
Study Shows 630% More Aerosolized Flu Virus Particles Emitted by Flu-Vaccinated – A Message to Ethical MD’s
http://www.pnas.org/content/115/5/1081
-
Edited by Peter Palese, Icahn School of Medicine at Mount Sinai, New York, NY, and approved December 15, 2017 (received for review September 19, 2017)
Significance
Lack of human data on influenza virus aerosol shedding fuels debate over the importance of airborne transmission. We provide overwhelming evidence that humans generate infectious aerosols and quantitative data to improve mathematical models of transmission and public health interventions. We show that sneezing is rare and not important for—and that coughing is not required for—influenza virus aerosolization. Our findings, that upper and lower airway infection are independent and that fine-particle exhaled aerosols reflect infection in the lung, opened a pathway for a deeper understanding of the human biology of influenza infection and transmission. Our observation of an association between repeated vaccination and increased viral aerosol generation demonstrated the power of our method, but needs confirmation.
Abstract
Little is known about the amount and infectiousness of influenza virus shed into exhaled breath. This contributes to uncertainty about the importance of airborne influenza transmission. We screened 355 symptomatic volunteers with acute respiratory illness and report 142 cases with confirmed influenza infection who provided 218 paired nasopharyngeal (NP) and 30-minute breath samples (coarse >5-µm and fine ≤5-µm fractions) on days 1–3 after symptom onset. We assessed viral RNA copy number for all samples and cultured NP swabs and fine aerosols. We recovered infectious virus from 52 (39%) of the fine aerosols and 150 (89%) of the NP swabs with valid cultures. The geometric mean RNA copy numbers were 3.8 × 104/30-minutes fine-, 1.2 × 104/30-minutes coarse-aerosol sample, and 8.2 × 108 per NP swab. Fine- and coarse-aerosol viral RNA were positively associated with body mass index and number of coughs and negatively associated with increasing days since symptom onset in adjusted models. Fine-aerosol viral RNA was also positively associated with having influenza vaccination for both the current and prior season. NP swab viral RNA was positively associated with upper respiratory symptoms and negatively associated with age but was not significantly associated with fine- or coarse-aerosol viral RNA or their predictors. Sneezing was rare, and sneezing and coughing were not necessary for infectious aerosol generation. Our observations suggest that influenza infection in the upper and lower airways are compartmentalized and independent.
The association of current and prior year vaccination with increased shedding of influenza A might lead one to speculate that certain types of prior immunity promote lung inflammation, airway closure, and aerosol generation. This first observation of the phenomenon needs confirmation. If confirmed, this observation, together with recent literature suggesting reduced protection with annual vaccination, would have implications for influenza vaccination recommendations and policies.
___________
https://jameslyonsweiler.com/2018/02/02/a-message-to-ethical-mds-the-problem-with-the-2017-8-flu-vaccine-is-the-2016-7-flu-vaccine/ (Please read entire article here by James Lyons Weiler)
Letter to ethical MD’s (snippets below):
The last time the flu vaccine was 60-70% effective was eight years ago.
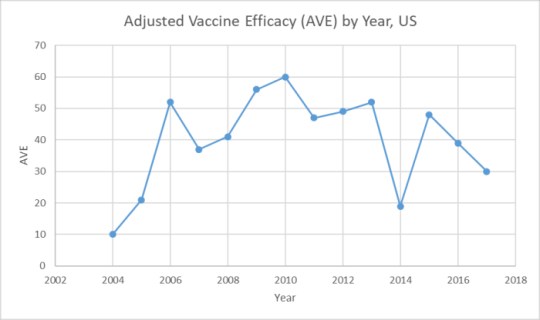
“This is the CDC’s data https://www.cdc.gov/flu/professionals/vaccination/effectiveness-studies.htm Clearly, Gupta’s “Years” is, in immunological memory, a singular “Year”. Only once out of the last 14 years was the flu vaccine above 59% – that the value was not 60-70%, it was 60%.
This type of misrepresentation is a consistent penchant within the media and of course from the CDC to exaggerate and highly emphasize only positive views and diminish, dismiss, or ignore any negative views on the safety and efficacy of vaccines.
The Jury is In: The Flu Vaccine Reduces its Own Efficacy
Too many studies now exist that have independently come to the same conclusion: increases in the uptake of flu vaccine reduces that vaccine’s effectiveness in the following year – and some studies show the negative effects of mass influenza vaccination last two years.
