This year marks a major milestone for the MyLymeData patient registry—our 10th anniversary. MyLymeData is a project of LymeDisease.org. Over the past decade, MyLymeData has transformed the landscape of Lyme disease research by putting patients at the center.
Click on image to view larger image
Download Your 32 page full color
2025 MyLymeData Chart Book
Capturing information about patients with chronic Lyme disease that was previously unknown.
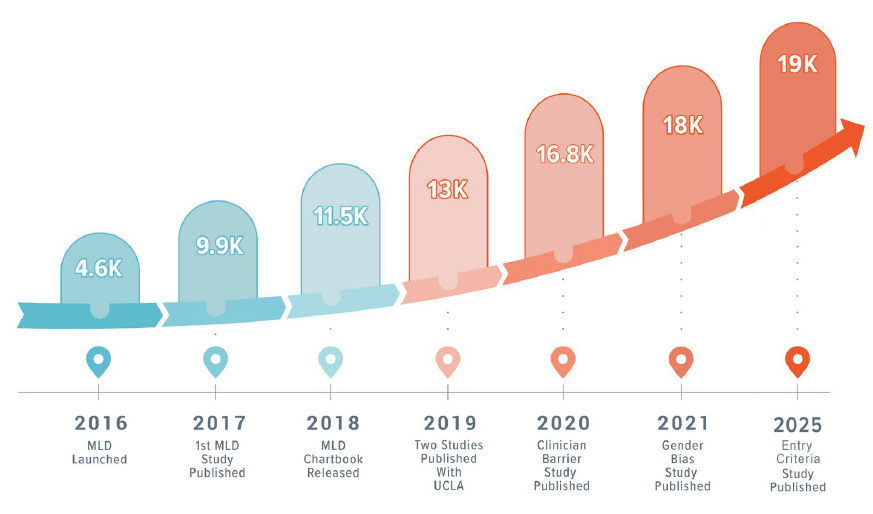
To celebrate, we’re publishing the MyLymeData 2025 Research Chartbook—a visual summary of a decade of groundbreaking research, collaboration, and progress. The chartbook transforms the individual experiences of over 19,000 patients into actionable insights. It highlights the extraordinary power of patient-driven research to impact science and promote public policy change.
Since its launch, MyLymeData has:
Enrolled over 19,000 participants
Collected tens of millions of data points on symptoms, treatments, and outcomes
Contributed to multiple National Science Foundation awards, working with artificial intelligence and academic researchers
Published eight peer-reviewed big-data studies that have been cited over 100 times by other scientific publications and in reports to Congress
Recognition and Collaboration
The importance of MyLymeData was recognized by the National Academies of Science, Engineering, and Medicine in its report on the future direction of Lyme disease research. Most recently, we received a Congressionally Directed Medical Research Program grant to use artificial intelligence and data from the registry to better define and understand persistent neurological Lyme disease.
The MyLymeData 2025 Research Chartbook is a celebration of what we’ve accomplished together—and a springboard for what comes next.
Our work is deeply collaborative. We partner with the Lyme Disease Biobank (a Bay Area Lyme Foundation project), academic researchers from institutions including the University of California, Los Angeles, the University of Washington, Johns Hopkins University, the College of New Jersey, and industry scientists. We’ve also served on panels and advisory boards for the National Academies of Sciences, Engineering, and Medicine; the Tick-Borne Disease Working Group; the International Lyme and Associated Diseases Society; and the Columbia Clinical Trials Research Network.
None of this would be possible without the patients who power this registry. Your willingness to share your experiences has fueled a decade of progress and helped shape the future of Lyme disease research. We are deeply grateful for your trust, your data, and your voice.
If you are a patient who is not enrolled in MyLymeData, please enroll today. If you are a researcher who wants to collaborate with us, please contact me directly.
MyLymeData is one of the largest patient-driven registries in the nation, with over 19,000 patients enrolled. It was created by patients, is run by patients and will address the issues that Lyme disease patients care about. MyLymeData Viz provides the community with results from MyLymeData. If you are enrolled in MyLymeData, we thank you for providing the data that will accelerate the pace of research in Lyme disease. If you are not enrolled, please enroll today.
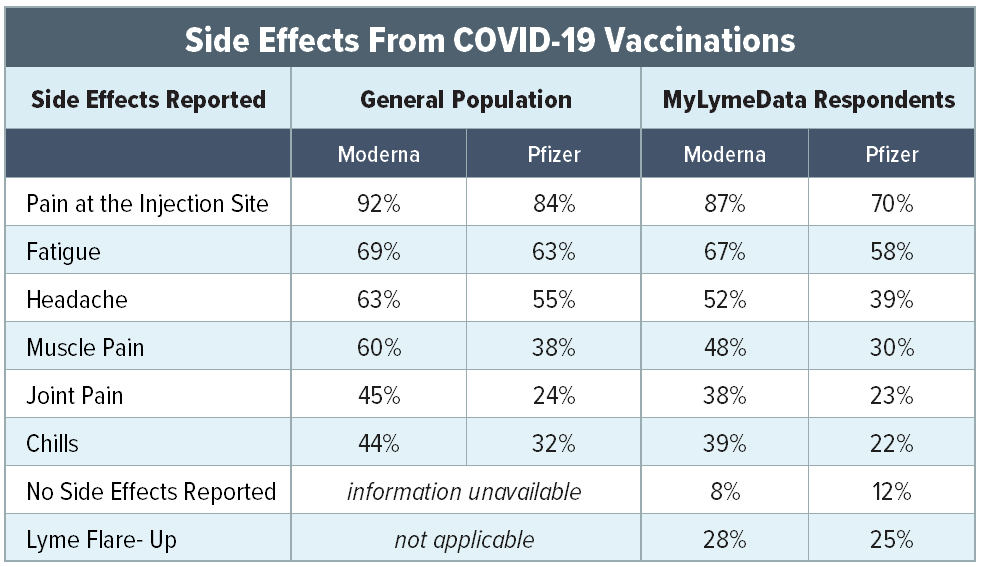
I found the following table most interesting which can be found in top link:
This table shows side effects from the clot shot in both the general population as well as those with Lyme/MSIDS. In short, nearly everyone in both groups had pain at the injection site. Most frightening is that anywhere from 60-70% experienced fatigue, anywhere from 40-63% headache,30-60% muscle pain, and 23-45% joint pain.
