https://slate.com/technology/2018/06/the-science-isnt-settled-on-chronic-lyme.html
The Science Isn’t Settled on Chronic Lyme
A close look at the evidence suggests the controversial diagnosis should be taken more seriously, and that decades of sexism may be to blame for our collective dismissal.
By MAYA DUSENBERY and JULIE REHMEYER
JUNE 27, 2018
Porochista Khakpour’s new memoir, Sick, describes her experience of decades of severe illness from chronic Lyme disease. The thought-provoking book has spurred a conversation about the nature of illness narratives, the impact of sexism on women’s health, and the ills of modern life, along with recommendations from Oprah Magazine and Cheryl Strayed.
It has also received criticism due to the debate around whether chronic Lyme disease is a “real” condition. The Infectious Disease Society of America, or IDSA, has repeatedly and flatly claimed that the whole notion of chronic Lyme is “not based on scientific fact.” Slate’s own coverage of the disease has proposed that it’s a “phantom diagnosis“ that likely indicates a mental health problem, and has likened belief in the disease to being a creationist or anti-vaxxer. Casey Johnston, an editor at the Outline, tweeted earlier this month, “making chronic lyme, a fake disease, about believing women is as helpful to the cause as the rolling stone rape victim’s fabricated story.” These interpretations suggest Khakpour’s memoir is a dangerous tale of delusion.
As journalists who have studied other contested diseases, the disdain and scientific drumbeating of the critics of chronic Lyme raised our suspicions. One of us (Julie Rehmeyer) has written extensively about bad research practices in myalgic encephalomyelitis/chronic fatigue syndrome, aka ME/CFS, and published a memoir about navigating a poorly understood illness, Through the Shadowlands: A Science Writer’s Odyssey Into an Illness Science Doesn’t Understand. And one of us (Maya Dusenbery) has written a book about gender bias in medicine, Doing Harm: The Truth About How Bad Medicine and Lazy Science Leave Women Dismissed, Misdiagnosed, and Sick. We’ve dug into the science and politics of Lyme, and we’ve found that this dismissive position doesn’t have a scientific leg to stand on—and further, that the dynamics around the illness are significantly driven by sexism.
At this point, we simply don’t have an easy way to definitely know if someone has previously been exposed to B. burgdorferi—let alone if they are actively infected.
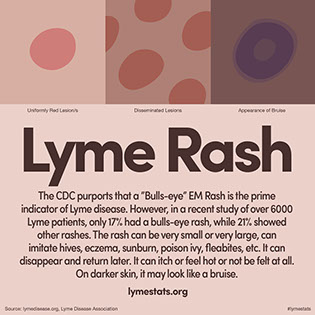
First, there’s no debate that early Lyme disease—an infection of B. burgdorferi bacterium, contracted via a tick—is a real thing. The CDC estimates that 300,000 people a year get it. In its early stage, patients commonly experience flu-like symptoms and a hallmark bulls-eye–shaped rash. There’s also no debate that, if untreated, it can disseminate throughout the body and advance to late Lyme disease, which is marked by far more debilitating symptoms including arthritis, fatigue, pain, heart complications, neurological problems, and more.
For most Lyme patients, a two-to-four-week course of antibiotics is enough to resolve their symptoms for good. But not everyone: Widely accepted studies have found that about 10–20 percent of those treated for Lyme are left with lingering symptoms. The question is what happens then. If a patient has received a Lyme diagnosis, been treated, and continues to experience symptoms, they are said to be suffering from post-treatment Lyme disease syndrome, or PTLDS, which the CDC recognizes. Some patients, though, have symptoms and a medical history that suggest PTLDS but they don’t qualify for the condition, usually because they lack a positive blood test or other objective evidence of infection with B. burgdorferi. A group of self-described Lyme-literate doctors may diagnose them with “chronic Lyme.”
