ICAN’s legal team led by Aaron Siri, sued the National Institutes of Health (NIH) and Moderna to receive a copy of their Covid Vaccine Phase 1 Trial Safety Summary Report and what we found will create an avalanche of opposition to any forced vaccine.
From ICAN:
You and I both know forced vaccines are a bad idea.
You and I both support common-sense exemptions to any vaccine–like exempting those who may have adverse reactions–or those who have pre-existing health conditions where a vaccine may make their health situation worse.
There are many thousands more who have religious reasons for avoiding a mandated vaccine.
There are those who are conscientious objectors–and they lean on the right to say no or opt out.
These are all legitimate reasons — and reasons that have always been supported by our U.S. Constitution and understood to protect all citizens from tyranny. But what if the vaccine itself is unproven.
What if the vaccine itself is hurting people–making them sick, and risking the very lives of those it claims it will save?
This is what ICAN is discovering right now.
In fact, our legal team led by Aaron Siri, sued the National Institutes of Health (NIH) and Moderna to receive a copy of their Covid Vaccine Phase 1 Trial Safety Summary Report and what we found will create an avalanche of opposition to any forced vaccine.
In our initial reporting, we discovered that 70% of trial participants reported adverse events–some of which are extremely concerning.
As promised, I wanted to make sure that you have a copy of this report yourself–so you can be armed with the truth about the Covid 19 vaccine–the truth that the NIH and Moderna DO NOT WANT YOU TO SEE.
This is why I do what I do every day. You see, you and I deserve to know what we are putting into our bodies; I want answers, not stonewalling.
And sadly, the FDA, the NIH, Big Pharma, Big Government, the MainStream Media, Silicon Valley, all of them are COVERING UP and CENSORING THE TRUTH!
The only way ICAN and our weekly television program, The HighWire, can survive is with your support. If you believe in seeking the truth, if you believe in maintaining your liberty and your rights as an American citizen, if you believe in a free and independent press that is unwilling to compromise or cover-up the truth, then I hope you will consider joining our cause today.
Pfizer broke big news this week, that their #Covid19 Vaccine has proven 90% effective in trials. While all major news outlets are in a frenzy, Del has found some shocking information in the fine print.
Analysis evaluated 94 confirmed cases of COVID-19 out of 43,538 participants. This is .2%. Repeat, only .2% reporting.
They have not noted any serious safety concerns for only 2 months.
While the study states it willevaluate the potentialfor the vaccine candidate to provide protection against COVID-19 in those who have had prior exposure to SARS-CoV-2, as well as prevention against severe COVID-19 disease, IT HASN’T YET DONE SO. Therefore, they have not yet obtained whether this vaccine does these things at all.
Re: Covid-19 vaccines: Many ADRs are already expected
Dear Editor
The Ted-tenders electronic daily: Supplement to the Official Journal of the EU, details a contract negotiated by the Medicines and Healthcare Products Agency (MHRA), dated 14.9.20 (1).
It states:
“The MHRA urgently seeks an Artificial Intelligence (AI) software tool to process the expected high volume of Covid-19 vaccine Adverse Drug Reaction (ADRs) and ensure that no details from the ADRs’ reaction text are missed”.
It further explains: “For reasons of extreme urgency under Regulation 32(2)(c) related to the release of a Covid-19 vaccine MHRA have accelerated the sourcing and implementation of a vaccine specific AI tool…… it is not possible to retrofit the MHRA’s legacy systems to handle the volume of ADRs that will be generated by a Covid-19 vaccine. Therefore, if the MHRA does not implement the AI tool, it will be unable to process these ADRs effectively. This will hinder its ability to rapidly identify any potential safety issues with the Covid-19 vaccine and represents a direct threat to patient life and public health”.
Why do they expect that a high volume of ADRs will be generated?
And would it not be more sensible to determine the safety profile of a Covid-19 vaccine while the stable door is shut, rather than monitor the galloping horse once it has bolted?
In 2009 they reached a fraud settlement with the U.S. Department of Justice for $2.3 BILLION, the largest ever fraud settlement in the history of the DOJ at that time. (Source.)
It is very unlikely that Merck, AZ, J&J and Moderna are just going to sit back and let Pfizer dominate this new, lucrative COVID vaccine market. Look for similar press releases from those companies very soon, touting how effective their vaccines are as well, as they look to get their piece of the pie.
Pfizer’s stock has already soared, and market analysis is now predicting that due to this announcement their sales will now reach $258 million in the fourth quarter of 2020, with sales in 2021 expected to reach $4.6 BILLION. (Source.)
All of these companies have already received BILLIONS through Operation Warp Speed, so they will ALL come out ahead financially no matter what happens.
The real losers will be the citizens of the U.S. and other countries who receive these vaccines.