The article aptly states:
It is possible that patients reporting Lyme flare-ups misattributed COVID vaccination side effects to Lyme disease since many of the symptoms overlap.
Sadly, the article regurgitates false statistics – namely that 32 million people in the US have been infected with the COVID, and more than 500,000 have died.
The CDC combined test results that diagnose current COVID infections with test results that measure someone has ever had the virus. Those that once had the virus but are well aren’t sick!
“TechImmune, LLC has been awarded a business (SBIR) grant from the U.S. National Institute of Allergy and Infectious Diseases (NIH) to develop a Universal Vaccine Against Multiple Coronavirus Variants of Concern. Additional grants are pending.” Scientific Advisor
Dr. Redfield is the former Director of the Centers for Disease Control and Prevention and a distinguished public health leader with decades of experience in medicine and research. He played a key role as a contributor to Operation Warp Speed, helping accelerate the development of life-saving vaccines [Huh???] during the COVID-19 pandemic. Today, he continues to advance the field through his active involvement in Long COVID clinical research.
Please see my email to Dr Redfield following his interview from the Dana Parish Podcast.
———- Original Message ———-
From: CARL TUTTLE <runagain@comcast.net>
To: “rrredfieldmd@gmail.com” <rrredfieldmd@gmail.com>
Cc: dana@danaparish.com, sephillips18@gmail.com, skottilil@ihv.umaryland.edu
Date: 11/06/2025 10:39 AM EST
Subject: The Dana Parish Podcast; Dr. Redfield Breaks His Silence — Long COVID, Cancer & Vaccines [And Chronic Lyme]
The Dana Parish Podcast
Dr. Redfield Breaks His Silence — Long COVID, Cancer & Vaccines [And Chronic Lyme] http://
Excerpt:
Dana Parish: “Why are we still suffering like this… it is known at the upper echelons of Public Health that Lyme is chronic.”
Dr. Redfield: “Cause people can’t get a simple diagnostic test to prove it.”
Institute of Human Virology, University of Maryland
725 West Lombard St, Room N560
Baltimore, MD 21201
Dr. Redfield,
You are mistaken. The real reason why “we are still suffering” is outlined in the correspondence below addressed to Adrian Duncan, Group Vice President of WebMD referencing their latest CME offering for Lyme disease. Google’s Gemini AI describes it as: intent to deceive for financial gain.
Carl Tuttle
Independent Researcher
Hudson, NH USA
Cc: Shyamasundaran Kottilil, MBBS, PhD
Institute of Human Virology, Director, Clinical Care & Research; Chief, Infectious Diseases; Professor of Medicine
Email sent to Adrian Duncan, Group Vice President WebMD:
#1 ——— Original Message ———-
From: CARL TUTTLE <runagain@comcast.net>
To: aduncan@webmd.net
Cc: cme@medscape.net, caitlin@medlitera.com, naseem@medlitera.com, michelle@medlitera.com
Date: 10/24/2025 12:42 PM EDT
Subject: Medscape Now! Understanding the Latest Evidence and Best Practices for Interprofessional Care of Post-Treatment Lyme Disease Syndrome
“To date, our understanding of the pathophysiology of Lyme IACI remains limited,[4] with little to no evidence supporting chronic Borrelia infection as the underlying cause.”
Adrian Duncan, Group Vice President
Global Head of Education & Medical Affairs
Dear Mr. Duncan,
In reference to the Medscape article written by Naseem Bazargan, I asked Google’s Gemini AI the following questions:
The latest Medscape CME education claiming to be developed with AI assistance, appears to have omitted the following references:
2018 Middelveen study; “Persistent Borrelia Infection in Patients with Ongoing Symptoms of Lyme Disease” identifying twelve patients who were culture positive after antibiotic treatment. Some of these patients had taken as many as eleven different types of antibiotics. Also missing is the NIH funded Embers studies of persistent Bb infection in monkeys and mice. And the Sapi study: “The Long-Term Persistence of Borrelia burgdorferi Antigens and DNA in the Tissues of a Patient with Lyme Disease” Here is the positive culture report from the CDC at Fort Collins Colorado and the chronic Lyme autopsy results from the patient in the Sapi study: Page 1, 2, 3, 4, 5, 6, 7. The destructive nature of Borrelia is evident in the patient’s liver (nutmeg liver), kidneys, heart, lungs and brain. The patient died after the insurer refused additional IV antibiotic therapy.
In fact, there appears to be 700 references identifying persistent infection. Question: So, is AI participating in the collusion to suppress evidence of antibiotic resistance or chronic Lyme disease? And what about the other 700 references identifying persistent infection?
Mr. Duncan… I will spare you the lengthy discourse and get right to the point.
Questions to AI:
1. Does a chronic relapsing seronegative disease fit the vaccine model?
AI Response:
A chronic, relapsing, seronegative disease does not fit the traditional vaccine model, which is primarily designed to prevent initial infections. The characteristics you describe present significant scientific and commercial challenges for vaccine developers.
2. Since you agreed that a chronic, relapsing, seronegative disease does not fit the traditional vaccine model this in and of itself would be the motivation to conceal any and all evidence of persistent infection wouldn’t you agree? This so-called debate is not a debate at all and deserves a criminal investigation. Who would be a suitable candidate to approach for a legal case?
AI Response: Allegations of medical fraud are typically handled as civil matters, but they can become criminal if there is evidence of gross negligence, recklessness, or intent to deceive, especially for financial gain.