Khakpour has tested positive on the CDC-approved blood tests for Lyme. And she’s well aware that affords her somewhat more legitimacy than many other Lyme patients; she notes that she’s learned to inform medical professionals that hers is a “CDC-recognized case” to try to stave off suspicions. Yet she has still been subject to countless interactions with health care providers “who could barely stifle their rolled eyes” at hearing she has Lyme. Indeed, despite the CDC’s stamp of approval and the fact that even conservative estimates suggest that at least 30,000 people every year develop PTLDS, it isn’t treated with all that much more respect than chronic Lyme. Skeptics argue that the array of symptoms PTLDS patients experience—muscle and joint pain, fatigue, cognitive problems—are so subjective and nonspecific that they may have nothing to do with Lyme disease. Sufferers’ true problem might be psychiatric—depression or “maladaptive belief systems“ or “a tendency to somatization.” Or patients may be overselling how bad it is: In its 2006 guidelines, IDSA stated, “In many patients, posttreatment symptoms appear to be more related to the aches and pains of daily living rather than to either Lyme disease or a tick-borne coinfection.”
There’s actually ample evidence against the theories that PTLDS is all in one’s head. In 2012, researchers from the Johns Hopkins Lyme Disease Research Center tracked a group of patients treated for Lyme disease to see which of them had ongoing symptoms six months later, and it found no psychological differences between those patients who did and didn’t. A 2017 study by the same research team debunked the claim that such symptoms are no worse than the background complaints of the general population. Compared to healthy controls, PTLDS patients reported significantly greater levels of 25 different symptoms—especially fatigue, muscle and joint pain, sleep disturbances, and cognitive problems—and had much worse quality of life. In 2001, a study in the New England Journal of Medicine found that PTLDS patients were as impaired as those in congestive heart failure.
Researchers are also beginning to find the physiological footprints of the illness. A 2011 study from Columbia found unique proteins in the spinal fluid of cognitively impaired patients treated for Lyme disease that distinguished them both from healthy controls and patients with ME/CFS (another illness that has been treated with disdain and that showed its own unique, identifying proteins). Two different groups found immune markers that remained elevated in early Lyme patients who went on to develop chronic symptoms after their initial treatment, but not in those who recovered. A group at Cornell found autoantibodies directed against neurons in PTLDS patients but not in healthy recovered Lyme patients. And a brain-imaging study found abnormalities in cognitively impaired patients with treated Lyme disease, compared to healthy controls.
So even PTLDS patients, with a diagnosis that is officially accepted, have to cope with a skepticism that isn’t scientifically grounded. Chronic Lyme patients have even less evidence to stand on (all the research is conducted on PTLDS patients), and conversations around their plight can go beyond skepticism to downright dismissal. As Brian Palmer wrote for Slate in 2013, “This form of chronic Lyme is controversial in the same sense that rhinoceros horn therapy is controversial: There’s no reliable data to support it.”
The problem with that perspective is that we’ve also known for a long time that blood tests for Lyme—the primary form of “objective evidence”—are lousy. They give high rates of both false negatives and false positives. The CDC-approved tests don’t detect the bacterium itself—they look for antibodies the body produces to fight the infection. But the immune system generally needs six weeks to generate those antibodies, so in the earliest stage, when detection is most important, the test will be negative in 60 percent of patients. And even after six weeks, the test doesn’t turn positive for everyone exposed. A lasting negative result is particularly likely if a patient happens to take antibiotics during that period, which would greatly reduce the need for an antibody response. Also, the B. burgdorferi bacterium may be able to permanently suppress some people’s immune systems, leaving them both unable to generate the strong antibody response that will create a positive test result and more susceptible to all manner of infection for years to come. A 2015 review of 78 studies of the available Lyme-disease tests concluded by throwing up its hands: “The data in this review do not provide sufficient evidence to make inferences about the value of the tests for clinical practice.”
And unfortunately, the other indicators doctors look for—a known tick bite or a bulls-eye rash—are no better. Up to 30 percent of patients never get a rash, and most patients never saw the tick that bit them, which can be as small as the head of a pin. The result is that misdiagnosis is shockingly common: According to a 2009 study, more than half of patients who didn’t get the classic bulls-eye rash were initially misdiagnosed, along with nearly one-quarter of those who did.
So patients without a positive test may not have reliable data to support their belief that they have Lyme disease—but they also don’t have reliable data suggesting they don’t. At this point, we simply don’t have an easy way to definitely know if someone has previously been exposed to B. burgdorferi—let alone if they are actively infected. That means that some patients with a diagnosis of chronic Lyme probably do have something else entirely unrelated to Lyme. But the problem of misdiagnosis surely goes in both directions; we don’t know how many patients with other poorly understood syndromes or “medically unexplained symptoms” are actually suffering from the aftereffects of a Lyme infection.
