California’s First CDC-Confirmed Case of Borrelia Miyamotoi
https://www.lymedisease.org/californias-first-cdc-confirmed-case-of-borrelia-miyamotoi/
California’s first CDC-confirmed case of Borrelia miyamotoi

By Lonnie Marcum
May 4, 2023
A recent case reminds us that Lyme disease isn’t the only tick-borne disease we need to worry about.
Last year, the CDC confirmed California’s first known case of Borrelia miyamotoi—a tick-borne pathogen that causes a relapsing-fever illness in humans.
This discovery highlights the need for increased awareness and surveillance of emerging tick-borne illnesses across the United States.
In this case, a man from Marin County, California, sought care at a neurology clinic in San Francisco. His symptoms included recurring fever, night sweats, mild vision changes and nausea. The fevers typically lasted one day and would recur every 10-14 days. At the time, he was also undergoing monoclonal antibody therapy for multiple sclerosis.
His standard blood work was negative for fungi, Lyme disease, brucellosis and leptospirosis. Chest x-rays and abdominal CT scans were negative as well.
The only notable blood findings were a positive antigen for Epstein-Barr virus, a low platelet count (thrombocytopenia), an elevated C-reactive protein (an inflammatory marker), and an elevated procalcitonin—a biomarker that is released in response to bacterial infections.
Specialty lab testing
Considering the patient’s immunocompromised status and continued relapsing fevers, his blood was sent to a specialty lab for next-generation DNA sequencing. The specialty lab, Karius, says it can identify over 1000 clinically relevant pathogens including bacteria, DNA viruses, fungi, and parasites from a single blood sample.
The DNA test results came back positive for Borrelia miyamotoi and were sent to the CDC for confirmation. The CDC confirmed the patient’s blood was positive for Borrelia miyamotoi and 100% identical to an isolate that had been previously collected from an Ixodes pacificus tick in Marin County. This indicates the patient acquired the infection in California.
Borrelia miyamotoi, first identified in Japan in 1995, is considered an emerging infectious disease in Asia, Europe and the United States.