According to a study that examined how informed consent is given to COVID-19 vaccine trial participants, disclosure forms fail to inform volunteers that the vaccine might make them susceptible to more severe disease if they’re exposed to the virus
Previous coronavirus vaccine efforts — including those for SARS, MERS and RSV — have revealed a serious concern: The vaccines have a tendency to trigger antibody-dependent enhancement (ADE)
ADE means that rather than enhance your immunity against the infection, the vaccine actually enhances the virus’ ability to enter and infect your cells, resulting in more severe disease than had you not been vaccinated
Lethal Th2 immunopathology is another potential risk. A faulty T cell response can trigger allergic inflammation, and poorly functional antibodies that form immune complexes can activate the complement system, resulting in airway damage
There’s evidence showing the elderly — who are most vulnerable to severe COVID-19 and would need the vaccine the most — are also the most vulnerable to ADE and Th2 immunopathology
According to a study that examined how informed consent is given to COVID-19 vaccine trial participants, disclosure forms fail to inform volunteers that the vaccine might make them susceptible to more severe disease if they’re exposed to the virus.
The study,1 “Informed Consent Disclosure to Vaccine Trial Subjects of Risk of COVID-19 Vaccine Worsening Clinical Disease,” published in the International Journal of Clinical Practice, October 28, 2020, points out that “COVID-19 vaccines designed to elicit neutralizing antibodies may sensitize vaccine recipients to more severe disease than if they were not vaccinated.”
“Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach (consisting of the unmodified or minimally modified coronavirus viral spike to elicit neutralizing antibodies), be they composed of protein, viral vector, DNA or RNA and irrespective of delivery method, may worsen COVID-19 disease via antibody-dependent enhancement (ADE),” the paper states.
“This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID-19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.
The specific and significant COVID-19 risk of ADE should have been and should be prominently and independently disclosed to research subjects currently in vaccine trials, as well as those being recruited for the trials and future patients after vaccine approval, in order to meet the medical ethics standard of patient comprehension for informed consent.”
What Is Antibody-Dependent Enhancement?
As noted by the authors of that International Journal of Clinical Practice paper, previous coronavirus vaccine efforts — for severe acute respiratory syndrome coronavirus (SARS-CoV), Middle East respiratory syndrome coronavirus (MERS-CoV) and respiratory syncytial virus (RSV) — have revealed a serious concern: The vaccines have a tendency to trigger antibody-dependent enhancement.
What exactly does that mean? In a nutshell, it means that rather than enhance your immunity against the infection, the vaccine actually enhances the virus’ ability to enter and infect your cells, resulting in more severe disease than had you not been vaccinated.2
This is the exact opposite of what a vaccine is supposed to do, and a significant problem that has been pointed out from the very beginning of this push for a COVID-19 vaccine. The 2003 review paper “Antibody-Dependent Enhancement of Virus Infection and Disease” explains it this way:3
“In general, virus-specific antibodies are considered antiviral and play an important role in the control of virus infections in a number of ways. However, in some instances, the presence of specific antibodies can be beneficial to the virus. This activity is known as antibody-dependent enhancement (ADE) of virus infection.
The ADE of virus infection is a phenomenon in which virus-specific antibodies enhance the entry of virus, and in some cases the replication of virus, into monocytes/macrophages and granulocytic cells through interaction with Fc and/or complement receptors.
This phenomenon has been reported in vitro and in vivo for viruses representing numerous families and genera of public health and veterinary importance. These viruses share some common features such as preferential replication in macrophages, ability to establish persistence, and antigenic diversity. For some viruses, ADE of infection has become a great concern to disease control by vaccination.”
Previous Coronavirus Vaccine Efforts Have All Failed
In my May 2020 interview above with Robert Kennedy Jr., he summarized the history of coronavirus vaccine development, which began in 2002, following three consecutive SARS outbreaks. By 2012, Chinese, American and European scientists were working on SARS vaccine development, and had about 30 promising candidates.
Of those, the four best vaccine candidates were then given to ferrets, which are the closest analogue to human lung infections. In the video below, which is a select outtake from my full interview, Kennedy explains what happened next. While the ferrets displayed robust antibody response, which is the metric used for vaccine licensing, once they were challenged with the wild virus, they all became severely ill and died.
The same thing happened when they tried to develop an RSV vaccine in the 1960s. RSV is an upper respiratory illness that is very similar to that caused by coronaviruses. At that time, they had decided to skip animal trials and go directly to human trials.
“They tested it on I think about 35 children, and the same thing happened,” Kennedy said.“The children developed a champion antibody response — robust, durable. It looked perfect [but when] the children were exposed to the wild virus, they all became sick. Two of them died.They abandoned the vaccine. It was a big embarrassment to FDA and NIH.”
Neutralizing Versus Binding Antibodies
Coronaviruses produce not just one but two different types of antibodies:
Neutralizing antibodies,4 also referred to as immoglobulin G (IgG) antibodies, that fight the infection
Binding antibodies5 (also known as nonneutralizing antibodies) that cannot prevent viral infection
Instead of preventing viral infection, binding antibodies trigger an abnormal immune response known as “paradoxical immune enhancement.” Another way to look at this is your immune system is actually backfiring and not functioning to protect you but actually making you worse.
Many of the COVID-19 vaccines currently in the running are using mRNA to instruct your cells to make the SARS-CoV-2 spike protein (S protein). The spike protein, which is what attaches to the ACE2 receptor of the cell, is the first stage of the two-stage process viruses use to gain entry into cells.
The idea is that by creating the SARS-CoV-2 spike protein, your immune system will commence production of antibodies, without making you sick in the process. The key question is, which of the two types of antibodies are being produced through this process?
