association and Causation. Viruses. 2012 Dec; 4(12): 3701–3730.
15. Rowe M, Fitzsimmons L, and Bell A. Epstein-Barr virus and Burkitt lymphoma. Chin J Cancer. 2014 Dec; 33(12): 609–619.
16. Martorelli D et al. Exploiting the Interplay between Innate and Adaptive Immunity to Improve Immunotherapeutic Strategies for Epstein-Barr-Virus-Driven Disorders. Clin Dev Immunol. 2012; 2012: 931952.
17. Houldcroft C and Kellam P. Host genetics of Epstein–Barr virus infection, latency and disease. Rev Med Virol. 2015 Mar; 25(2): 71–84.
18. Draborg AH, Duus K, and Houen G. Epstein-Barr Virus in Systemic Autoimmune Diseases. Clin Dev Immunol. 2013; 2013: 535738.
19. Rac J et al. Telomerase Activity Impacts on Epstein-Barr Virus Infection of AGS Cells. PLoS One. 2015; 10(4): e0123645.
20. Pender M. The Essential Role of Epstein-Barr Virus in the Pathogenesis of Multiple Sclerosis. Neuroscientist. 2011 Aug; 17(4): 351–367.
21. Dittfeld A et al. A possible link between the Epstein-Barr virus infection and autoimmune thyroid disorders. Cent Eur J Immunol. 2016; 41(3): 297–301.
22. Chen XZ et al. Epstein–Barr Virus Infection and Gastric Cancer
A Systematic Review. Medicine (Baltimore). 2015 May; 94(20): e792.
23. David A. Thorley-Lawson. EBV Persistence—Introducing the Virus. Curr Top Microbiol Immunol. 2015; 390(Pt 1): 151–209.
24. Iwakiri D. Epstein-Barr Virus-Encoded RNAs: Key Molecules in Viral Pathogenesis. Cancers (Basel). 2014 Sep; 6(3): 1615–1630.
25. Dunmire SK, Hogquist KA, and Balfour HH. Infectious Mononucleosis. Curr Top Microbiol Immunol. 2015; 390: 211–240.
26. Krupka JA et al. Infectious mononucleosis-like syndrome with high lymphocytosis and positive IgM EBV and CMV antibodies in a three-year-old girl. Cent Eur J Immunol. 2017;42(2):210-212.
27. Collin V, Flamand L. HHV-6A/B Integration and the Pathogenesis Associated with the Reactivation of Chromosomally Integrated HHV-6A/B. Viruses. 2017 Jun 26;9(7).
28. Warren-Gash C et al. Association between human herpesvirus infections and dementia or mild cognitive impairment: a systematic review protocol. BMJ Open. 2017 Jun 23;7(6):e016522.
29. Fierz W. Multiple sclerosis: an example of pathogenic viral interaction? Virol J. 2017 Feb 28;14(1):42.
30.Enquist LW, Leib DA. Intrinsic and Innate Defenses of Neurons: Détente with the Herpesviruses. J Virol. 2016 Dec 16;91(1).
31. Hutt-Fletcher LM. The Long and Complicated Relationship between Epstein-Barr Virus and Epithelial Cells. J Virol. 2016 Dec 16;91(1).
32. Siddiquey MN et al. Anti-tumor effects of suberoylanilide hydroxamic acid on Epstein-Barr virus-associated T cell and natural killer cell lymphoma. Cancer Sci. 2014 Jun;105(6):713-22.
33. Cekanaviciute E et al. Gut bacteria from multiple sclerosis patients modulate human T cells and exacerbate symptoms in mouse models. Proc Natl Acad Sci U S A. 2017 Sep 11. pii: 201711235.
34. Berer K et al. Gut microbiota from multiple sclerosis patients enables spontaneous autoimmune encephalomyelitis in mice. Proc Natl Acad Sci U S A. 2017 Sep 11. pii: 201711233.