A recent study found widespread evidence of Borrelia miyamotoi in human blood samples of people living in the northeastern United States. An earlier study found evidence of tick-borne relapsing fever (TBRF) Borrelia, including Borrelia miyamotoi in the blood of 26 out of 101 samples of residents of Mendocino County, California in the 1980s.
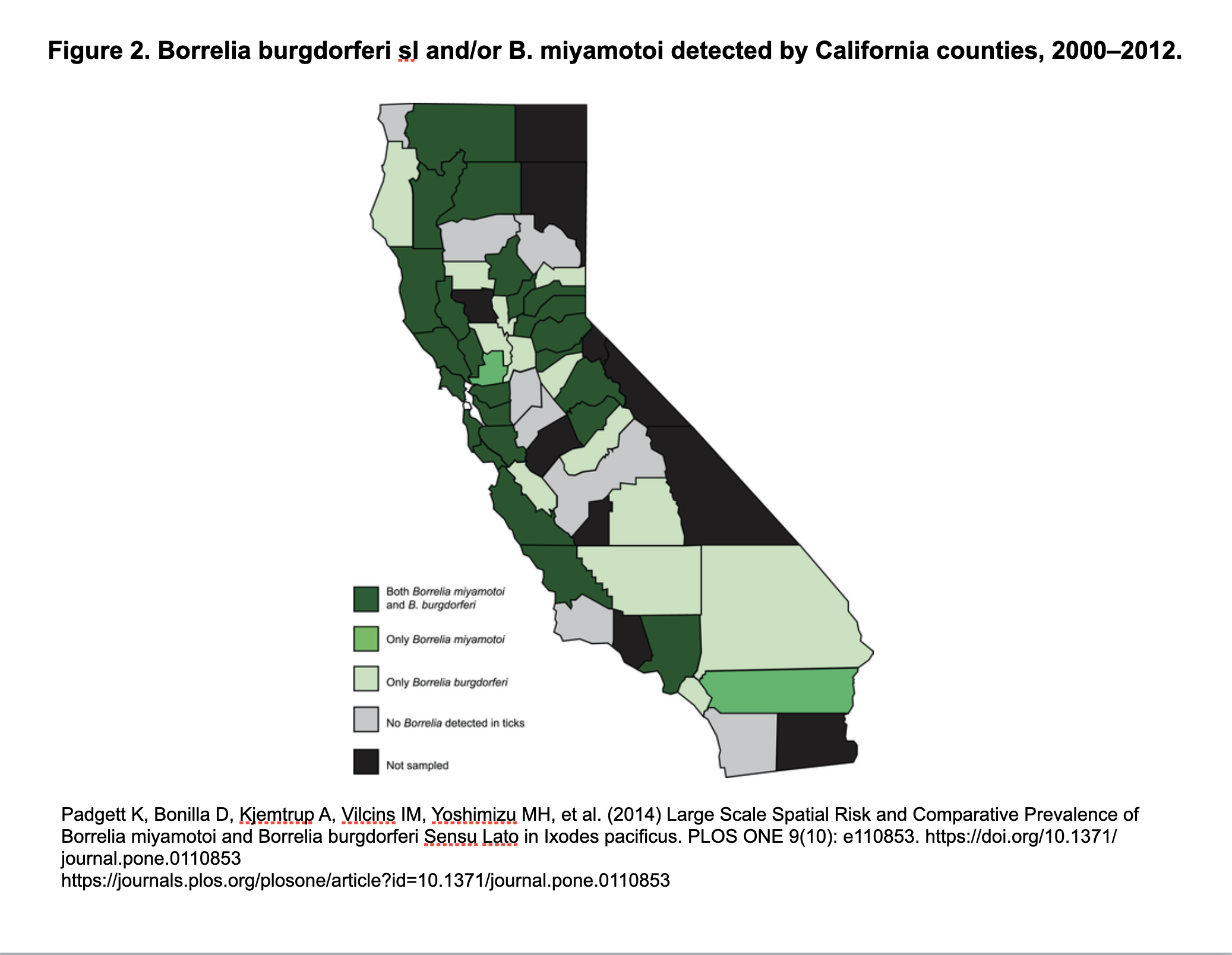
Another study found multiple species of relapsing fever Borrelia in blood samples drawn from patients in 16 out of 24 California counties. And a 13-year-long study found Borrelia miyamotoi in ticks found in 24 out of 48 counties in California (see map below).
Borrelia miyamotoi is transmitted to humans through the bite of infected blacklegged ticks. These are the same hardbodied ticks (Ixodes scapularis, Ixodes pacificus) that transmit Lyme disease to humans and animals. Other types of North American tick-borne relapsing fever Borrelia (B. hermsii, B. turicatae, B. parkeri), are transmitted by soft-bodied ticks.
The symptoms of Borrelia miyamotoi disease are similar to those of other tick-borne illnesses, such as Lyme disease. But standard Lyme tests will be negative, making the diagnosis challenging.
TBRF
According to the CDC, the main symptoms of TBRF are high fever, headache, muscle and joint pain. Fewer than 1 in 10 patients will develop a rash. Left untreated, the symptoms typically repeat, producing a telltale pattern of relapsing fever lasting 1-3 days, followed by 7-10 days without a fever, followed by another 1-3 days of fever.
The CDC website says: “Confirmation of a diagnosis relies on 1) the use of polymerase chain reaction (PCR) tests that detect DNA from the organism or 2) antibody-based tests. Both types of tests are under development and not widely commercially available but can be ordered from a limited number of CLIA-approved laboratories.”
Treatment for TBRF involves the use of antibiotics, such as doxycycline, amoxicillin or cefuroxime . In this case the man was given a 4-week course of doxycycline and achieved complete resolution of his symptoms. One month after completing antibiotics ,follow-up laboratory testing showed complete resolution of thrombocytopenia and normalization of inflammatory markers.