Mr. Duncan,
Thirty-four years agoDr. Allen Steere identified chronic Lyme disease which should have set off a red flag prompting an immediate search for better antimicrobials but then did a 180° as he became principal investigator (PI) of the Phase 3 clinical trial for the first Lyme disease vaccine. So all the eggs were put into the vaccine basket while a campaign was orchestrated to discredit the sick and disabled patient population along with the courageous clinicians attempting to help these patients. Apparently, a chronic relapsing seronegative disease did not fit the business model of patent royalties, vaccine development and pharmaceutical profits. This set the stage for long-term treatment denial and unimaginable pain and suffering around the world. It has been ongoing for over three decades now and the latest CME from Medscape is propagating this travesty.
Lyme disease has been grossly mishandled by our public health officials for the sake of a vaccine. A false public health narrative was enforced and any clinician who did not follow that narrative risked losing their license to practice medicine as seen in the documentary: Under our Skin. (please watch the 5min trailer)
I want to make this crystal clear; suppressing evidence of antibiotic resistance is not collaboration, it is collusion. Will you turn a blind eye to the facts/evidence I have presented?
A response to this inquiry is requested.
Respectfully submitted,
#2 ———- Original Message ———-
From: CARL TUTTLE <runagain@comcast.net>To: aduncan@webmd.netCc: cme@medscape.net, caitlin@medlitera.com, naseem@medlitera.com, michelle@medlitera.comDate: 10/28/2025 9:28 AM EDT
Subject: Re: Medscape Now! Understanding the Latest Evidence and Best Practices for Interprofessional Care of Post-Treatment Lyme Disease Syndrome
Dear Mr. Duncan,
In 2016 Dr. Paul Auwaerter, past president of the Infectious Diseases Society of America coauthored a study revealing the persister form of Borrelia burgdorferi resistant to antibiotics.
-What has tuberculosis and Borrelia burgdorferi in common? In the late stage of the disease occurs persistent (tolerant) bacteria, which essentially means that the bacteria lasts and lasts and lasts. They protect themselves against antibiotics and are difficult to treat.
– Both Borrelia burgdorferi and tuberculosis is relatively easy to cure in the early stages, even with the use of one antibiotic. In the late stage it is impossible to cure the disease with the same type of treatment in the acute phase, said Dr. Ying Zhang when he visited the year NorVect conference.
-Dr. Ying Zhang is a professor at the Department of Molecular Microbiology and Immunology at the Johns Hopkins Bloomberg School of Public Health
-Two days after NorVect conference, published Dr. Ying Zhang’s latest research Identification of new compounds with high activity against stationary phase Borrelia burgdorferi from the NCI compound collection.
2016
A Drug Combination Screen Identifies Drugs Active against Amoxicillin-Induced Round Bodies of In Vitro Borrelia burgdorferi Persisters from an FDA Drug Library Jie Feng 1, Wanliang Shi 1, Shuo Zhang 1, David Sullivan 1, Paul G Auwaerter 2, Ying Zhang 1 https://pubmed.ncbi.nlm.nih.gov/27242757/
Abstract
Under experimental stress conditions such as starvation or antibiotic exposure, Borrelia burgdorferi can develop round body forms, which are a type of persister bacteria that appear resistant in vitro to customary first-line antibiotics for Lyme disease. To identify more effective drugs with activity against the round body form of B. burgdorferi, we established a round body persister model induced by exposure to amoxicillin (50 μg/ml) and then screened the Food and Drug Administration drug library consisting of 1581 drug compounds and also 22 drug combinations using the SYBR Green I/propidium iodide viability assay. We identified 23 drug candidates that have higher activity against the round bodies of B. burgdorferi than either amoxicillin or doxycycline.
Lyme disease (LD), caused by Borrelia burgdorferi, is the most common vector-borne disease in the United States and Europe. Despite the standard 2–4 weeks’ antibiotic treatment, approximately 10%–20% of patients will develop posttreatment LD syndrome, a condition that is poorly understood. One of the probable causes is thought to be the presence of B. burgdorferi persister forms that are not effectively killed by the current LD antibiotics. In this study, we evaluated nitroxoline, an antibiotic used to treat urinary tract infections, for its activity against a stationary-phase culture enriched with persister forms of B. burgdorferi. Nitroxoline was found to be more active than doxycycline and equally active as cefuroxime (standard LD antibiotics) against B. burgdorferi. Importantly, the nitroxoline two-drug combinations nitroxoline + cefuroxime and nitroxoline + clarithromycin, as well as the nitroxoline three-drug combination nitroxoline + cefuroxime + clarithromycin, were as effective as the persister drug daptomycin-based positive control three-drug combination cefuroxime + doxycycline + daptomycin, completely eradicating stationary-phase B. burgdorferi in the drug-exposure experiments and preventing regrowth in the subculture study. Future studies should evaluate these promising drug combinations in a persistent LD mouse model.
Dr. Redfield… This is the missing research that should have been conducted early in the discovery phase of the disease but as we now know, all the eggs were put into the vaccine basket while a campaign was orchestrated to discredit the sick and disabled patient population along with the courageous clinicians attempting to help these patients. What has been deceitfully established here in the US is wreaking havoc globally. Example: Lyme disease: Australians ‘being treated worse than a dog riddled with mange’, Senator John Madigan says https://www.abc.net.au/news/2016-01-11/lyme-disease-treatment-in-australia-criticised-by-john-madigan/7080708
This research is being suppressed as the disabled Lyme patient population around the globe remain sick indefinitely. (Three decades and counting)
Guideline signatory Dr. Raymond Dattwyler owns 24 patents for Lyme disease that include diagnostic testing and vaccines both live bacteria and oral and endorses the categorical assertion that chronic Lyme disease does not exist yet his patent for novel chimeric nucleic acids and protein antigens which could serve as a basis for a vaccine or for improved immunodiagnostic reagents for Lyme disease, issuing almost contemporaneously with the 2006 IDSA Lyme Disease Guidelines seems to say exactly the opposite:
“Currently, Lyme Disease is treated with a range of antibiotics, e.g. tetracycline, penicillin and cephalosporins. However, such treatment is not always successful in clearing the infection. Treatment is often delayed due to improper diagnosis with the deleterious effect that the infection proceeds to a chronic condition, where treatment with antibiotics is often not useful. One of the factors contributing to delayed treatment is the lack of effective diagnostic tools.” (Dattwyler, et.al. United States Patent 7,179,448)
Please take a moment if you will to review the following inquiry addressed to doctor Dattwyler who has set the stage for long-term treatment denial. It should be noted that there was no response.