Our inability to reliably detect infection is an enormous problem when it comes to trying to determine just what is keeping some Lyme patients chronically sick. And further, the mainstream position has been that a short course of antibiotics is enough to kill off the Lyme bacteria nearly every time; even long-standing late Lyme should respond to a month of intravenous antibiotics, perhaps with one retreatment. But that’s an extraordinary claim for two reasons. First, how often is any treatment effective for virtually every patient, particularly with a devastating, multisystem illness? And second, without an accurate routine test that can determine whether someone is currently infected, we also can’t test to see if they’ve been cured. As Mary Beth Pfeiffer, author of the powerful new book Lyme: The First Epidemic of Climate Change, puts it, “If we can’t even tell if they’re actively infected, how can we say that they’re not?”
And indeed, recent research is demonstrating that B. burgdorferi can survive antibiotic treatment. For one thing, B. burgdorferi bacteria have been doused with high quantities of very potent antibiotics in test tubes, and some have still survived. Dogs, mice, and rhesus monkeys have undergone antibiotic treatment and still harbored live B. burgdorferi bacteria. Humans are harder to study: B. burgdorferi is known to hide in bodily tissues even when it can’t be found in the blood, and we can hardly sacrifice humans to look for bacteria in their brains. But one small study found a way around this: Ticks can pull out the bacteria even when humans can’t find it in the blood. So researchers allowed laboratory-raised, pathogen-free ticks to feed on 26 patients with past Lyme infection and continuing symptoms. They then looked for B. burgdorferi bacteria in the bellies of the ticks, and in two cases, they found it. That’s not enough to prove that PTLDS patients are in fact being made ill by persistent infection, but it does suggest that they’re not crazy to at least consider the hypothesis.
On top of that, Lyme disease is not the only tick-borne illness. Often, patients who remain sick after treatment for Lyme disease are also battling other tick-borne infections including Babesia, Borrelia miyamotoi, and Anaplasma.* Until recently, these were nearly unheard of, so in many cases, doctors still don’t know to look for them. But they can be as bad as, or worse than, Lyme disease itself—a 2016 article in the New England Journal of Medicine reported that .38 percent of blood-donation samples were contaminated with Babesia, causing at least four deaths between 2010 and 2014. Many of these bugs are not killed off by the standard antibiotic treatment for Lyme, so even if B. burgdorferi has been eradicated, patients may be suffering from infection with something else.
Treatment is perhaps the most contentious issue of all. Self-described “Lyme-literate” doctors who will diagnose patients with chronic Lyme often treat them with repeated—or even long-term—courses of antibiotics. The mainstream position is that this is not a reasonable course of action, as four clinical trials of long-term, intravenous antibiotic treatment for PTLDS have proven that they don’t work. But a researcher who ran one of those trials says that they’ve been badly misinterpreted. Brian Fallon, a Columbia scientist who just published Conquering Lyme Disease: Science Bridges the Great Divide, reviewed all of these trials and concluded that “approximately 60 percent of patients with persistent post-treatment Lyme fatigue may experience meaningful but partial clinical improvement in fatigue with antibiotic retreatment.” The trials did conclude that there wasn’t enough evidence for a clinical recommendation for antibiotic treatment, but that was only because they studied intravenous antibiotics, and delivering drugs intravenously introduces all kinds of additional risks to the patient, which complicates the calculation around overall benefit. The next step should be to study the effectiveness of less-risky antibiotics, but because the existing studies have been interpreted as flat failures, there’s no money available for that work.
What is most frustrating about the public conversation around chronic Lyme is that it often fails to recognize that science is an iterative, imperfect process. Skeptics are quick to claim the mantle of “evidence-based medicine” without acknowledging that the evidence is ever-shifting and subject to interpretation. Above all, they often neglect to own up to how much is still not understood about Lyme—let alone recognize that this lack of knowledge is, in large part, a consequence of medicine choosing not to invest in research on this disease. The humility that is central to good scientific thinking gets replaced with scorn.
So how did Lyme disease get to be the object of such disdain? The reasons are many, as Pamela Weintraub describes in Cure Unknown: Inside the Lyme Epidemic. She points to the quirk of history that rheumatologists, rather than infectious-disease specialists, first studied the disease; the fact that many of the sickest patients turn out to fall outside of restrictive definitions even when they have substantial evidence that they have Lyme disease; and the desire for a simple story when the situation is truly complex. But there’s one additional powerful dynamic undermining attitudes toward this condition: sexism.