35. Ivanova MV et al. Role of Chlamydia in Multiple Sclerosis. Bull Exp Biol Med. 2015 Sep;159(5):646-8.
36. Libbey JE, Cusick MF, Fujinami RS. Role of pathogens in multiple sclerosis. Int Rev Immunol. 2014 Jul-Aug;33(4):266-83.
37. Sriram S et al. Detection of chlamydial bodies and antigens in the central nervous system of patients with multiple sclerosis. J Infect Dis. 2005 Oct 1;192(7):1219-28. Epub 2005 Sep 2.
38. Buhner S. Herbal Antivirals, Natural Remedies for Emerging & Resistant Viral Infections. Storey Publishing. Copyright 2013.
Online Ahead of Print: October 24, 2017
Serbia
E-mail: ale@polj.uns.ac.rs
ABSTRACT
Tick-borne encephalitis (TBE) is a zoonotic flaviviral infection that is a growing public health concern in European countries. The aims of this research were to detect and characterize tick-borne encephalitis virus (TBEV) in Ixodes ricinus ticks at presumed natural foci in Serbia, and to determine seroprevalence of TBEV IgG antibodies in humans and animals.
A total of 500 I. ricinus ticks were examined for the presence of TBEV by real-time RT-PCR, and conventional nested PCR and sequencing. To determine TBEV seroprevalence, 267 human sera samples were collected, as were 200 sera samples from different animal species. All sera samples were examined by ELISA for the presence of anti-TBEV antibodies. To exclude cross-reactivity, all sera samples were tested for anti-West Nile virus (WNV) antibodies and all human sera samples were also tested for anti-Usutu virus antibodies by ELISA.
Results of this preliminary study indicated TBEV activity in Serbia at two microfoci. Several decades after the previous documentation of TBEV in Serbia, we have demonstrated the presence of TBEV in I. ricinus questing nymphs (prevalence 2% and 6.6% at the two different localities) and anti-TBEV antibodies in humans (seroprevalence 0.37%). Moreover, we show for the first time TBEV seroprevalence in several animal species in Serbia, including dogs (seroprevalence 17.5%), horses (5%), wild boars (12.5%), cattle (2.5%), and roe deer (2.5%). None of the goats tested was positive for anti-TBEV IgG antibodies. TBEV isolate from I. ricinus tick in this study belonged to the Western European subtype. To understand the true public health concern in Serbia, detailed epidemiological, clinical, virological, and acarological research are required. This is important for implementation of effective control measures to reduce the incidence of TBE in Serbia.
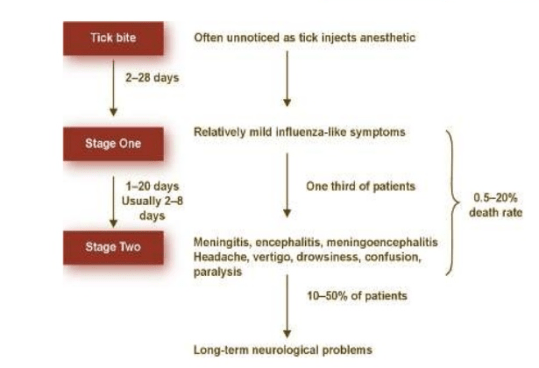
It is only in the second stage of disease that early meningoencephalitis can be detected by laboratory tests(blood, brain and spinal fluid).
https://www.cdc.gov/vhf/tbe/index.html Other Flaviviridae viruses closely related to TBEV: Omsk hemorrhagic fever virus in Siberia, Kyasanur Forest disease virus in India and its close relative, Alkhurma virus in Saudi Arabia, Louping ill virus (United Kingdom) that causes disease primarily in sheep but has been reported as the cause of a TBE-like illness in laboratory workers and persons with contact to sick sheep (e.g., veterinarians, butchers), and Powassan virus in the USA and Russia, is responsible for encephalitis in humans.