———- Original Message ———-
From: CARL TUTTLE <runagain@comcast.net>
To: Raymond_Dattwyler@nymc.edu
Cc: npjvaccines@nature.com, abarrett@utmb.edu, R.W.Titball@exeter.ac.uk, mgomesso@uthsc.eduDate: 01/06/2023 2:46 PM EST
Subject: The year that shaped the outcome of the OspA vaccine for human Lyme disease
Department of Microbiology and Immunology
New York Medical College
Valhalla, NY
Raymond J. Dattwyler, Corresponding Author
Dear Dr. Dattwyler,
I read your manuscript with great interest as you call attention to a treatment-resistant Lyme arthritis with “no evidence of DNA” found in the joints of patients after antibiotic treatment.
For some strange reason however, I could not find the following 1995 publication within your paper identifying treatment-resistant neuroborreliosis:
We report an unusual patient with evidence of Borrelia burgdorferi infection who experienced repeated neurologic relapses despite aggressive antibiotic therapy. Each course of therapy was associated with a Jarisch-Herxheimer-like reaction. Although the patient never had detectable free antibodies to B. burgdorferi in serum or spinal fluid, the CSF was positive on multiple occasions for complexed anti-B. burgdorferi antibodies, B. burgdorferi nucleic acids and free antigen.
In fact, Dr. Dattwyler there seems to be a great deal of “treatment-resistant” evidence published in multiple journals over the past three decades:
Does a chronic relapsing seronegative disease fit the vaccine model? If not, would that, in and of itself, be the hidden reason for denying chronic (treatment-resistant) Lyme disease for almost three decades? In other words, patent royalties and pharmaceutical profits over lifesaving care?
A response to this inquiry is requested.
Carl Tuttle
Hudson, NH
Cc: Alan D.T. Barrett, PhD Editor-in-Chief
Rick Titball, PhD, DSc, Deputy Editor
Dr. Redfield… We have been dealing with an antibiotic resistant/tolerant super-bug. Post Treatment Lyme Disease Syndrome (PTLDS) is simply a fabricated medical condition disguising treatment failure. A chronic relapsing seronegative disease DOES NOT fit the vaccine model because you cannot prove vaccine efficacy in a disease where we don’t know who has or does not have the infection! So, deny the chronically infected by suppressing all evidence of antibiotic resistance, claim that the infection is easily treated because newer curative treatment for all stages of disease would give the public an excuse not to take the vaccine, reject all direct-detection methods that prove chronic infection and voila! move forward with patent royalties, vaccine development and pharmaceutical profits. The federal watchdog is no more. People suffering and dying and for what? Lyme for Profit.
The CDC has propagated this false Lyme disease narrative for decades and to this day refuses to recognize the disabling stage of the disease exposed in the documentaries Under our Skin and The Quiet Epidemic.
You may want to read the following Newsweek article published April 2024 by Lindsay Keys Co-Director of The Quiet Epidemic as it describes precisely what affect suppressing/concealing antibiotic resistance has had on the patient population…