The studies reporting those results are reviewed in my article, “Diseases with Unknown Etiology Trace Back to Mass Vaccination Against Influenza in 1976“, and they are extensive and damning. https://jameslyonsweiler.com/2018/01/31/diseases-with-unknown-etiology-trace-back-to-mass-vaccination-against-influenza-in-1976/
Patients have a right to know the specific nature of their infections, and survivors in families of those who die from respiratory infections deserve an accurate cause of death. Coroners should certainly be required to provide an accurate cause of death in so-called “flu” mortalities. Health departments should be required to count only deaths due to confirmed influenza infection as “flu” – otherwise their numbers perpetuate misperception on the risk of influenza infection, and cause fear leading to increased vaccination. How is this seen as a good thing? The population deserves good and honest doctors and stewards of public health.
HHS could demand swab results for all suspected cases of “flu deaths” with a press release and enforce them with random audits. This annual ritual of fear-mongering over “flu-deaths” hides the fact that as long as thimerosal is injected into patients, they are at increased risk of other infections. And due to heterologous immunity, even without thimerosal, flu vaccines can confuse the immune system and muddle up ineffective immune response by trying to re-purpose B-cells trained on the wrong virus, hobbling the immune system making it unresponsive to similar viruses. Such as next year’s flu strain.
We do need objectivity to arise immediately throughout the public health system in the US, starting with HHS, then to CDC and to all Health Departments around the country. Many studies have also found problems with Tamiflu. But no emergency epidemiological study is addressing the question – why are so many young people dying from “flu”? Many of the reports I’ve seen include mention that they person had not only been vaccinated, they also had taken Tamiflu. And many had taken Tylenol. It’s time to ask the tough questions. The science is there on problems with Tylenol for vaccine-induced fever, and it must be taken into consideration. Fever due to respiratory infections after flu vaccination is still vaccine-induced.
A look at the issues with Tamiflu (see primary scientific literature reviewed here) shows that we cannot ignore the possibility that the human immune system is not infinitely resilient, and that medicine’s approaches to tackling “the flu” is imprecise, not evidence-based, and self-defeating. I’m not talking about the number of antigens the human body can take; I’m talking about the amount of tweaking it can tolerate, especially given the aluminum-dense childhood vaccination schedule. The allopathic medical community would do very well to heed the studies that show that Vitamin D helps alleviate both vaccine injury and severity of viral infections. It helps resolve the unfolded protein response without killing the cells. And the science of ER stress (endoplasmic reticulum stress) shows that Thimerosal is, after all, not safe for human use. Same for aluminum.
Real Reform is Coming – It’s a Mathematical Certainty
Vaccines injure people every day, and kill people every week. Each injury and death informs family members, co-workers, and schoolmates. The flaws in vaccines, combined with misinformation campaigns on safety, fuel the fire and build the vaccine risk aware army. It’s a peaceful army, filled with individuals who are hurt so badly, they do not want others to suffer the same fate. They are altruistic. And under informed, ethical and distributed leadership, they are finding their momentum.
Vaccine safety science reform means removing those in the CDC and HHS that perpetuated the debacle as it grew to proportions that even they could no longer easily deny it. And that’s fine. Let them go. There are many excellent professionals capable of replacing them – people who have not been involved in cooking studies to alter the public’s perception of vaccine risk. People who have withstood unwarranted and unfair criticism by those who live in cowardice of reality. People who now no longer afraid to publish their views. An important question is who among my colleagues in Academic Public Health, and which doctors in Pediatric medicine are willing to #bebrave and take on a debacle as huge as a failed national immunization program? Who will stand up to the AAP and tell them they are wrong?
If you are that type of doctor, it will be easier if you trust those who have worked at this for years. Read Dr. Paul Thomas’ book, The Vaccine Friendly Plan. After the resignations, have him come and teach the entire CDC and HHS what he knows. Consider Dr. Alvin Moss’s wisdom – ask him to create a Conflicts of Interest Policy for CDC and HHS, as he has done for the rest of academic medicine. Bring in Dr. Bob Sears from California, who was willing to stare down threats of the loss of his license to practice medicine because he dared to continue to practice medicine in the face of wanton misinformation and pressure from the AAP. Consider Dr. Richard Frye, and Dr. Chris Exley from the UK, who care first and foremost about the truths that impact total health. Dr. Frye would be great as the new NIH Director, in my opinion. Let these people form a new national public health direction that overrides existing contracts. There are others. Like Dr. Judy Mikovits whose character stands much taller than those who tried – and failed – to silence her – on the issue of adventitious agents in viral vaccines (specifically and quite problematic: retroviruses). Ask Dr. Ted Fogarty about Ethical Vaccinomics, and testing for vaccine injuries. Bring in Dr. John Piesse from Australia and end his persecution there, and put his good will toward safety to work here. We would be lucky to have him.