Without Neutralizing Antibodies, Expect More Severe Illness
In an April 2020 Twitter thread,6 The Immunologist noted: “While developing vaccines … and considering immunity passports, we must first understand the complex role of antibodies in SARS, MERS and COVID-19.” He goes on to list several coronavirus vaccine studies that have raised concerns about ADE.
The first is a 2017 study7 in PLOS Pathogens, ”Enhanced Inflammation in New Zealand White Rabbits When MERS-CoV Reinfection Occurs in the Absence of Neutralizing Antibody,” which investigated whether getting infected with MERS would protect the subject against reinfection, as is typically the case with many viral illnesses. (Meaning, once you recover from a viral infection, say measles, you’re immune and won’t contract the illness again.)
To determine how MERS affects the immune system, the researchers infected white rabbits with the virus. The rabbits got sick and developed antibodies, but those antibodies were not the neutralizing kind, meaning the kind of antibodies that block infection. As a result, they were not protected from reinfection, and when exposed to MERS for a second time, they became ill again, and more severely so.
“In fact, reinfection resulted in enhanced pulmonary inflammation, without an associated increase in viral RNA titers,” the authors noted. Interestingly, neutralizing antibodies were elicited during this second infection, preventing the animals from being infected a third time. According to the authors:
“Our data from the rabbit model suggests that people exposed to MERS-CoV who fail to develop a neutralizing antibody response, or persons whose neutralizing antibody titers have waned, may be at risk for severe lung disease on re-exposure to MERS-CoV.”
In other words, if the vaccine does not result in a robust response in neutralizing antibodies, you might be at risk for more severe lung disease if you’re infected with the virus.
And here’s an important point: COVID-19 vaccines are NOT designed to prevent infection. As detailed in “How COVID-19 Vaccine Trials Are Rigged,” a “successful” vaccine merely needs to reduce the severity of the symptoms.They’re not even looking at reducing infection, hospitalization or death rates.
ADE in Dengue Infections
The Dengue virus is also known to cause ADE. As explained in a Swiss Medical Weekly paper published in April 2020:8
“The pathogenesis of COVID-19 is currently believed to proceed via both directly cytotoxic and immune-mediated mechanisms. An additional mechanism facilitating viral cell entry and subsequent damage may involve the so-called antibody-dependent enhancement (ADE).
ADE is a very well-known cascade of events whereby viruses may infect susceptible cells via interaction between virions complexed with antibodies or complement components and, respectively, Fc or complement receptors, leading to the amplification of their replication.
This phenomenon is of enormous relevance not only for the understanding of viral pathogenesis, but also for developing antiviral strategies, notably vaccines …
There are four serotypes of Dengue virus, all eliciting protective immunity. However, although homotypic protection is long-lasting, cross-neutralizing antibodies against different serotypes are short-lived and may last only up to 2 years.
In Dengue fever, reinfection with a different serotype runs a more severe course when the protective antibody titer wanes. Here, non-neutralizing antibodies take over neutralizing ones, bind to Dengue virions, and these complexes mediate the infection of phagocytic cells via interaction with the Fc receptor, in a typical ADE.
In other words, heterotypic antibodies at subneutralizing titres account for ADE in persons infected with a serotype of Dengue virus that is different from the first infection.
Cross-reactive neutralizing antibodies are associated with decreased odds of symptomatic secondary infection, and the higher the titer of such antibodies following the primary infection, the longer the delay to symptomatic secondary infection …”
The paper goes on to detail results from follow-up investigations into the Dengue vaccine, which revealed the hospitalization rate for Dengue among vaccinated children under the age of 9 was greater than the rate among controls. The explanation for this appears to be that the vaccine mimicked a primary infection, and as that immunity waned, the children became susceptible to ADE when they encountered the virus a second time. The author explains:
“A post hoc analysis of efficacy trials, using an anti-nonstructural protein 1 immunoglobulin G (IgG) enzyme-linked immunosorbent assay (ELISA) to distinguish antibodies elicited by wild-type infection from those following vaccination, showed that the vaccine was able to protect against severe Dengue [in] those who had been exposed to the natural infection before vaccination, and that the risk of severe clinical outcome was increased among seronegative persons.
Based on this, a Strategic Advisor Group of Experts convened by World Health Organization (WHO) concluded that only Dengue seropositive persons should be vaccinated whenever Dengue control programs are planned that include vaccination.”
ADE in Coronavirus Infections
This could end up being important for the COVID-19 vaccine. Hypothetically speaking, if SARS-CoV-2 works like Dengue, which is also caused by an RNA virus, then anyone who has not tested positive for SARS-CoV-2 might actually be at increased risk for severe COVID-19 after vaccination, and only those who have already recovered from a bout of COVID-19 would be protected against severe illness by the vaccine.
To be clear, we do not know whether that is the case or not, but these are important areas of inquiry and the current vaccine trials will simply not be able to answer this important question.
The Swiss Medical Weekly paper9 also reviews the evidence of ADE in coronavirus infections, citing research showing inoculating cats against the feline infectious peritonitis virus (FIPV) — a feline coronavirus — increases the severity of the disease when challenged with the same FIPV serotype as that in the vaccine.