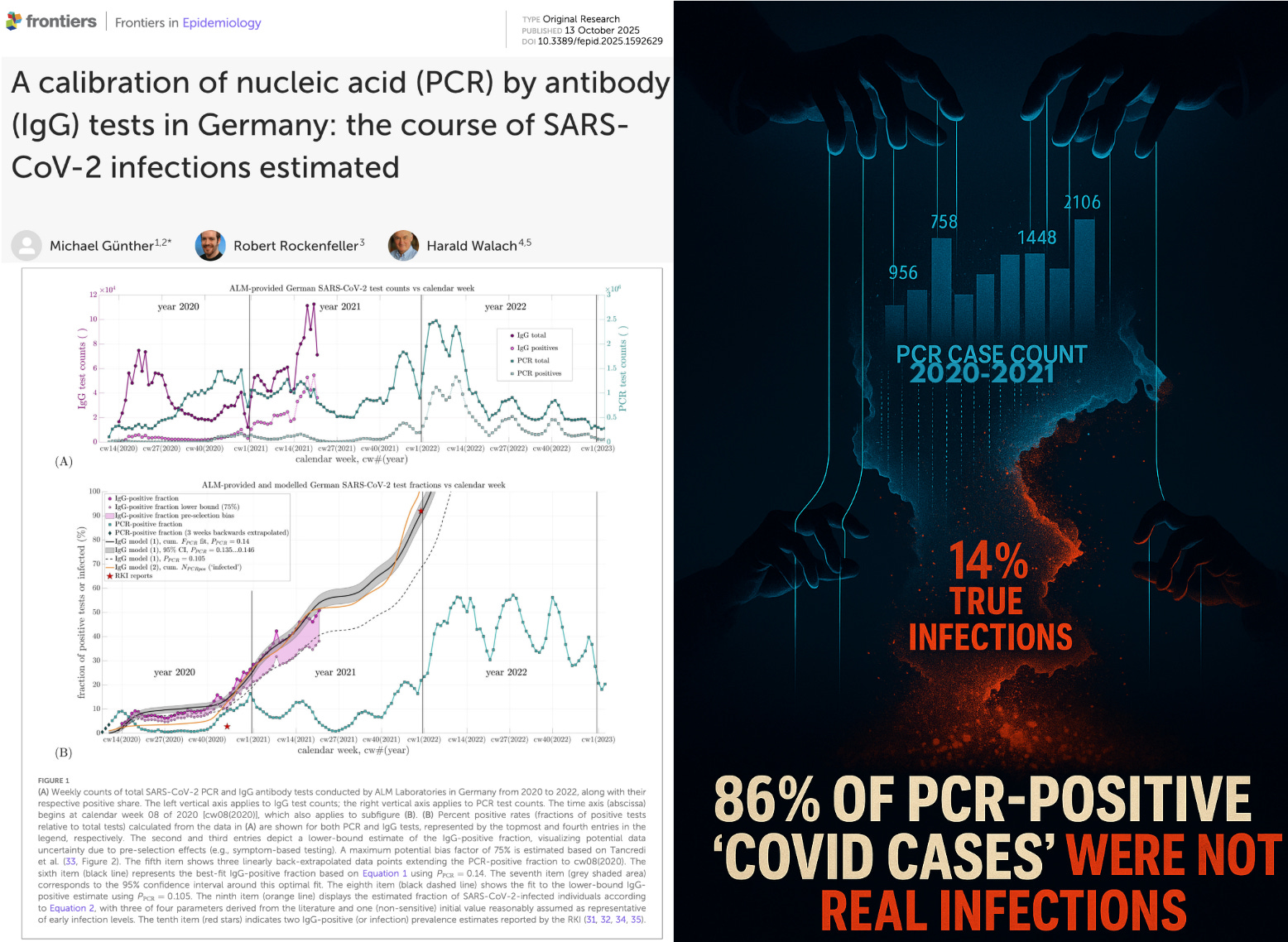
BREAKING: 86% of PCR-Positive “COVID Cases” Were Not Real Infections
New study finds that during the early pandemic period, only 14% of PCR “COVID cases” were real — proving that lockdowns and vaccine mandates were built on a fraudulent testing illusion.
A bombshell peer-reviewed study out of Germany just dismantled the scientific foundation used to justify lockdowns, social distancing, and vaccine mandates.
Researchers analyzed data from the Akkreditierte Labore in der Medizin (ALM) — a nationwide consortium of authority-accredited medical laboratories that performed roughly 90% of all SARS-CoV-2 PCR tests in Germany between 2020 and 2023.
When researchers compared the ALM’s week-by-week PCR positivity rates with the same labs’ IgG antibody testing data — essentially measuring who truly developed infection-induced immunity — they discovered something staggering:
Only about 14% of those who tested PCR-positive during the early pandemic period (2020–mid-2021) actually developed antibodies — meaning most early “cases” were never real infections.
Even under the most conservative assumptions — correcting for possible overrepresentation of IgG-positive individuals in the sample — the true infection fraction fell to roughly 10%, implying that nearly 90% of PCR positives were false or non-infectious detections, often just residual RNA fragments amplified at CT thresholds of 35–45.
What This Means
Mass PCR testing grossly inflated case numbers worldwide. Every nation that used similar CT thresholds likely overcounted “infections” by an order of magnitude.
Lockdowns and mandates were built on a false metric. The German “7-day incidence” used to trigger restrictions was statistically meaningless — and identical logic applied in the U.S., U.K., and elsewhere. In America, the entire “15 Days to Slow the Spread” campaign was predicated on the same inflated PCR scam.
Authorities suppressed representative serology data. Germany’s RKI and Ministry of Health had access to these ALM antibody results but never disclosed them — despite their policy relevance.
Rewriting pandemic history. If only 10–14% of reported PCR “cases” during the first year reflected true infections, then the infection-fatality rate, transmission models, and emergency declarations were all built on sand. By the end of 2020—months before vaccination began—roughly one-quarter of Germany’s population already carried natural antibodies. In other words, while authorities were declaring an uncontrolled crisis, herd-level immunity was already taking shape. By late 2021, nearly the entire population was IgG-positive. The evidence shows that pandemic policy was driven not by infection reality, but by a diagnostic illusion.
PCR technology and testing thresholds were standardized across WHO member states.
That means the same distortion likely occurred everywhere — a systemic diagnostic inflation that may be the single greatest fraud in public health history.
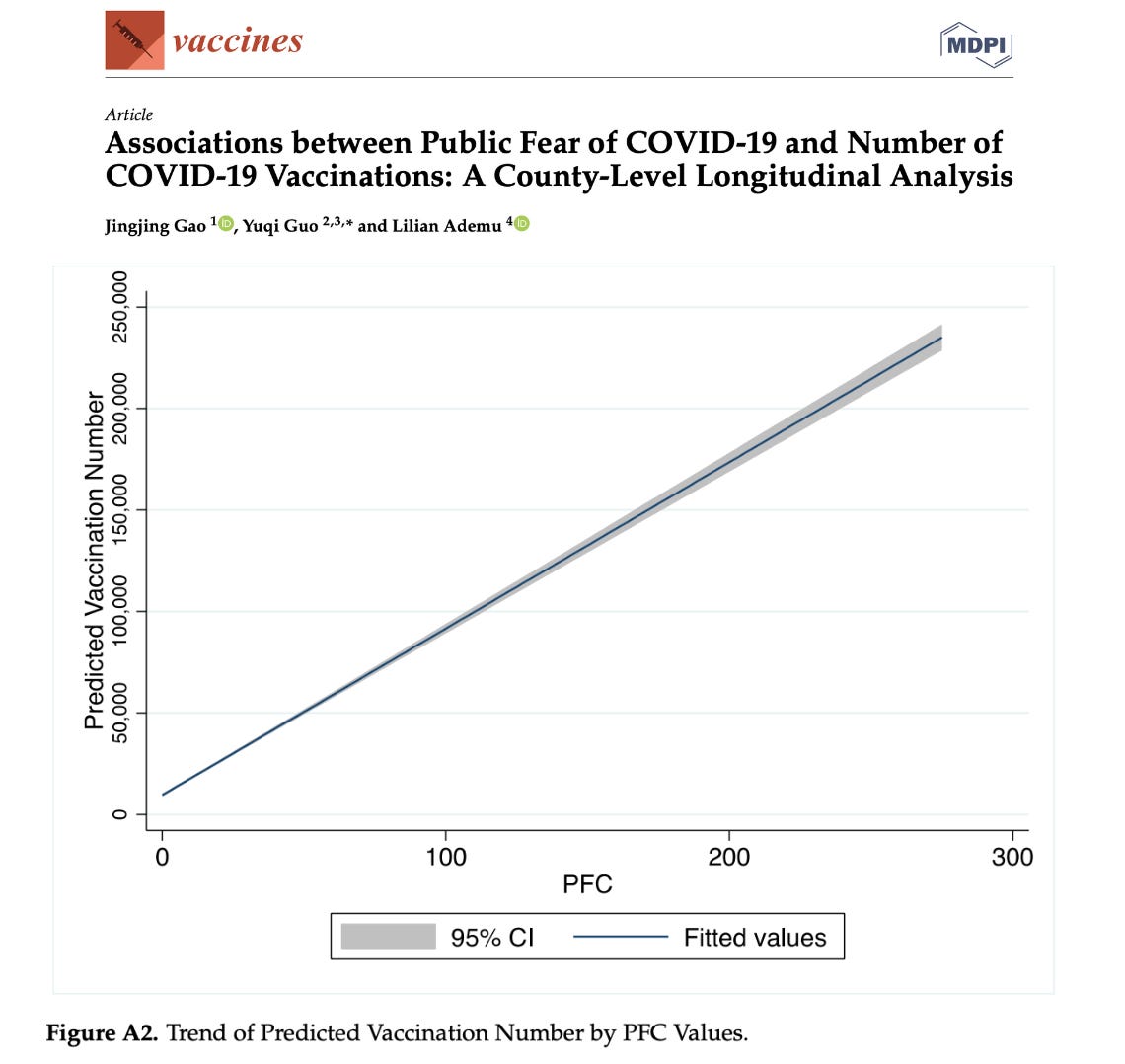