All tick-borne diseases are a significant health concern worldwide, particularly in areas where ticks are prevalent. These illnesses can present with a range of symptoms, some of which can be mysterious and difficult to diagnose.
While relapsing fever Borrelia has been detected in California before, this is the first CDC-confirmed case of Borrelia miyamotoi in California. This case highlights the need for continued education and awareness of tick-borne diseases.
As with all tick-borne illnesses, prevention is key. To reduce the risk of tick bites, take precautions when spending time outdoors, such as pre-treating shoes and clothing with permethrin, using insect repellant on yourself, your children and your pets, and performing thorough tick checks after being outdoors.
LymeSci is written by Lonnie Marcum, a Licensed Physical Therapist and mother of a daughter with Lyme. She served two terms on a subcommittee of the federal Tick-Borne Disease Working Group. Follow her on Twitter: @LonnieRhea Email her at: lmarcum@lymedisease.org.
Reference
Rubio LA, Kjemtrup AM, Marx GE, Cronan S, Kilonzo C, Saunders MEM, et al. Borrelia miyamotoi infection in immunocompromised man, California, USA, 2021. Emerg Infect Dis. 2023 May https://doi.org/10.3201/eid2905.221638 DOI: 10.3201/eid2905.221638
Padgett K, Bonilla D, Kjemtrup A, Vilcins I-M, Yoshimizu MH, Hui L, et al. (2014) Large Scale Spatial Risk and Comparative Prevalence of Borrelia miyamotoi and Borrelia burgdorferi Sensu Lato in Ixodes pacificus. PLoS ONE 9(10): e110853. https://doi.org/10.1371/journal.pone.0110853
Additional Resources
Stanford: Tick-borne disease risk high in SF Bay Area
Yale: Tick-borne Borrelia miyamotoi widespread in northeastern US
LYME SCI: Infected ticks in California? It’s complicated.
LYME SCI: B. miyamotoi has been in California ticks for a long time
LYME SCI: Lyme-carrying ticks in West differ from their Eastern cousins
LYME SCI: How many “negative” Lyme tests are due to B. miyamotoi?
LYME SCI: Tick infection rates as high as 31% in some coastal areas of California
BALF: New interactive maps show where citizen scientists found infected ticks
For more:
- https://madisonarealymesupportgroup.com/2020/11/18/what-you-need-to-know-about-borrelia-miyamotoi/
- https://madisonarealymesupportgroup.com/2017/07/18/transmission-time-for-borrelia-mayonii-by-nymphal-ticks-mouse-model/
- https://madisonarealymesupportgroup.com/2020/06/17/borrelia-miyamotoi-infection-in-a-highly-endemic-area-of-lyme-disease/
- https://madisonarealymesupportgroup.com/2020/10/24/a-case-of-borrelia-miyamotoi/
And the question begging to be asked is: how many people with B. miyamotoi are falling through the cracks? It isn’t even reportable to the CDC yet (which notoriously undercounts all things tick-borne-related).
For more: https://igenex.com/tick-talk/what-you-need-to-know-about-borrelia-miyamotoi/
This article points out the confusion with B. miyamotoi:
- many separate it from other tick-borne relapsing fevers
- while it can cause relapsing fevers, it sometimes doesn’t
- it appears to be the only TBRF transmitted from a hard bodied tick, unlike TBRF which is mainly transmitted from a soft bodied tick (I remain skeptical of this as ticks have repeatedly been found to transmit things they shouldn’t – just like they are found in places they shouldn’t be.)
- symptoms often resemble Lyme disease
- you can be infected with BOTH B. miyamotoi AND Lyme disease (as well as numerous other coinfections) which will complicate symptom presentation
- testing for B. miyamotoi is just as abysmal as it is for Lyme/MSIDS: https://madisonarealymesupportgroup.com/2020/03/01/study-cdcs-2-tier-lyme-testing-inaccurate-in-more-than-70-of-cases/