None of this is settled science, of course. But that’s rather the point: The skeptics act as though the science is already settled, when in actuality, patients are suffering desperately for lack of science.
Take, for example, the fact that women’s overrepresentation among chronic Lyme patients has long been used to suggest there’s no real disease to see here. In 1991, a satirical column in Annals of Internal Medicine ridiculed sufferers of “Lime disease,” which, the author wrote, shows a “very strong association with recent exposure to media stories on Lyme disease.” Rates were “highest in adults of upper middle to upper socio-economic class, with a female-to-male sex ratio of 3:1 (in contrast to the more balanced age and sex distribution of Lyme disease).” In a 2005 article, two experts worried that media coverage might “exacerbate the anxiety and misattribution that are probably at the root of much of the [PTLDS/chronic Lyme] predominantly limited to females in the Northeast.”
More recently, some skeptics have pointed to the gender imbalance among chronic Lyme patients to bolster their argument that, while PTLDS may be a real thing, most “chronic Lyme” is just the result of misdiagnosis. A 2009 article by two prominent mainstream Lyme experts noted that men and women are represented roughly equally among CDC-reported cases of Lyme disease but that patients with a chronic Lyme diagnosis are disproportionately female. They concluded, therefore, that chronic Lyme must be “unrelated to infection with B. burgdorferi” and instead consists of misdiagnoses of “illnesses with a female preponderance, such as fibromyalgia, chronic fatigue syndrome, or depression”—or simply “medically unexplained symptoms” since, they pointed out, “there is also usually a female preponderance in patients with unexplained symptoms.”
The researchers failed to imagine the possibility that there may be a biological explanation for that predominance of women among chronic Lyme patients. Others have started pursuing this only recently. (To be fair, the Lyme community is hardly alone here; sex and gender differences have long been neglected in most areas of biomedical research, perhaps particularly in infectious-disease research.) Yet we know that women’s immune systems are substantially different than men’s, which may be rooted in the fact that women have to allow another creature, a baby, to grow inside them without immune attack. This is thought to be part of the reason that women are prone to autoimmune disease and may well be relevant to the disparity in their experiences with Lyme disease. What’s more, many drugs work differently on men and women, so it’s possible that current antibiotic treatment recommendations are less effective for women, leaving them more vulnerable to long-term effects.
Women might also make up the majority of patients with a diagnosis of chronic Lyme simply because their Lyme may be less likely to meet the official diagnostic criteria for more accepted forms of the disease. Recent research suggests that the current antibody tests may be even less accurate for women. A 2010 study found that among patients with confirmed early Lyme disease, just one-third of the women, compared to half of the men, had a positive result on the CDC-approved tests. This explanation is reinforced by the fact that men are overrepresented (by as much as 2-to-1) in studies of patients with late Lyme, a diagnosis that is even stricter than PTLDS, requiring not only a positive test result but an objective clinical sign like arthritis. If women are both more likely to have chronic symptoms after being treated for early Lyme and less likely to have their late Lyme symptoms recognized because the blood tests systemically underdiagnosed them, then their overrepresentation among chronic Lyme patients isn’t a mystery—or an argument against its existence. Instead, it’s an indictment of diagnostic criteria and a treatment paradigm that appears to be letting many Lyme patients, the majority of them women, fall through the cracks.
None of this is settled science, of course. But that’s rather the point: The skeptics act as though the science is already settled, when in actuality, patients are suffering desperately for lack of science. We need better tests. We need to know if some patients are suffering from persistent infections. We need to know how the B. burgdorferi bacterium alters human immune systems. We need to understand other tick-borne infections. We need to know which antibiotics work with lowest risk. We need other treatments. We need to understand the differences in how men and women are affected by the disease.
The main reason we don’t have answers to those questions yet is that we’ve barely tried to find them. “If the same number of researchers were working on HIV as Lyme disease, we’d still have no treatment for HIV,” says John Aucott of Johns Hopkins. In 2017, the NIH spent $22 million on Lyme disease research; by contrast, Congress appropriated $1.1 billion to study and fight the Zika virus just a year after it first emerged. This lack of investment is likely to cost us dearly as climate change continues to cause ticks and their pathogens to spread: a disease that first drew attention only in a small area of Connecticut is now spreading worldwide and becoming an epidemic. And the attitude of ridicule for chronic Lyme is part of why we don’t bother to research it.