The paper also cites research showing “Antibodies elicited by a SARS-CoV vaccine enhanced infection of B cell lines in spite of protective responses in the hamster model.” Another paper,10“Antibody-Dependent SARS Coronavirus Infection Is Mediated by Antibodies Against Spike Proteins,” published in 2014, found that:
“… higher concentrations of anti-sera against SARS-CoV neutralized SARS-CoV infection, while highly diluted anti-sera significantly increased SARS-CoV infection and induced higher levels of apoptosis.
Results from infectivity assays indicate that SARS-CoV ADE is primarily mediated by diluted antibodies against envelope spike proteins rather than nucleocapsid proteins. We also generated monoclonal antibodies against SARS-CoV spike proteins and observed that most of them promoted SARS-CoV infection.
Combined, our results suggest that antibodies against SARS-CoV spike proteins may trigger ADE effects. The data raise new questions regarding a potential SARS-CoV vaccine …”
A study11 that ties into this was published in the journal JCI Insight in 2019. Here, macaques vaccinated with a modified vaccinia Ankara (MVA) virus encoding full-length SARS-CoV spike protein ended up with more severe lung pathology when the animals were exposed to the SARS virus. And, when they transferred anti-spike IgG antibodies into unvaccinated macaques, they developed acute diffuse alveolar damage, likely by “skewing the inflammation-resolving response.”
SARS Vaccine Worsens Infection After Challenge With SARS-CoV
An interesting 2012 paper12 with the telling title, “Immunization with SARS Coronavirus Vaccines Leads to Pulmonary Immunopathology on Challenge with the SARS Virus,” demonstrates what many researchers now fear, namely that COVID-19 vaccines may end up making people more prone to severe SARS-CoV-2 infection.
The paper reviews experiments showing immunization with a variety of SARS vaccines resulted in pulmonary immunophathology once challenged with the SARS virus. As noted by the authors:13
“Inactivated whole virus vaccines whether inactivated with formalin or beta propiolactone and whether given with our without alum adjuvant exhibited a Th2-type immunopathologic in lungs after challenge.
As indicated, two reports attributed the immunopathology to presence of the N protein in the vaccine; however, we found the same immunopathologic reaction in animals given S protein vaccine only, although it appeared to be of lesser intensity.
Thus, a Th2-type immunopathologic reaction on challenge of vaccinated animals has occurred in three of four animal models (not in hamsters) including two different inbred mouse strains with four different types of SARS-CoV vaccines with and without alum adjuvant. An inactivated vaccine preparation that does not induce this result in mice, ferrets and nonhuman primates has not been reported.
This combined experience provides concern for trials with SARS-CoV vaccines in humans. Clinical trials with SARS coronavirus vaccines have been conducted and reported to induce antibody responses and to be ‘safe.’ However, the evidence for safety is for a short period of observation.
The concern arising from the present report is for an immunopathologic reaction occurring among vaccinated individuals on exposure to infectious SARS-CoV, the basis for developing a vaccine for SARS. Additional safety concerns relate to effectiveness and safety against antigenic variants of SARS-CoV and for safety of vaccinated persons exposed to other coronaviruses, particularly those of the type 2 group.”
The Elderly Are Most Vulnerable to ADE
On top of all of these concerns, there’s evidence showing the elderly — who are most vulnerable to severe COVID-19 — are also the most vulnerable to ADE. Preliminary research findings14 posted on the preprint server medRxiv at the end of March 2020 reported that middle-aged and elderly COVID-19 patients have far higher levels of anti-spike antibodies — which, again, increase infectivity — than younger patients.
Immune Enhancement Is a Serious Concern
Another paper worth mentioning is the May 2020 mini review15 “Impact of Immune Enhancement on COVID-19 Polyclonal Hyperimmune Globulin Therapy and Vaccine Development.” As in many other papers, the authors point out that:16
“While development of both hyperimmune globulin therapy and vaccine against SARS-CoV-2 are promising, they both pose a common theoretical safety concern. Experimental studies have suggested the possibility of immune-enhanced disease of SARS-CoV and MERS-CoV infections, which may thus similarly occur with SARS-CoV-2 infection …
Immune enhancement of disease can theoretically occur in two ways. Firstly, non-neutralizing or sub-neutralizing levels of antibodies can enhance SARS-CoV-2 infection into target cells.
Secondly, antibodies could enhance inflammation and hence severity of pulmonary disease. An overview of these antibody dependent infection and immunopathology enhancement effects are summarized in Fig. 1 …
Currently, there are multiple SARS-CoV and MERS-CoV vaccine candidates in pre-clinical or early phase clinical trials. Animal studies on these CoVs have shown that the spike (S) protein-based vaccines (specifically the receptor binding domain, RBD) are highly immunogenic and protective against wild-type CoV challenge.
Vaccines that target other parts of the virus, such as the nucleocapsid, without the S protein, have shown no protection against CoV infection and increased lung pathology. However, immunization with some S protein based CoV vaccines have also displayed signs of enhanced lung pathology following challenge.
Hence, besides the choice of antigen target, vaccine efficacy and risk of immunopathology may be dependent on other ancillary factors, including adjuvant formulation, age at vaccination … and route of immunization.”