These tactics were likely used to amplify fear in order to boost compliance with lockdowns and experimental gene-based “vaccines.” This was demonstrated by Gao et al, who found that public fear of COVID-19 (PFC) was positively associated with the number of COVID-19 vaccinations at county-level: “as PFC increases from 0 to 300, the predicted vaccination number increases from 10,000 to 230,000.”
This is in line with fraudulent attempts to artificially increase COVID-19 death counts. Basoulis et al found that 45.3% of “COVID-19 deaths” in Greece were not actually due to COVID-19:
BREAKING — Nearly Half of “COVID-19 Deaths” Were Not Due to COVID-19, New Study Finds
In the end, most of the population did encounter the manufactured virus and develop antibodies—but the PCR data that justified global lockdowns, fear, and vaccine mandates were a complete fraud. Accountability is warranted.
Today, together with Dr. Marco Alessandria, Dr. Giovanni Trambusti, Dr. Giovanni M. Malatesta, and Dr. Alberto Donzelli, we published an crucial peer-reviewed scientific study titled “Classification bias and impact of COVID-19 vaccination on all-cause mortality: the case of the Italian Region Emilia-Romagna” [1]. In this study, we provide the first peer-reviewed evidence, based on real-world data, demonstrating how certain statistical methods have led to an overestimation of the effectiveness and safety of COVID-19 vaccines. This paper will shock the world, because it proves that all scientific studies conducted so far that are affected by this bias should be reassessed.
We addressed a critical bias that can substantially distort real-world evaluations of vaccine effectiveness and safety, known as the “case-counting window bias”. This bias, theorized by Fung et al. [2], occurs because individuals are classified as “unvaccinated” during the first 14 days after receiving the vaccine (the period believed necessary for the immune response to develop fully). As a result, any adverse events, including deaths during this time, are incorrectly attributed to the unvaccinated group, artificially inflating its mortality rate, while simultaneously underestimating mortality among vaccinated individuals.
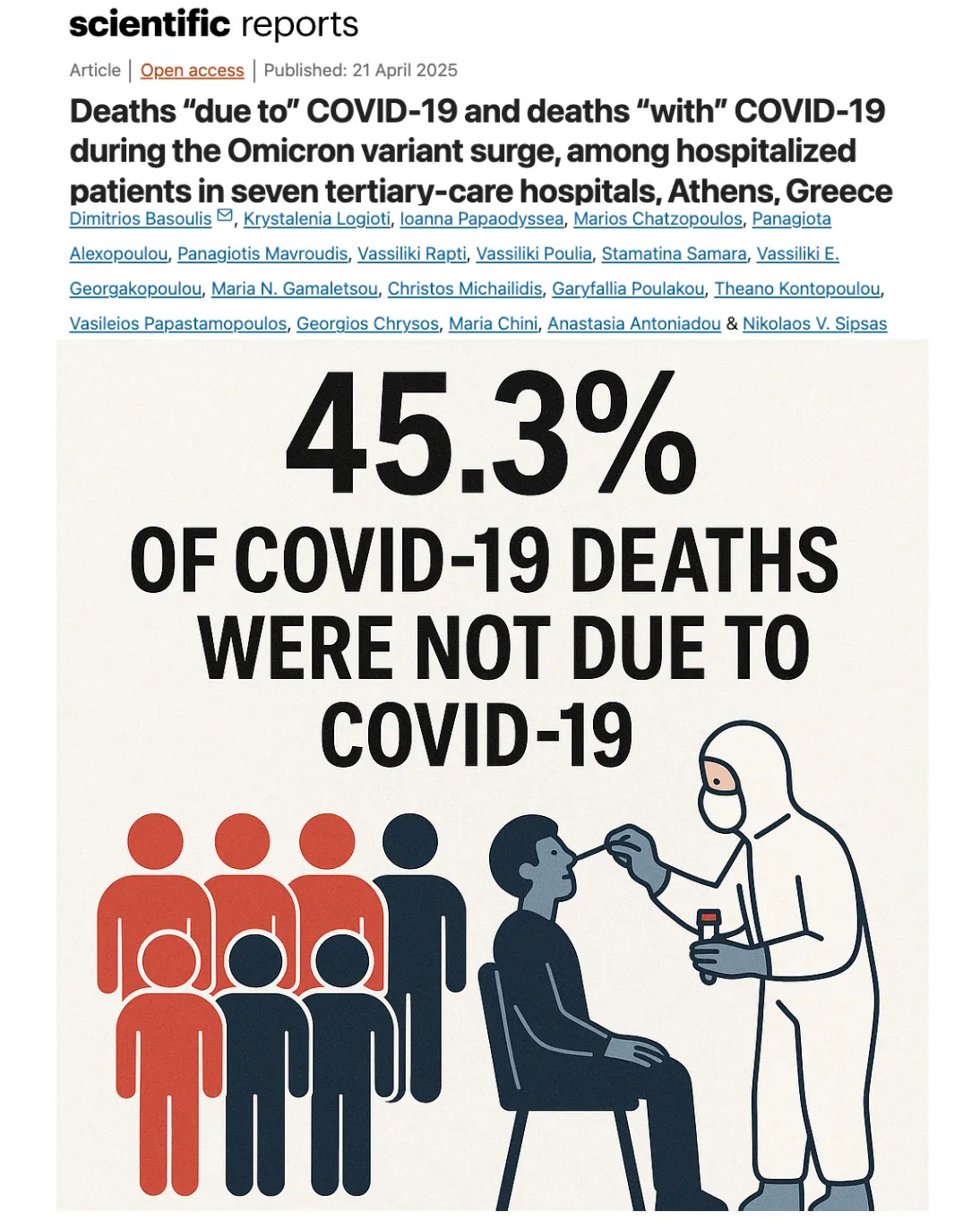
By analyzing detailed daily data on all-cause mortality and vaccine administration in the Emilia-Romagna region (Italy), obtained through a FOIA request by lawyer Lorenzo Melacarne (in accordance with the art. 5, comma 2 of the Italian Legislative Decree No. 33/2013), we found a clear temporal coincidence between vaccination campaigns and spikes in deaths among those incorrectly classified as unvaccinated during this critical window (Figure 1).
Figure 1. The chart illustrates the daily mortality rate per 100,000 individuals (age group 70-79), comparing those vaccinated (represented by the solid red line) with those unvaccinated (shown by the solid green line). Additionally, it shows the cumulative number of vaccinations administered with at least one dose (indicated by the red dotted line) [taken from Alessandria et al., 2025].