https://madisonarealymesupportgroup.com/2017/10/15/vaccines-and-retroviruses-a-whistleblower-reveals-what-the-government-is-hiding/ Since the 1970’s scientists have done disease research in the same labs manufacturing vaccines. They erroneously believed that mouse viruses and human viruses would not interact, or travel from one part of the research facility to another. This belief was proven wrong in 2009 by Dr. Judy Mikovits and other scientists who discovered that a retrovirus called XMRV (xenotropic murine retrovirus) and other related retroviruses were now present in 6% of Americans and that this retrovirus was appearing in a very high percentage of people with diseases such as prostate cancer, Chronic Fatigue Syndrome, autism, Lou Gehrig’s Disease, treatment resistant Lyme disease, and Parkinson’s Disease.
Man dies of Powassan virus and doctors are sounding the alarms to not only Lyme disease, but other tick-borne illnesses. Stefan Holt reports in the final part of News 4’s 5-part series on the Lyme Wars.
______________
**Comment**
Another informative report on the dangers of other TBI’s (tick borne illness) besides Lyme Disease. Please remember that a tick’s gut is a literal garbage can of pathogens that work synergistically to make us extremely sick. This is why throwing doxycycline like napalm doesn’t work for a significant portion of patients and until doctors become educated and admit that Lyme Disease is usually MSIDS(multi systemic infectious disease syndrome) we are doomed as there is often far more than just Lyme (borrelia) at play requiring different medications. The CDC/IDSA unscientific and antiquated guidelines are seriously behind the 8 ball.
Also, please do not be taken in by doctors such as Dr. Wormser, chief of infectious diseases at NY Medical College, who claim this or that disease is “rare.”That type of verbiage has kept thousands from being tested, diagnosed, and treated for decades. I assure you all of this is more common than currently believed and until every TBI is reportable we have no clue about numbers. Reporting criteria also needs to be brought up to speed as a majority of patients don’t meet the current arbitrary standards created by the CDC that follows the controlled narrative.
Bartonella – Dr. Phillips states many doctors completely ignore Bartonella, and while the CDC states there is no convincing evidence that ticks transmit Bartonella, Phillips is not surprised. He says research on Bartonella is where Lyme was 30 years ago. The majority of WI patients I work with have Bart symptoms.
Prior to 2008, anaplasmosis and ehrlichiosis infections were referred to as human granulocytic ehrlichiosis (HGE) and human monocytic ehrlichiosis (HME), respectively.
Since 2008, surveillance for human anaplasmosis and ehrlichiosis are classified as:
– Anaplasmosis caused by the A. phagocytophilum bacteria (transmitted by the blacklegged tick).
– Ehrlichiosis caused by E. chaffeensis, E. ewingii (transmitted by the Amblyomma americanum or lone star tick).
– Anaplasmosis/Ehrlichiosisundetermined(speciesunknown) including the new species E. muris-like (EML).
Increase in probable cases of E. chaffeensis (lone star tick vector not traditionally seen in Wisconsin.)
In 2009, identified a cluster of novel E. muris-like cases.
In 2009, EML was first identified in a cluster of four case-patients from Wisconsin (3) and Minnesota (1). This atypical Ehrlichia had never before been identified in North America.
From 2009-2012, a total of 33 confirmed EML cases have been identified from both states and one case-patient was cultured positive.
It is uncertain how widely spread the E. muris-like infections are in Wisconsin because of the limited testing available.
DPH is currently working with laboratories to bring the 34 multiplex PCR testing on board.
If one thing is clear it’s that none of this is straight forward and simple. Research and testing for all things TBI is abysmal and has been a controlled narrative from the beginning. Until researchers and doctors have an unbiased approach patients are caught in the Lyme Wars.
JENNIFER CRYSTAL ADDRESSES THE COMMON MYTH THAT LYME DISEASE ONLY EXISTS IN NEW ENGLAND.
Last summer, a friend who lives in Oklahoma found a classic bullseye rash on her seven-year-old daughter.