Figure 1: Mechanism of ADE and antibody mediated immunopathology. Left panel: For ADE, immune complex internalization is mediated by the engagement of activating Fc receptors on the cell surface. Co-ligation of inhibitory receptors then results in the inhibition of antiviral responses which leads to increased viral replication. Right panel: Antibodies can cause immunopathology by activating the complement pathway or antibody-dependent cellular cytotoxicity (ADCC). For both pathways, excessive immune activation results in the release of cytokines and chemokines, leading to enhanced disease pathology.
Do a Risk-Benefit Analysis Before Making Up Your Mind
In all likelihood, regardless of how effective (or ineffective) the COVID-19 vaccines end up being, they’ll be released to the public in relatively short order. Most predict one or more vaccines will be ready sometime in 2021.
Ironically, the data17,18,19 we now have no longer support a mass vaccination mandate, considering the lethality of COVID-19 is lower than the flu for those under the age of 60.20
If you’re under the age of 40, your risk of dying from COVID-19 is just 0.01%, meaning you have a 99.99% chance of surviving the infection. And you could improve that to 99.999% if you’re metabolically flexible and vitamin D replete.
So, really, what are we protecting against with a COVID-19 vaccine? As mentioned, the vaccines aren’t even designed to prevent infection, only reduce the severity of symptoms.Meanwhile, they could potentially make you sicker once you’re exposed to the virus. That seems like a lot of risk for a truly questionable benefit.
To circle back to where we started, participants in current COVID-19 vaccine trials are not being told of this risk — that by getting the vaccine they may end up with more severe COVID-19 once they’re infected with the virus.
Lethal Th2 Immunopathology Is Another Potential Risk
In closing, consider what this PNAS news feature states about the risk of vaccine-induced immune enhancement and dysfunction, particularly for the elderly, the very people who would need the protection a vaccine might offer the most:21
“Since the 1960s, tests of vaccine candidates for diseases such as dengue, respiratory syncytial virus (RSV), and severe acute respiratory syndrome (SARS) have shown a paradoxical phenomenon:
Some animals or people who received the vaccine and were later exposed to the virus developed more severe disease than those who had not been vaccinated. The vaccine-primed immune system, in certain cases, seemed to launch a shoddy response to the natural infection …
This immune backfiring, or so-called immune enhancement, may manifest in different ways such as antibody-dependent enhancement (ADE), a process in which a virus leverages antibodies to aid infection; or cell-based enhancement, a category that includes allergic inflammation caused by Th2 immunopathology. In some cases, the enhancement processes might overlap …
Some researchers argue that although ADE has received the most attention to date, it is less likely than the other immune enhancement pathways to cause a dysregulated response to COVID-19, given what is known about the epidemiology of the virus and its behavior in the human body.
‘There is the potential for ADE, but the bigger problem is probably Th2 immunopathology,’ says Ralph Baric, an epidemiologist and expert in coronaviruses … at the University of North Carolina at Chapel Hill.
In previous studies of SARS, aged mice were found to have particularly high risks of life-threatening Th2 immunopathology … in which a faulty T cell response triggers allergic inflammation, and poorly functional antibodies that form immune complexes, activating the complement system and potentially damaging the airways.”
Hopefully it is abundantly clear this vaccine could be the kiss of death for Lyme/MSIDS patients if ADE happens.
Not only is this vaccine NOT needed, it is experimental – which means there are many unanswered questions. The fact they are not being honest with vaccine volunteers does not bode well with transparency and honesty. If they will withhold information in early research, will they not also withhold other critical information?
Also, there are proven treatments that are working beautifully.
Originally, the flu vaccine was a measure to protect the elderly, but go here for a blast from the past when four scientists researching the Flu vaccine during the 1960s found it to be ineffectiveand refused to give it to their own families. The scientists state they were prevented from publishing their negative findings.
Despite this, the ineffective and dangerous vaccine has increasingly been pushed on everyone 6 months old and up, including pregnant women despite the fact the flu vaccine is linked to increased risk of miscarriage.
Now a recent Japanese study shows NO BENEFIT on hard outcomes: hospitalization and death. Another perfect example of how the massive push to vaccinate people for the flu has been a waste of time and effort. Do not expect to read about this in the news.
Further demonstrating the diabolical history behind vaccines, the military mandated the Adenovirus vaccine for ‘cold-like symptoms’:
”…when it was shown that the vaccine contained a contaminant which caused cancer in laboratory animals, it was taken off the market, but that was 3 years after the division’s scientists have pointed out the danger…”
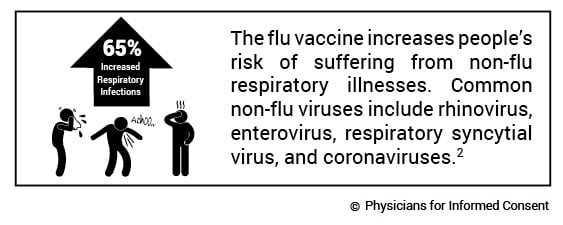
1. THE FLU VACCINE INCREASES THE RISK OF CONTRACTING A NON-FLU RESPIRATORY ILLNESS BY 65%.
Although some studies suggest positive effects of the flu vaccine on the incidence of illness caused by flu viruses, that benefit is potentially outweighed by the negative effects of the flu vaccine on the incidence of non-flu respiratory illness.1 To address the concern among patients that the flu vaccine causes illness (i.e., acute respiratory illness), the Centers for Disease Control and Prevention (CDC) funded a three-year study,2 published in Vaccine, to analyze the risk of illness after flu vaccination compared to the risk of illness in unvaccinated individuals.