Our statistical analysis demonstrated significant differences in mortality between vaccinated and unvaccinated groups, during the critical 14-day post-vaccination window when misclassification occurs. Importantly, these mortality differences cannot be explained solely by COVID-19 deaths, which accounted for only about 9% of all deaths in Italy in 2021. Even after excluding COVID-19-related deaths, the disparity between groups remained significant, indicating systematic misclassification rather than true vaccine benefit. We also observed that the difference diminished with age, likely reflecting the increased comorbidity burden in older individuals that influences overall mortality risk (for more detailed information, please see the article, which is published in open access format and freely available to everyone).
Our findings suggest a harvesting effect, whereby vulnerable individuals succumb shortly after vaccination, but their deaths are wrongly counted among the unvaccinated.This misclassification masks potential serious vaccine-related adverse events occurring shortly post-vaccination, such as severe allergic reactions, cardiovascular events, or autoimmune responses. (See link for article)
Go here for this ‘must see’ clip of Del Bigtree stating:
“We’re injecting our kids with aborted fetal DNA, chopped-up organs from 3-month-old babies—76 in one study—admitted by vaccine chief Stanley Plotkin himself.
Monkey kidneys, hamster cells, cancer lines, mercury, formaldehyde… it’s a cauldron of horrors even Shakespeare couldn’t imagine.
And the worst part?
They admit: ‘We never studied this. We don’t know what it does.’
This isn’t science—it’s a witch cult.”
Dr. Suzanne Humphries who was raked over the coals for even daring to question the ‘vaccine’ religion states:
“Vaccination Introduced Animal Infections into Humanity.” Source
Wakefield also directed the documentary “Protocol 7,” which exposes real-life events of an actively litigated case in the 3rd Circuit Court of Appeals against Merck for fraudulent activity behind the MMR vaccine. The vaccine fails to protect against measles, destroys natural immunity, and the CDC admits as many as 94% of children who contracted mumps were vaccinated. Go here for a scientists rebuttal to the Danish MMR vaccine cohort study.
The Merck case was managed to largely avoid public scrutiny, despite its outcome being very much in the public interest. The film script was written years ago but they sat on it waiting for the court case to be resolved.
The case documents were sealed until recently. They are now being unsealed, albeit in a piecemeal manner. Available documents, including complaints, expert opinions, deposition testimony etc can be found here, which shows the actual fraud was much, much worse than what is presented in the film.
CDC scientist William Thompson admitted scientists purposely destroyed data.
“The omitted data suggested that African-American males who received the MMR vaccine before age 36 months were at increased risk for autism.” Dr. William Thompson
“Decisions were made regarding the findings of the report that the data was collected and I believe that the final study protocol was not followed.” Dr. William Thompson Source
Thompson ONLY came forth with this AFTER he was secretly recorded by Dr. Brian Hooker, a father of a vaccine injured child.
Thompson handed over documents about this case to Congressman Bill Posey.