“That’s a spider bite,” a local pediatrician told her. “We don’t have Lyme in Oklahoma.”
The doctor was wrong. Had my friend taken his advice, her daughter would not have been diagnosed in a timely fashion and she would likely have developed symptoms over the next few months or years. She probably would have become severely debilitated, and the infections might have crossed the blood-brain barrier and become chronic.
In other words, the little girl could have wound up like me. For as it turns out, she did not have a spider bite. She had Lyme disease and two co-infections, Babesia and Bartonella.
Now she’s a healthy, happy second grader because a Lyme Literate Medical Doctor (LLMD) was brought in who accurately saw the bullseye rash for what it was. Another pediatrician ordered special tests, and started the child on proper medication for all three infections.Because they were caught early,those infections have now cleared up.
This little girl was lucky, but that’s because her mother was informed about Lyme and knew to persist beyond the “spider bite” diagnosis. But what about all those children whose parents and pediatricians aren’t Lyme literate? Especially those who live outside the so-called endemic areas?
I don’t believe the Oklahoma pediatrician meant harm with his inaccurate diagnosis. His lack of awareness stemmed from a common myth that Lyme only exists in New England, and specifically in the woods. I’ve had people in Massachusetts say to me,
“Oh Lyme—that’s the thing you get when you’re hiking, right?”
Yes and no. Ticks live not only in the woods but also in long grasses, gardens, woodpiles, leaf litter and on lawns. They love any moist, shady area. They feed not just on deer—another common myth—but also on mice, chipmunks, shrews, birds, and other small mammals. Therefore, they travel a lot. People travel, too. Someone from South Carolina might take a vacation in Maine, get bitten by a tick, and later be told by their doctor, “It can’t be Lyme. We don’t have it in the South.” In fact, cases of Lyme disease have been documented across the United States, and throughout the world.
New research published in the Journal of Medical Entomology shows that infected ticks are now in half the counties across the country, a number that has almost doubled since a similar survey was done in 1998. The study notes that over the past two decades, the black-legged tick
“has expanded from its northeastern focus northward into upstate New York, Vermont, New Hampshire, and northern Maine; westward across Pennsylvania, eastern Ohio, and New York; and south—and southwestward into West Virginia, Virginia, and North Carolina.” The study also notes a similar geographic expansion in the North-Central states. “The two previously distinct foci in the Northeast and North-Central states appear to be merging in the Ohio River Valley to form a single contiguous focus.”[1]
Ticks are spreading across the country, bringing not just Lyme but co-infections. These require different treatment and can complicate recovery.
Had my friend’s daughter only been treated for Lyme and not for Babesia and Bartonella, she would still be sick.
Some of these co-infections are specific to states that are nowhere near New England. Bourbon virus, a rare but potentially deadly illness, has been reported in Kansas and Oklahoma. The Heartland virus, spread through the bite of an infected Lone Star tick, has been found in Missouri, Tennessee and Oklahoma. Also transmitted by the Lone Star tick is Southern Tick-Associated Rash Illness (STARI), while dog ticks and Rocky Mountain wood ticks carry Rocky Mountain Spotted Fever.
Tick borne illnesses are rampant not just in New England, not just deep in the woods, but all across the country and world. As the International Lyme and Associated Diseases Society states on its website,
“ticks know no borders and respect no boundaries.”[2]
No matter where you live, if you have symptoms of Lyme and/or co-infections, it’s critical to see an LLMD. If you still have the tick, you can also get that tested. Follow the smart lead of my friend in Oklahoma, so you don’t wind up like me.
Opinions expressed by contributors are their own.