The study found there is a 65% increased risk of suffering from a non-flu acute respiratory illness within 14 days of receiving the flu vaccine. The authors state, “Patients’ experiences of illness after vaccination may be validated by these results.”
This is important because although flu vaccines target three or four strains of flu virus,3 over 200 different viruses cause illnesses that produce the same symptoms—fever, headache, aches, pains, cough, and runny nose—as influenza,4 and more than 85% of acute respiratory illnesses do not involve the flu.5
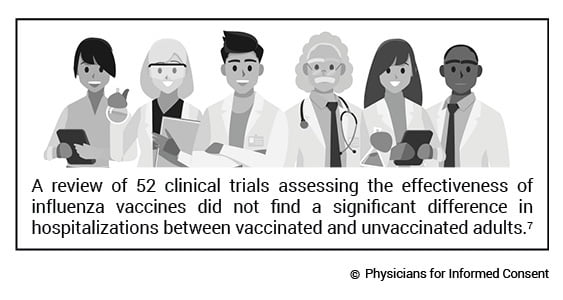
2. THE FLU VACCINE DOESN’T REDUCE DEMAND ON HOSPITALS.
The National Institute of Health (NIH) funded a study6 to measure the effect of seasonal influenza vaccination on hospitalization among the elderly. The study analyzed 170 million episodes of medical care and found that “no evidence indicated that vaccination reduced hospitalizations.”
In addition, a 2018 Cochrane review7 of 52 clinical trials assessing the effectiveness of influenza vaccines did not find a significant difference in hospitalizations between vaccinated and unvaccinated adults. Instead, the reviewers found “low-certainty evidence that hospitalization rates and
time off work may be comparable between vaccinated and unvaccinated adults.”
Furthermore, the Mayo Clinic conducted a case-control study8 to analyze the effectiveness of the trivalent inactivated influenza vaccine (TIV) in preventing flu hospitalization in children 6 months to 18 years old. The study evaluated the risk of hospitalization in both vaccinated and unvaccinated children over an eight-year period. The authors state: “TIV is not effective in preventing laboratory-confirmed influenza-related hospitalization in children.” Instead, “[W]e found a threefold increased risk of hospitalization in subjects who did get the TIV vaccine.”
3. THE FLU VACCINE DOESN’T PREVENT THE SPREAD OF THE FLU.
Households are thought to play a major role in community spread of influenza, and there has been a long history of analyzing family households to study the incidence and transmission of respiratory illnesses of all severities. As such, the CDC funded a study9 of 1,441 participants, both vaccinated and unvaccinated, in 328 households. The study evaluated the flu vaccine’s ability to prevent community-acquired influenza (household index cases) and influenza acquired in people with confirmed household exposure to the flu (secondary cases). Transmission risks were determined and characterized.
In conclusion, the authors state: “There was no evidence that vaccination prevented household transmission once influenza was introduced.”9,10
Furthermore, a systematic review5 of 50 influenza vaccine studies conducted for the Cochrane Library states: “Influenza vaccines have a modest effect in reducing influenza symptoms and working days lost. There is no evidence that they affect complications, such as pneumonia, or transmission.”
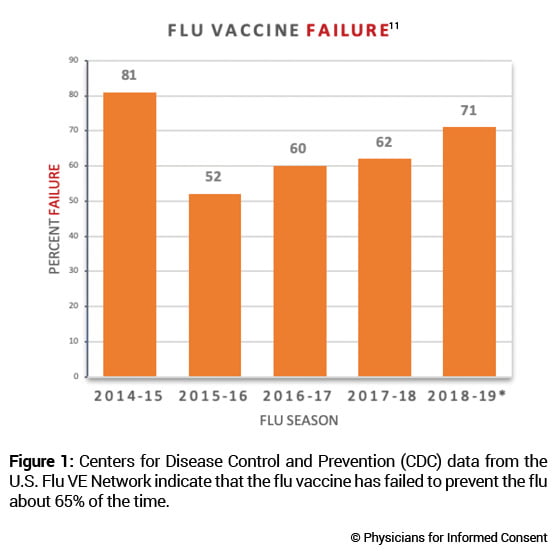
4. THE FLU VACCINE FAILS TO PREVENT THE FLU ABOUT 65% OF THE TIME.
The CDC conducts studies to assess the effects of flu vaccination each flu season to help determine if flu vaccines are working as intended.11 As circulating flu viruses are constantly changing (primarily due to antigenic drift mutations),12flu vaccines are reformulated regularly based on a “best guess” of which viruses might circulate during the coming flu season.3 The CDC states: “CDC monitors vaccine effectiveness annually through the Influenza Vaccine Effectiveness (VE) Network, a collaboration with participating institutions in five geographic locations… [A]nnual estimates of vaccine effectiveness give a real-world look at how well the vaccine protects against influenza caused by circulating viruses each season.”13
Data from the CDC’s Influenza VE Network indicate a 65% vaccine failure rate between 2014 and 2018 (Fig. 1).11