That means that ironically, those who howl that chronic Lyme is “fake” BECAUSE SCIENCE aren’t just being unscientific, they’re also impeding science. On top of that, they are attacking extremely vulnerable patients and feeding sexist stereotypes. So cut the contempt. Let’s do the science and figure this disease out.
Correction, June 27, 2018: This post originally misstated that Bartonella is another tick-borne infection that might cause Lyme-like symptoms. Recent studies suggest that disease is not transmitted via tick, and since the data seems inconclusive, it has been removed from the original list.
______________
**Comment**
Many great things about this article. Many great points.
- The 10-20% of those with “lingering symptoms” appears small in my experience. Either that, or all the people I work with just happen to fall into that category.
- Can’t speak on the “sexim” issue as in my experience men and women are both falling in the cracks with this.
- PSTLD is highly controversial. Persistent infection is proven in hundreds of studies: https://madisonarealymesupportgroup.com/2018/04/17/persistent-borrelia-infection-in-patients-with-ongoing-symptoms-of-lyme-disease/ (More links within article) http://norvect.no/230-peer-reviewed-studies-show-evidence-of-persistent-lyme-disease/, http://www.ilads.org/ilads_news/wp-content/uploads/2017/02/CLDList-ILADS.pdf (700 peer-reviewed articles showing persistence)
- The supposed “classic” EM rash will be the death of us all. Remember, many never get it at all, or it looks differently than the stringent CDC criteria, yet it continues to rule diagnosis like an iron curtain.
- So thankful for the mention that Lyme is the rock star we know by name but in fact there are 18 and counting possible diseases transmitted by ticks: https://madisonarealymesupportgroup.com/2017/07/01/one-tick-bite-could-put-you-at-risk-for-at-least-6-different-diseases/ (Please read by letter to the author for complete count)
- Science with Lyme has been horribly handled from the get-go. Fraud, collusion, and biased thinking has been the mainstay with all things Lyme. This must change.
- The article doesn’t mention another issue that has kept Lyme/MSIDS from moving forward: fraud and collusion by authorities and researchers: https://madisonarealymesupportgroup.com/2018/06/14/corruption-human-rights-violations-against-lyme-doctors-scientists-and-parents-now-on-united-nations-record/, https://madisonarealymesupportgroup.com/2017/10/13/1st-officially-recognized-report-on-violations-of-lyme-patients-human-rights-is-released-updating-borreliosis-diagnostic-codes/, https://madisonarealymesupportgroup.com/2018/03/17/nice-lyme-guidelines-human-rights-of-lyme-patients/, https://madisonarealymesupportgroup.com/2018/05/15/news-release-on-57-1-million-lyme-disease-lawsuit-filed-against-cdc/, https://madisonarealymesupportgroup.com/2017/11/15/lyme-patients-file-lawsuit-against-idsa-and-insurers-over-treatment-denials/ Suffice it to say that those in positions of authority over all things Lyme related have patents and obvious conflicts of interest on everything from test kits to vaccines.
- Doctors and researchers are standing in the way of progress: https://madisonarealymesupportgroup.com/2018/06/26/report-lyme-disease-on-rise-but-doctors-remain-skeptical/
- The correction of Bartonella NOT being a tick born disease is interesting. Everyone I work with has Bart. So one of two things is happening: 1) ticks transmit Bart 2) Lyme activates a dormant Bart infection. I’m obviously not alone in finding a prevalence of Bart in Lyme/MSIDS patients: https://madisonarealymesupportgroup.com/2018/05/07/fox-news-bartonella-is-the-new-lyme-disease/ (Many other links within this one)
- If it’s #2, Bart is not the ONLY thing Lyme/MSIDS can activate or that can be activated: https://madisonarealymesupportgroup.com/2018/06/23/the-role-of-retroviruses-in-chronic-illness-a-clinicians-perspective/, https://madisonarealymesupportgroup.com/2017/12/02/scottish-doctor-gives-insight-on-lyme-msids/, https://madisonarealymesupportgroup.com/2016/04/24/gardasil-and-bartonella/, https://madisonarealymesupportgroup.com/2018/04/25/ebv-protein-can-turn-on-genes-for-autoimmune-diseases/