Jennifer Crystal is a writer and educator in Boston. She is working on a memoir about her journey with chronic tick-borne illness. Contact her at jennifercrystalwriter@gmail.com
[1] Rebecca J. Eisen, Lars Eisen, Charles B. Beard; County-Scale Distribution of Ixodes scapularisand Ixodes pacificus (Acari: Ixodidae) in the Continental United States , Journal of Medical Entomology, Volume 53, Issue 2, 1 March 2016, Pages 349–386, https://doi.org/10.1093/jme/tjv237
Lyme/MSIDS is everywhere. Do not let anyone tell you otherwise. The entomology maps of tick locations have been used for decades keeping patients undiagnosed and untreated. For a great article on how the Spielman maps have been an iron curtain keeping patients from getting tested:https://doczz.net/doc/4593057/the-confounding-debate-over-lyme-disease-in-the-south (scroll to page 6 & 7 for details)
As to testing, the current CDC two-tiered testing misses over half of all cases. The “special” tests Ms. Crystal mentions are more sensitive but are not supported by main stream medicine for reasons I won’t delve into here (essentially governmental collusion, patents, power and money – read article about the CDC needing a good dictionary above).
Lyme literate doctors (LLMD’s) use the more sensitive testing but also diagnose patients clinically as some NEVER test positive. This is important to know. Here is a common checklist you can print out and complete on your own. https://madisonarealymesupportgroup.com/wp-content/uploads/2016/01/symptomlist.pdf If you have a preponderance of symptoms – think TBI’s (tick borne illness); however, there is a caveat – some people present differently and don’t fit the classic mold. For instance, for some, the only significant symptom is psychiatric:
https://madisonarealymesupportgroup.com/2017/10/24/the-lyme-wars-faces-of-the-health-crisis-a-digital-documentary/Kyra, didn’t have the normally thought of symptoms – just horrible anxiety, depression, and hopelessness. Her doctor knows Lyme is the great imitator and suspected it despite a negative test. She tested positive for Ehrlichia, which implies contact with a tick. Due to the Lyme/MSIDS diagnosis Kyra went from blaming herself to understanding she now had something she could fight. After doxycycline they chose IV Rocephin – and Kyra became herself again. “The feeling of actually starting to recognize pieces of what I was before was such an amazing feeling.”


 Another interesting fact is that it’s a herpes-type virus. Yep, you read that right: EBV is a close relative of genital herpes. Known technically as Human Herpesvirus 4 (HHV-4), it’s #4 on the list of nine different herpes-type viruses that can infect humans.
Another interesting fact is that it’s a herpes-type virus. Yep, you read that right: EBV is a close relative of genital herpes. Known technically as Human Herpesvirus 4 (HHV-4), it’s #4 on the list of nine different herpes-type viruses that can infect humans. Known as kissing disease, infectious mononucleosis (IM) is spread by intimate contact with someone shedding the virus. It typically occurs in young adults who haven’t been exposed early in life. It usually catches the person off guard when immune system functions are depressed, such as during the stress of high school or college.
Known as kissing disease, infectious mononucleosis (IM) is spread by intimate contact with someone shedding the virus. It typically occurs in young adults who haven’t been exposed early in life. It usually catches the person off guard when immune system functions are depressed, such as during the stress of high school or college. Symptoms of reactivated EBV include severe chronic fatigue, chronic achiness, chronic sore throat and irritation of mucous membranes, swollen lymph nodes, and a range of debilitating neurological symptoms. Symptoms can wax and wane for years. Severe cases can include evidence of liver dysfunction, immune suppression, and anemia.1
Symptoms of reactivated EBV include severe chronic fatigue, chronic achiness, chronic sore throat and irritation of mucous membranes, swollen lymph nodes, and a range of debilitating neurological symptoms. Symptoms can wax and wane for years. Severe cases can include evidence of liver dysfunction, immune suppression, and anemia.1 First and foremost is minimizing the 7 System Disruptors. Following an optimal diet and making some lifestyle modifications to promote a healing environment in the body is essential for overcoming chronic EBV or any other chronic illness.
First and foremost is minimizing the 7 System Disruptors. Following an optimal diet and making some lifestyle modifications to promote a healing environment in the body is essential for overcoming chronic EBV or any other chronic illness.