5. REPEAT DOSES OF THE FLU VACCINE MAY INCREASE THE RISK OF FLU VACCINE FAILURE.
Studies have observed that influenza vaccines have low effectiveness in individuals who are vaccinated in two consecutive years.9 A review of 17 influenza vaccine studies published in Expert Review of Vaccines states, “The effects of repeated annual vaccination on individual long-term protection, population immunity, and virus evolution remain largely unknown.”14
6. DEATH FROM INFLUENZA IS RARE IN CHILDREN.
Before the widespread use of the influenza vaccine in children, between 2000 and 2003, each year kids age 18 and younger had about 1 in 1.26 million or 0.00008% chance of dying from the flu.15 In a 2004 report, the CDC stated, “Deaths from influenza are uncommon among children with and without high-risk conditions.”16
7. THE FLU VACCINE DOESN’T REDUCE DEATHS FROM PNEUMONIA AND FLU.
The National Vaccine Program Office, a division of the U.S. Department of Health and Human Services (HHS), funded a study17 to examine flu mortality over the period of 33 years (1968–2001). The study found that there has been no decrease in flu mortality since the widespread use of the influenza vaccine. The authors state: “We could not correlate increasing vaccination coverage after 1980 with declining mortality rates in any age group… [W]e conclude that observational studies substantially overestimate vaccination benefit.”
Furthermore, the National Institute of Health (NIH) funded a study6 to measure the effect of seasonal influenza vaccination on mortality among the elderly. The study analyzed 7.6 million deaths and found “a sharp increase in influenza vaccination rates at age 65 years with no matching decrease in hospitalization or mortality rates.”
8. PATIENTS DON’T BENEFIT FROM THE VACCINATION OF HEALTHCARE WORKERS.
A review18 of more than 30 influenza vaccine studies conducted for the Cochrane Library states, “Our review findings have not identified conclusive evidence of benefit of HCW [healthcare workers] vaccination programs on specific outcomes of laboratory-proven influenza, its complications (lower respiratory tract infection, hospitalization or death due to lower respiratory tract illness), or all cause mortality in people over the age of 60.” The authors conclude, “This review does not provide reasonable evidence to support the vaccination of healthcare workers to prevent influenza.” In addition, “There is little evidence to justify medical care and public health practitioners mandating influenza vaccination for healthcare workers.”
9. FLU VACCINE MANDATES ARE NOT SCIENCE-BASED.
A Cochrane Vaccines Field analysis19 evaluated studies measuring the benefits of flu vaccination. The analysis, published in the BMJ, concludes: “The large gap between policy and what the data tell us (when rigorously assembled and evaluated) is surprising… Evidence from systematic reviews shows that inactivated vaccines have little or no effect on the effects measured… Reasons for the current gap between policy and evidence are unclear, but given the huge resources involved, a re-evaluation should be urgently undertaken.”
Dierig A, Heron LG, Lambert SB, Yin JK, Leask J, Chow MY, Sloots TP, Nissen MD, Ridda I, Booy R. Epidemiology of respiratory viral infections in children enrolled in a study of influenza vaccine effectiveness. Influenza Other Respir Viruses. 2014 May;8(3):293-301. Epub 2014 Jan 31.
Rikin S, Jia H, Vargas CY, Castellanos de Belliard Y, Reed C, LaRussa P, Larson EL, Saiman L, Stockwell MS. Assessment of temporally related acute respiratory illness following influenza vaccination. Vaccine. 2018 Apr 5;36(15):1958-64.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. Selecting viruses for the seasonal influenza vaccine; [cited 2020 Aug 17]. https://www.cdc.gov/flu/prevent/vaccine-selection.htm.
Demicheli V, Jefferson T, Al-Ansary LA, Ferroni E, Rivetti A, Di Pietrantonj C. Vaccines for preventing influenza in healthy adults. Cochrane Database of Syst Rev. 2014 Mar 13;(3):CD001269.
Jefferson T, Di Pietrantonj C, Rivetti A, Bawazeer GA, Al-Ansary LA, Ferroni E. Vaccines for preventing influenza in healthy adults. Cochrane Database Sys Rev. 2010 Jul 7;(7):CD001269.
Anderson ML, Dobkin C, Gorry D. The effect of influenza vaccination for the elderly on hospitalization and mortality: an observational study with a regression discontinuity design. Ann Intern Med. 2020 Apr 7;172(7):445-52.
Demicheli V, Jefferson T, Ferroni E, Rivetti A, Di Pietrantonj C. Vaccines for preventing influenza in healthy adults. Cochrane Database Syst Rev. 2018 Feb 1;2(2):CD001269.
Joshi AY, Iyer VN, Hartz MF, Patel AM, Li JT. Effectiveness of trivalent inactivated influenza vaccine in influenza-related hospitalization in children: a case-control study. Allergy Asthma Proc. 2012 Mar-Apr;33(2):e23-7.
Ohmit SE, Petrie JG, Malosh RE, Cowling BJ, Thompson MG, Shay DK, Monto AS. Influenza vaccine effectiveness in the community and the household. Clin Infect Dis. 2013 May;56(10):1363.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. How the flu virus can change: ‘drift’ and ‘shift’; [cited 2020 Aug 17]. https://www.cdc.gov/flu/about/viruses/change.htm.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. How flu vaccine effectiveness and efficacy are measured; [cited 2020 May 14]. https://www.cdc.gov/flu/vaccines-work/effectivenessqa.htm.
