Data & Intel’s Here: Time to Cancel mRNA
https://www.thefocalpoints.com/p/we-have-the-dataits-time-to-cancel?
We Have the Data—It’s Time to Cancel mRNA
In my interview with Dr. Drew, I walk through the latest data linking COVID-19 mRNA shots to global surges in death and serious harm:
Among 184 Million Test Subjects, The Verdict Is Clear
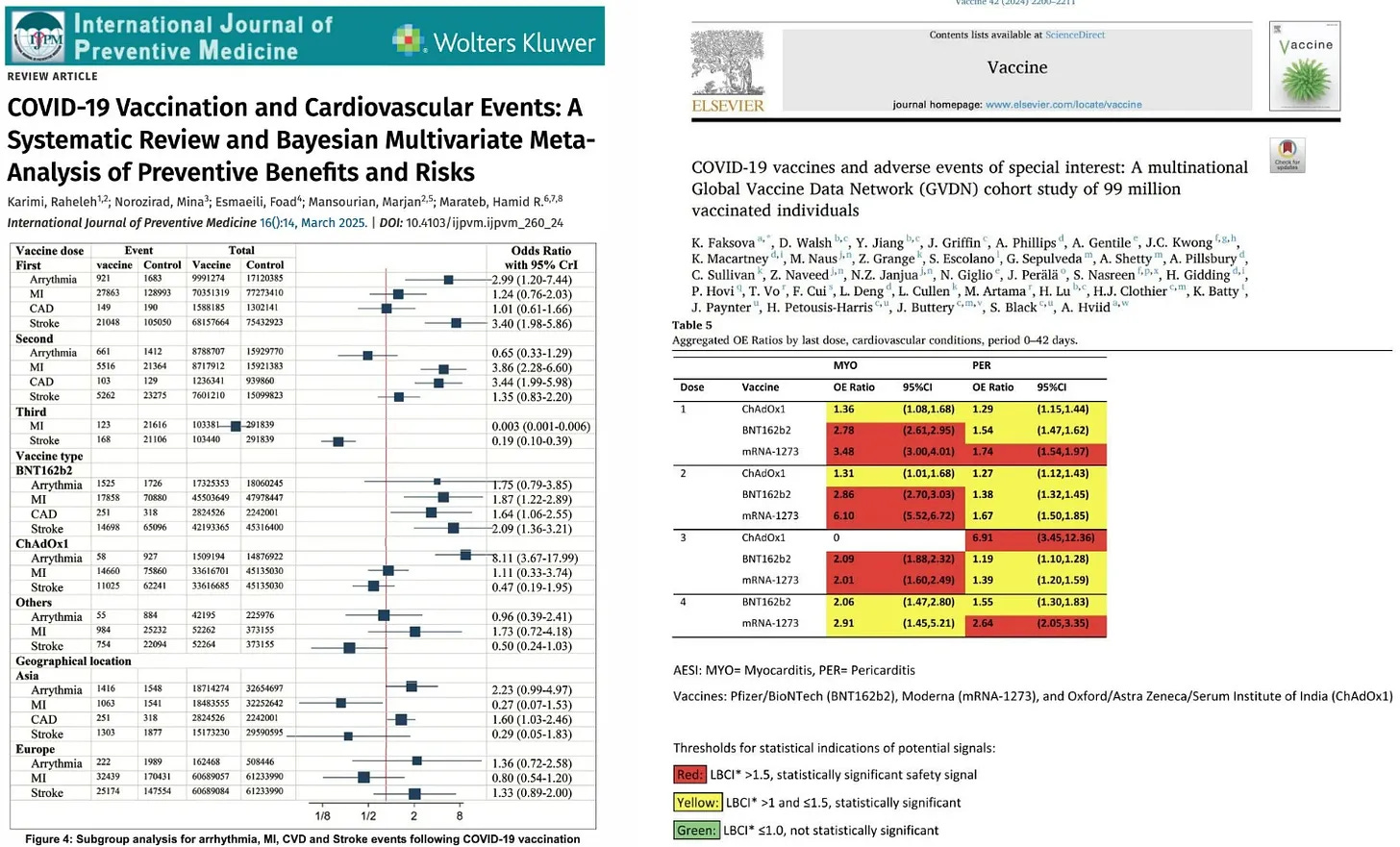
The two largest COVID-19 vaccine safety studies ever conducted, involving 99 million (Faksova et al) and 85 million people (Raheleh et al), found that mRNA injections are not safe for human use. The shots significantly increase risks of the following serious adverse events:
- Myocarditis (+510% after second dose)
- Acute Disseminated Encephalomyelitis (+278% after first dose)
- Cerebral Venous Sinus Thrombosis (+223% after first dose)
- Guillain-Barré Syndrome (+149% after first dose)
- Heart Attack (+286% after second dose)
- Stroke (+240% after first dose)
- Coronary Artery Disease (+244% after second dose)
- Cardiac Arrhythmia (+199% after first dose)
Emergency Room Visits Surge 20% Among mRNA Vaccinated Teens, Study Finds
Higher rates of emergency room and doctor visits were observed among 105,726 Pfizer mRNA vaccinated 12–18-year-olds compared to unvaccinated controls — lasting for at least 6 months after injection. If we are serious about reversing the chronic disease epidemic—now affecting over 60% of Americans—the most obvious and urgent step is to remove chronic disease-inducing injections from the market. These products are still being administered to millions of children, adolescents, adults, and the elderly every year.
COVID-19 mRNA Injection Spike Protein Expressed in Cerebral Arteries of Stroke Patients for Up to 17 Months
Vaccine mRNA and Spike protein found in hemorrhagic stroke patients’ brains — confirming human biodistribution to vital organs.
