
Pharma-Sponsored Media Launches Measles Fear Campaign Based on Distorted Science
UPDATE:
Numerous deaths have now occurred after the MMR vaccine, but the emphasis is always placed upon the virus.
- Stanford scientists confirm a fatal case of vaccine-associated measles encephalitis in an immunocompromised child.
In this case, the vaccine measles virus hypermutated to a fatal strain that invaded the brain and killed the child.
If the child was unvaccinated, the AML would have been treated in the usual fashion, with a good chance at survival. Source
- International news sources pounced when a 6-year old Texas child died. They blamed the fact she was unvaccinated, but the true cause of death was multiple co-existing respiratory illnesses.
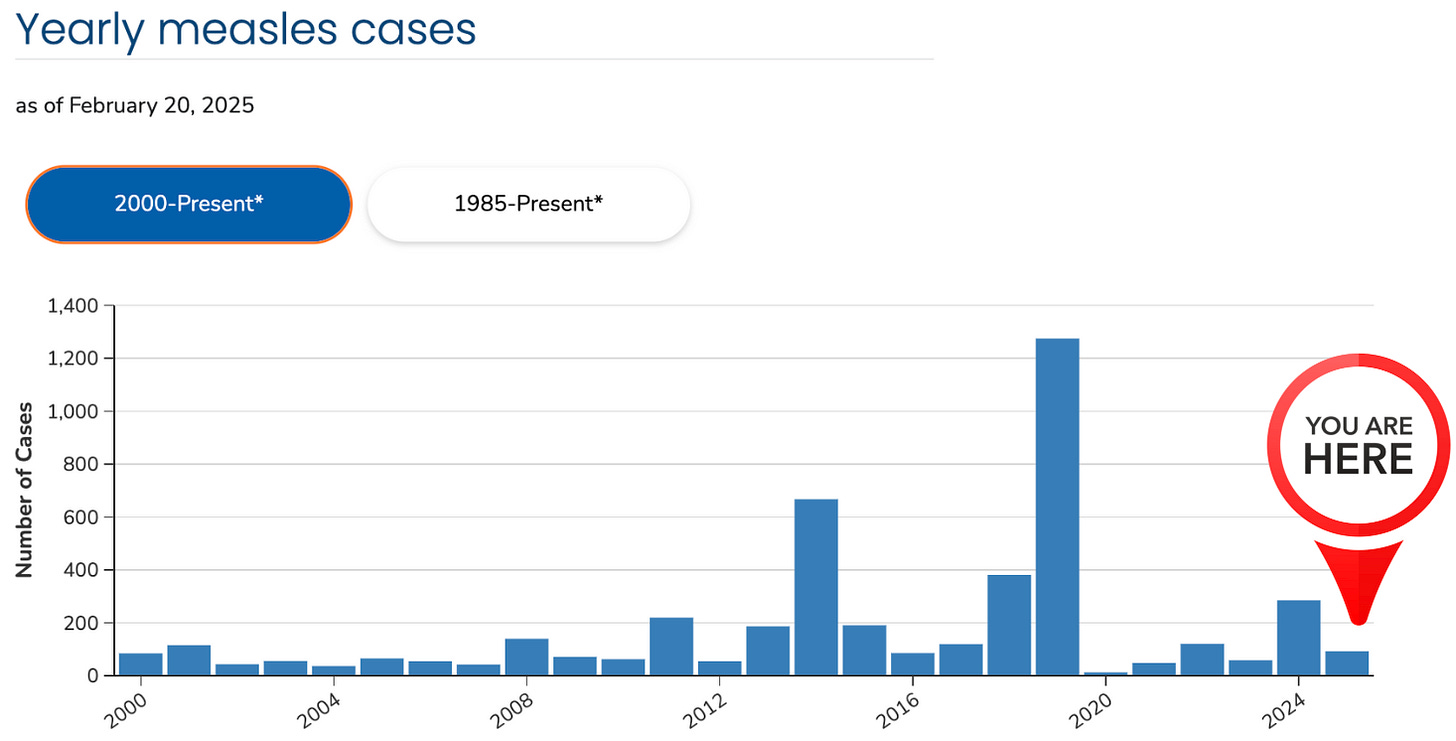
Measles outbreaks occur every year across the U.S. despite 90.8% MMR vaccine uptake.
- It’s easy for the media to push measles fear porn due to the fact the CDC obfuscates vaccine data by classifying 95% of measles cases as ‘unvaccinated or unknown’– two fundamentally different categories.
Truth be told, measles cases with unknown vaccination status may in fact be vaccinated.
- The CDC purposely merges unknown cases with unvaccinated ones maximizing the association between measles cases and non-vaccination while obscuring uncertainty in the data. It purposely does not apply the same logic in reverse – merging ‘unknown cases with vaccinated cases maximizing the association between measles cases and vaccination, which very well could be true.
This allows them to smugly reinforce a predetermined narrative.
You won’t hear these little factoids from mainstream media.
https://www.thefocalpoints.com/p/pharma-sponsored-media-launches-measles?
Pharma-Sponsored Media Launches Measles Fear Campaign Based on Distorted Science
Media-driven panic over measles ignores real risks, natural disease patterns, and the role of vaccine shedding.
A google search for ‘measles’ reveals the coordinated fear campaign propagated by pharma-sponsored mass media:
Is there a reason to cower in fear as the news suggests and rush to get MMR booster shots? No, especially not for healthy children. However, we must remember that children with multiple comorbidities can face serious outcomes, as with any disease. It’s important to approach these discussions with a level-headed assessment of individual risk rather than reacting to sensationalized headlines.
Measles outbreaks occur every year across the United States despite 90.8% MMR vaccine uptake:
Shedding of measles vaccine RNA is a recognized phenomenon, with detectable levels in nasopharyngeal samples for up to 29 days post-vaccination (Washam et al). This shedding results from the replication of the attenuated vaccine virus, which can be transmitted to close contacts. (See link for article, studies, and graphs)
_______________
Important point:
A study by Miller, published prior to the introduction of the measles vaccine—found for measles:
- hospitalization rate of 11.5 per 1,000 cases
- mortality rate of 0.2 per 1,000 cases
In comparison, seasonal influenza:
- hospitalization rate of 10–20 per 1,000 cases
- mortality rate of 0.5–2 per 1,000 cases
Dissolving Illusions by Bystrianyk and Humphries indicates that measles-related deaths in children are overwhelmingly linked to malnutrition and vitamin A deficiency.
Please also recognize the scam of media reports using a positive test rather than cause of death. Testing positive means little as we saw with COVID. People tested positive and didn’t have ANY symptoms whatsoever.
Just like the COVID shot the measles vaccine does not protect against infection and destroys natural immunity.
For more:
-
https://madisonarealymesupportgroup.com/2020/05/07/was-the-covid-19-test-meant-to-detect-a-virus/ Excerpt:
I’m skeptical that a PRC test is ever true. It’s a great scientific research tool. It’s a horrible tool for clinical medicine. Dr. David Rasnick, bio-chemist, protease developer, and former founder of an EM lab called Viral Forensics https://madisonarealymesupportgroup.com/2020/05/07/was-the-covid-19-test-meant-to-detect-a-virus/