Belongia EA, Skowronski DM, McLean HQ, Chambers C, Sundaram ME, De Serres G. Repeated annual influenza vaccination and vaccine effectiveness: review of evidence. Expert Rev Vaccines. 2017 Jul;16(7):723,733.
Centers for Disease Control and Prevention. Washington, D.C.: U.S. Department of Health and Human Services. CDC wonder: about underlying cause of death, 1999-2018; [cited 2020 May 2]. https://wonder.cdc.gov/ucd-icd10.html; query for death from influenza, 2000-2003. Between 2000 and 2003, there were 61 annual deaths from influenza out of 77 million children age 18 and younger, about 1 death in 1.26 million.
Harper SA, Fukuda K, Uyeki TM, Cox NJ, Bridges CB; Centers for Disease Control and Prevention (CDC) Advisory Committee on Immunization Practices (ACIP). Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep. 2004 May 28;53(RR-6):1-40.
Simonsen L, Reichert TA, Viboud C, Blackwelder WC, Taylor RJ, Miller MA. Impact of influenza vaccination on seasonal mortality in the US elderly population. Arch Intern Med. 2005 Feb 14;165(3):265-72.
Thomas RE, Jefferson T, Lasserson TJ. Influenza vaccination for healthcare workers who care for people aged 60 or older living in long-term care institutions. Cochrane Database Syst Rev. 2016 Jun 2;(6):CD005187.
Jefferson T. Influenza vaccination: policy versus evidence. BMJ. 2006 Oct 28;333(7574):912-5.
Cochrane’s 2018 review9 of 52 clinical studies on vaccines for preventing influenza in adults, including pregnant women, found only 15% of the studies were well-designed and conducted. Based on 25 studies that looked at inactivated influenza vaccines, Cochrane concluded they have only a minor protective effect against influenza and influenza-like illness (ILI), noting:
“Inactivated influenza vaccines probably reduce influenza in healthy adults from 2.3% without vaccination to 0.9% and they probably reduce ILI from 21.5% to 18.1% … 71 healthy adults need to be vaccinated to prevent one of them experiencing influenza, and 29 healthy adults need to be vaccinated to prevent one of them experiencing an ILI …
In its 2018 review10 of 41 clinical trials on live and inactivated vaccines for preventing influenza in children, they found:
“Compared with placebo or do nothing, live attenuated influenza vaccines probably reduce the risk of influenza infection in children aged 3 to 16 years from 18% to 4%, and they may reduce ILI by a smaller degree, from 17% to 12% …
This particularly frightening statement was given:
“Adverse event data were not well described in the available studies. Standardized approaches to the definition, ascertainment, and reporting of adverse events are needed.”
The Cochrane review also concluded that recommendations for routine use of influenza vaccine as a routine public health measure was not supported by the published evidence base and stated,
“The results of this review provide no evidence for the utilisation of vaccination against influenza in healthy adults as a routine public health measure. As healthy adults have a low risk of complications due to respiratory disease, the use of the vaccine may only be advised as an individual protective measure.” 13
A new study examining how informed consent is given to the COVID vaccine trial participants found that disclosure forms were not sufficient for the participants to understand that the vaccine could make them more susceptible to worse disease later.
“COVID‐19 vaccines designed to elicit neutralizing antibodies may sensitize vaccine recipients to more severe disease than if they were not vaccinated,” study authors said.
“Vaccines for SARS, MERS and RSV have never been approved, and the data generated in the development and testing of these vaccines suggest a serious mechanistic concern: that vaccines designed empirically using the traditional approach … may worsen COVID‐19 disease via antibody‐dependent enhancement (ADE).
“This risk is sufficiently obscured in clinical trial protocols and consent forms for ongoing COVID‐19 vaccine trials that adequate patient comprehension of this risk is unlikely to occur, obviating truly informed consent by subjects in these trials.”











Rapid Response:
Re: Covid-19 vaccines: Many ADRs are already expected
Dear Editor
The Ted-tenders electronic daily: Supplement to the Official Journal of the EU, details a contract negotiated by the Medicines and Healthcare Products Agency (MHRA), dated 14.9.20 (1).
It states:
It further explains: “For reasons of extreme urgency under Regulation 32(2)(c) related to the release of a Covid-19 vaccine MHRA have accelerated the sourcing and implementation of a vaccine specific AI tool…… it is not possible to retrofit the MHRA’s legacy systems to handle the volume of ADRs that will be generated by a Covid-19 vaccine. Therefore, if the MHRA does not implement the AI tool, it will be unable to process these ADRs effectively. This will hinder its ability to rapidly identify any potential safety issues with the Covid-19 vaccine and represents a direct threat to patient life and public health”.
Why do they expect that a high volume of ADRs will be generated?
And would it not be more sensible to determine the safety profile of a Covid-19 vaccine while the stable door is shut, rather than monitor the galloping horse once it has bolted?
(1) https://ted.europa.eu/udl?uri=TED:NOTICE:506291-2020:TEXT:EN:HTML&src=0
Competing interests: No competing interests