WHO Data Reveals Global COVID-19 Deaths Skyrocketed After Mass Vaccination
New study finds that mass COVID-19 vaccination not only failed, but made things worse — with the highest death surges in the most heavily vaccinated populations.
Catastrophic Neurological and Psychiatric Damage from COVID-19 Vaccines
Based on multiple studies, COVID-19 vaccines seriously damage the neurological system and devastate mental health. They increase your risk of:
- Alzheimer’s (+22.5%)
- Cognitive impairment (+137.7%)
- Ischemic stroke (+44%)
- Hemorrhagic stroke (+50%)
- Transient ischemic attack (+67%)
- Myelitis (+165%)
- Myasthenia gravis (+71%)
- Depression (+68.3%)
- Anxiety disorders (+43.9%)
- Sleep disorders (+93.4%)
(See link for article, studies, and video)
_______________
Government Admits it Knew Covid Shots Were Fraud
Karen Kingston is a biotech analyst and former Pfizer employee who is back with some grotesque news about what the US government knew about the CV19 bioweapon vax. They knew it was not safe at all, and the FDA also knew Pfizer committed fraud to get the CV19 injections approved. Kingston says, “This is the government’s words exactly: ‘The FDA was aware of the protocol violations.’ So, the FDA was aware of the fraud that was reported . . . before it granted emergency use authorization (EUA) for its vaccine. They were aware of the fraud. Second, the government said it ‘had continued access’ to the Pfizer vaccine clinical data, and ‘in the FDA’s view, Pfizer’s vaccine is effective.’ Notice they dropped the word ‘safe.’ The minimum bar is safe before effective, but they intentionally dropped the word safe. . . . They ignored safety.
Kingston says, “In 2020, they met and listed out Myocarditis. Pericarditis, neurological malfunctions, respiratory failure, multiple system inflammatory disease, Guillain-Barré syndrome, and they listed everything out except for cancer. So, they knew the CV19 vax would cause all those debilitating injuries, infertility and death.
Kingston points out they want to put so-called mRNA in everything to fight cancer, but all the studies for the past several decades on mRNA say it causes cancer. Kingston says:
“Pfizer is telling us we are putting in faulty genes. We are debilitating you. We are disabling you. We are sterilizing you, and we are killing you. We are directing the evolution of human beings to become more weak and more dependent on us. . . . To survive, you will need us. It’s on their website. It’s called ‘directed evolution.’ They are directing the extinction of our species. That is what this is. They are playing God. . . .You can call it eugenics. You can call it depopulation, but the new word is ‘directed evolution.’ It’s mRNA technology or personalized medicine, it’s all the same thing.”
(Go to link for article and interview)
_______________
**Comment**
Kingston came out early that the COVD clot shots are bioweapons. She hasn’t changed her tune but has in fact been continuously outspoken. The attorney for another whistleblower, Brook Jackson, revealed that Pfizer argued the court should dismiss her lawsuit alleging fraud in Pfizer’s COVID clinical trials because the government knew about the fraud but continued to do business with them.
None of this matters to the hopelessly irredeemable CDC (and government) which is set to recommend MORE mRNA shots this year despite a minimum 35% increase in 1-year all-cause mortality (at least for the Pfizer shot), and FIVE recent papers showing the COVID shot harms outweigh any supposed benefits.
Oh AND……
Covid mRNA ‘Vaccines’ Caused ‘Alarming’ Surge in Violent Behavior, Homicidal Ideation
https://www.preprints.org/manuscript/202504.1099/v1
This version is not peer-reviewed.
Submitted: 11 April 2025
Posted: 14 April 2025
Big Pharma Throws Fit
May 6, 20205
Dr. Dhand reports that Big Pharma and researchers obtaining government grants are panicking due to fears of HHS daring to collect information about funding for research into mRNA technology.
Any research utilizing public funds should have oversight about funding information!
But, true to form Big Pharma and these deluded researchers are making this political by stating that Trump-appointed officials are being driven by misinformation and conspiracy theories.
Demonstrating the complete lunacy, these researchers completely ignore the body of mRNA research which was originally abandoned by its creator (Robert Malone) due to being a dead end as well as for health concerns, which now include: infertility, fetal loss, maternal death rates, excess deaths, organ damage, autoimmunity, myocarditis, and cancer.
Please remember that the CDC changed the definition of a ‘vaccine’ so mRNA would fit in the category. It is asinine to expect an mRNA platform to work like a traditional vaccine, and it’s purposely called a platform for drug delivery because new drugs are needed for variants, creating a endless market.
Dr. Dhand states that one of the best things he ever did for his health was to refuse the clot shots. He states he will continue refuse any mRNA product. He’s not alone:
“I Have Absolute Faith That mRNA Vaccines Will Kill You” ~ Dr. Sucharit Bhakdi:
For more:
- https://madisonarealymesupportgroup.com/2023/03/31/mrna-platform-what-it-is-what-it-means/
- https://madisonarealymesupportgroup.com/2023/06/09/mrna-will-be-everywhere/
- https://madisonarealymesupportgroup.com/2023/03/03/animals-injected-with-mrna-technology-hardly-anyone-knows-about-it/
- https://madisonarealymesupportgroup.com/2023/04/07/mrna-gene-therapy-coming-to-the-food-supply-this-month-china-loads-milk-with-mrna-exosomes-successfully-immunize-mice/
- https://madisonarealymesupportgroup.com/2023/04/18/gene-therapied-pork/
- https://madisonarealymesupportgroup.com/2023/05/19/biowarfare-through-the-food-supply/
- https://madisonarealymesupportgroup.com/2025/02/04/treatment-recovery-of-mrna-shot-injury/
- https://madisonarealymesupportgroup.com/2023/01/11/covid-gene-therapy-injections-developed-by-u-s-military-are-called-counter-measures-were-ordered-as-prototypes/