Create a Manhattan Project focused on reducing vaccine injuries, not on making currently licensed vaccines safer. They are old, and stale, and tired, and they, too, need to go. Bring in exciting new developments in artificial immunization like microneedle patches. Bring in Dr. Kanduc to screen epitopes that are unsafe. Drop aluminum, as many have now called for, and bring in calcium carbonate – if needed at all. Let those pharmaceutical companies who created the disaster make good on their promises to stop making their vaccines. Then we will see new approaches to artificial immunization that compete on the platform of safety.
Don’t just end COIs at ACIP: End ACIP. Create a Vaccine Safety Commission that enforces Science Integrity. Open up the markets. Let ideas thrive. Let consumers choose. Let the FDA do its job. Let the people’s experiences be heard. Establish a paradigm in which the end consumer has a say in the quality of the product. Strip the CDC of the ability to hold patents. End the CDC Foundation. End the differences between drugs and biologics and require randomized clinical trials – with proper placebos, not aluminum hydroxide – for vaccines. Repeal the 1986 Act that protects drug companies from liability for faulty vaccines. Perform random spot checks of vaccines in practices for contamination. The total sum of policies in the National Immunization Program, and the burden of morbidity on the population is a serious threat to our National Security.
Let some new faces and voices drive this reform. Bring in Dr. Dan Neides who had to escape the Cleveland Clinic after speaking his conscience. Let him oversee the transition. Bring in Dr. Brian Hooker to personally issue the pink slips to those who must now go from the CDC. Let all of those named here share his or her experience with Congress. Have Dr. Thompson testify. We need truth and reconciliation. And we need it 42 years ago.
There are MDs who sit in the shadows, silent, and afraid of job loss, sanction, ridicule. Step up. Let your views be known to the current Administration. Join Physicians for Informed Consent. You are not alone. You can help be part of the solution. Attend Health Department meetings and speak up for Informed Consent. Speak up for vaccine exclusions for kids in homes with high lead levels. Speak up for spacing out vaccines and skipping them. Speak up for tolerance and understanding of the pain and anguish parents of kids with autism experience when they are told it’s genetic, they know it’s environmental, and they are told they have to vaccinate their other babies. Speak up against calling CPS for parents who want to take the time they have under the law to consider vaccinations. And, of course, do right by your patients. Listen to their concerns. Inform them of both risks and benefits, as required by Federal Regulations. Let them know they are enrolling themselves or their children (and unborn baby) in post-licensure vaccine safety clinical trials (as required by Federal Regulations). Provide medical and philosophical exemptions for school waivers as required by the laws of your state and the rule of your own conscience. The AAP does not represent the rights and will of the people of the United States of America. Our legislation does.
Let’s aim to not make 2020 vaccination look anything like 2019. We have solutions. We’re now aiming for Healthy People 2050, and the current vaccines have very little to do with our vision. By the way, these ideas don’t come (exclusively) from me. They are shared by hundreds of thousands of American citizens, many of whom have been made sick or lost loved ones to vaccines. #werenotgoingaway #releasetheothermemos #hearthiswell #notmine #Vaxxed #cdctruth #saveourbabies #bebrave #ipak #cdcwhistleblower #rfkcommission #educatebeforeyouvaccinate #vaxxed #learntherisk #wedid #cdclied #stopmandatoryvaccination #learntherisk.”
____________
**Comment**
More just keeps popping out of Pandora’s Box regarding vaccines.
This recent talk shows how vaccines are causing Lyme/MSIDS patients to relapse as well as worsen: https://madisonarealymesupportgroup.com/2018/02/04/dr-muth-immune-issues-and-lyme-msids/
https://madisonarealymesupportgroup.com/2017/12/02/scottish-doctor-gives-insight-on-lyme-msids/ Scottish doctor treating a number of young women who fell ill after their HPV vaccination, which seems to have stimulated a latent Lyme infection to reactivate.
https://madisonarealymesupportgroup.com/2016/04/24/gardasil-and-bartonella/ Asymptomatic girls after receiving Gardasil activated dormant Bartonella which was confirmed by testing.
Great video on the flu vaccine’s ineffectiveness: https://madisonarealymesupportgroup.com/2015/11/08/flu-vaccine-causes-the-flu/
I could go on and on to infinity. Something must be done. Be a part of the solution.