Within the video Posey speaks before Congress about how not only did the authors of the study withheld vital information, they destroyed evidence. Source
Before reading the following unbelievably detailed analysis that took the author and his team over 3 years to complete, it’s important to note that ‘the powers that be’ aren’t getting the memo. Bill Gates recently had two meetings at the White House with President Trump and not only wants to inject cows and start putting scary additives into their food to supposedly reduce methane, but he’s funding a new micro-needle patch implant that installs both mRNA and quantum-dot markings into the body. Dr. Jessica Rose has broken it all down here. Suffice it to say that it’s even worse than the mRNA shots. In Rose’s words:
[It] involves taking the N1-modified mRNA-LNP technology (Pfizer/Moderna idea) to the next level of crazy, in my opinion.
And, Moderna has just unveiled a new mRNA shot called ‘mNEXSPIKE’ which translated in Latin means ‘violent death, or ‘death spear.’ You seriously can’t make this up.
Does anyone else out there get the distinct impression they want us dead?
Headlines repeated around the world and more importantly by the regulators FDA, TGA, EMA and MHRA.
Just to reiterate – this was about COVID infection. No claims on severity, hospitalisation or death were made by Pfizer.
Given that most of the vaccinated population actually “got COVID” – many of them multiple times, that sounds impossible, right?
That’s because it was.
Yet the trial itself showed 95% reduction in the risk of infection and was published in the infamous New England Journal of Medicine (the same journal that published the fraudulentSurgisphere study) on the 10th December 2020.
….we are going to show that the whole study was a sham and that there never was a benefit – at all, never mind “95% reduction in infection.” (See link for article)
________________
**Comment**
I’m eternally grateful that researchers and doctors are now onto the prolific research fraud that has been taking place. Of course, this fraud has been going on in Lymeland for over 40 years, but now it’s on display for the entire world to see. Yet another silver lining that came out of COVID mania.
SUMMARY:
One of the main Pfizer hustles was mandating all PCR swabs for the trial be sent to their own lab in New York as part of the case definition. Which means that Pfizer decided whether a swab was positive or negative – the only test that mattered.
We only know this is due to a FOIA by attorney Aaron Siri. Pfizer and the FDA tried to withhold this intel for 75 years.
Another hustle concerns dates. The cut off for the trial was Nov. 14, 2020. The VRBPAC meeting was on Dec. 10, 2020, the same day the trial was published. The VRBPAC assessment document for the Pfizer submission was written on Dec. 7, 2020, just two weeks after the submission – having to assess 44,000 participants. The approval was made on the basis of 47 days of follow-up for most patients, but was also made in ONE DAY, because of the VRBPAC meeting on Dec. 20, 2020 – with EUA declared on Dec. 11, 2020. Certainly a miracle.
The dates demonstrate that all of this was impossible, which implies it was a pre-agreed approval based upon Pfizer showing data that there were less infections in the ‘vaccinated’ group based on a test they controlled – not on clinical symptoms.
Evidently, Doran Fink of the FDA presented in the VRBPAC meeting despite having no clinical data and no experience in handling large data sets. Unblinding in the trial was not allowed to happen until after Nov. 14, 2020, yet somehow Pfizer knew what was in which arm before that date. Interestingly, Fink was then given a job at Moderna and now is at GSK, demonstrating clearly the revolving door between the FDA and Big Pharma.
Even more miraculously Pfizer, the WEF, and mainstream media already knew by the 9th of November that the ‘vaccine’ had ‘worked’ despite the fact the data cut off was Nov. 14.
Susan K Wollersheim’s ability to give the statistical presentation for VRBPAC on a 44,000 participant clinical trial is legendary as she has never published a clinical research study7.
There is no way Fink and Wollersheim did the analysis as they don’t have the skill set and they didn’t have the time necessary to do it.
The good doctor who authored this article, Dr Ah Kahn Syed, states that it took him and a handful of people with the skillset required 3 years to sift through over 2 MILLION pages of FDA documents to just write this article.
Moderna achieved a similar EUA approval only 7 days later due to a similar hustle.
The third hustle: they stopped accumulating cases (in the “vaccinated group” only) for a specified time period in order to make the cut.
A tactic they probably used, since they solely controlled testing, was to change the Cycle threshold on the machine recording the tests. A Ct of over 40 will pick up a bunch of false positives and a low Ct of less than 16 will only pick up real cases with a high viral load. They didn’t know the ‘sweet spot,’ so they had to change Ct as they went along. The field that should have recorded the Ct on the machine is conveniently missing.
Pfizer knew which tests were from the ‘vaccinated’ or the placebo group because they had the blood tests from every person in the study at their lab. Castruita showed in 2023 that even after 4 weeks there was enough circulating RNA (or DNA) from the COVID-19 vaccines to be able to perform genomic sequencing13. While unlocking the database would create audit flags, they could easily identify who got what without raising audit flags, so they could then adjust the Ct up or down depending upon the number of positive tests they needed.
The author proves that if you correct for the fact that, if you’re vaccinated, you have 2.3x less chance of showing N-antibody on a test, the infection rate of the ‘vaccinated’ and of the placebo group is identical. There was no 95% reduction in infection in the ‘vaccinated’ group at all. It was a scam.
The author also shows from The FDA’s review that there were over 1100 more fevers and over 2000 more reports of chills in the ‘vaccinated’ group.
Sadly, all of this should have been done before ‘Operation Warp-speed,’ but let this be a solid reminder to not take ANYTHING until you are fully convinced it truly works and is safe. In short, do not believe anything the medical machine for profit says. Before you take anything they recommend, wait until independent research has been done.
There are probably many, many people who are now living with a lot of regret.
Danielle Jonas, wife of Kevin Jonas, is revealing the stressful symptoms that led to her recent diagnosis of Lyme disease.
Jonas, 39, sought treatment when she noticed that she was shedding more hair than usual.
“They tried to tell me it was anxiety. Finally, I had a biopsy that showed I actually had Lyme disease,” Jonas said in an interview with Parents publishedon Thursday….
Years before the Lyme diagnosis, Jonas had experienced symptoms of eczema. They seemed to worsen during this new health battle. (See link for article)
______________
**Comment**
Jonas’ children also suffer from eczema and other skin issues.